
Abstract
Purpose:
The aim of this study was to compare the biomechanical properties between the suture fixation technique and the screw fixation technique for tibial eminence fracture (TEF).
Methods:
The current study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The PubMed, Embase, and the Cochrane were searched from inception to January 2019 comparing the suture and the screw fixation technique for TEF. The results of the eligible studies were analyzed in terms of stiffness, ultimate failure load, and displacement after the cyclic testing.
Results:
Six laboratory studies were included with a total of 114 knees: 57 knees were in the FiberWire suture group and 57 knees were in the single-screw group. The suture group had higher stiffness than the screw group, but there was no statistical difference between these two groups. Ultimate failure load in the suture group was statistically higher than that in the screw group. No statistically significant difference existed in displacement after the cyclic testing between the suture group and the screw group.
Conclusion:
The FiberWire suture fixation may be biomechanically superior to a single screw fixation in TEF treatment in mature knees regarding ultimate failure load, while no significant difference was found between the two fixations in terms of stiffness and displacement after the cyclic testing.
Introduction
Tibial eminence fracture (TEF), also known as anterior cruciate ligament (ACL) avulsion fracture, 1 –3 is common in people with immature skeleton during exercise, 4 yet it can also occur in skeletally mature population because of high-energy mechanisms. 5 Such fracture can lead to joint instability, pain, and loss of knee extension secondary to displacement of fracture segments. 1,2 Consequently, it is crucial and necessary to reestablish the biomechanics by anatomical reduction and internal fixation. 6
Multiple surgical methods, including open techniques and arthroscopic techniques, have been described in TEF treatment. Nowadays, arthroscopic treatment is considered to be the gold standard 6 –8 and has replaced open techniques, which have a higher incidence of postoperative complications. 2,9 –11 Additionally, there are many different arthroscopic fixation techniques for the treatment of TEFs. 7,8,12 –17 Suture fixation and screw fixation are commonly used arthroscopic techniques to promote fracture healing and to reduce joint relaxation. 18 –21
Screw fixation has advantages in direct reduction and compression for large, complete fractures without interfering with the growth plate, 1,22,23 while suture fixation can be used in all types of fractures including comminuted fractures. 15,24 However, there is still no consensus as to which technique is superior in biotechnical properties for TEF treatment. Senekovic and Balazic 25 reported that arthroscopic fixation with sutures of TEF is even more reliable than that with the cannulated screws and washers. Moreover, no second operation is necessary for screw fixation. However, Tsukada et al. 26 performed a cadaveric biomechanical analysis and found that screw fixation had a slight biomechanical advantage over suture fixation in biomechanical property. Besides, Mahar et al. 27 found no significant difference between the suture and screw fixation in TEF treatment in biomechanical analysis.
Since the sample size is small in the above studies and the conclusions are inconsistent, it is imperative and crucial to pool relevant data to make the comparison more objective and accurate. In our present meta-analysis, only laboratory studies were included to compare the biomechanical outcome between the FiberWire suture fixation and the single screw fixation in the treatment of TEF. We hypothesized that the FiberWire suture fixation could provide better biotechnical properties than the single screw fixation during early rehabilitation. Additionally, we hope that this article could provide theoretical support for clinicians to choose appropriate fixation technology in TEF treatment and provide reference for their later clinical research.
Materials and methods
Search strategy
The present study was conceived and implemented according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 28 PubMed, Cochrane Library, and Embase databases were searched from inception to January 2019. A manual search of all reference lists contained in the literature was also conducted. Medical subject headings, titles as well as abstracts were searched for the keywords: Biomechanical AND (“Tibial Eminence Fracture” OR “anterior cruciate ligament avulsion fracture” OR “tibial avulsion fractures of the anterior cruciate ligament” OR “Tibial Eminence Fractures”).
Inclusion criteria and exclusion criteria
Inclusion criteria were as follows: (1) intervention method—comparison of biomechanical outcome between the suture fixation and screw fixation technique for TEF; (2) outcome parameters—stiffness, ultimate failure load, displacement after the cyclic testing; (3) study objective—porcine knees or human cadaveric knees; and (4) study type—laboratory studies.
The exclusion criteria were the following: (1) clinical studies or other animal studies; (2) not FiberWire suture in the suture fixation technique; and (3) two or more screws in the screw fixation technique.
Literature selection
All possible studies were imported into the Endnote and duplicates were excluded. Then, irrelevant studies were excluded by two researchers independently based on titles and abstracts. Finally, after reading the full text cautiously, the studies that did not satisfy the selection criteria were eliminated. Disagreements were resolved by discussion between the two researchers.
Data extraction and assessment of study quality
All potentially eligible studies were checked by two researchers independently using a predesigned table to perform data extraction. Extracted data included article information (author and publication date), sample size, the age of samples, sample type, fracture size, fracture type, and outcome parameter.
Study quality of the included studies was assessed by the same two researchers independently according to the Stroke Therapy Academic Industry Roundtable (STAIR) list, 29 which comprises seven items. In this list, the following seven items were assessed in all included studies: (1) sample size calculation, (2) inclusion and exclusion criteria, (3) randomization, (4) allocation concealment, (5) reporting of animals excluded from analysis, (6) blinded assessment of outcome, and (7) reporting potential conflicts of interest and study funding. Each item was scored yes or no, with a maximum score of 7. A trial with a score of ≥5 was considered to be of high quality.
Statistical analysis
Stata/SE version 12.0 was used for the present meta-analysis. Relative risk was used for analysis for dichotomous outcomes. A weighted mean difference (WMD) was calculated for continuous outcomes when the same measurement criterion was used; otherwise, a standardized mean difference was calculated. Both used 95% confidence intervals (CI). The statistical heterogeneity was tested with the χ 2 test and I 2. A fixed-effects model was used when heterogeneity was low (p > 0.1 or I 2 ≤ 50%). However, when heterogeneity was significant (p < 0.1, I 2 > 50%), sensitivity analysis, subgroup analyses as well as meta-regression were conducted to find the source of the heterogeneity. If the heterogeneity could not be eliminated, a random-effects model would be used or descriptive analysis was used. Begg’s test was used to check the publication bias of involved articles.
Results
Search results
Forty relevant articles were firstly selected according to the search strategy. Seventeen were excluded after duplicate checking. Twelve were excluded after reading the titles and the abstracts, including six studies not about suture versus screw fixation, five studies not about biomechanical comparison, and one study using specimens from bovine knees. Finally, six articles were included in this meta-analysis. A summary of the review process is presented in Figure 1.

Flowchart of article selection process.
Description of included studies
All six selected articles 1,6,25,30 –32 compared the biomechanical outcomes of the suture and screw fixation techniques in the treatment of TEF. The specimens were all from porcine knees or cadaveric knees with different fixation methods. There were 114 patients in total: 57 knees were in the suture group and 57 knees were in the screw group. All basic information of this article is presented in Table 1 and the outcome measures of the two fixation techniques are reported in Table 2. All of the six selected articles were laboratory studies and assessed using the STAIR list. The results showed that all articles scoring ≥5 were of high quality. The methodological score of each included study with general remarks is shown in Table 3.
Description of the included studies.
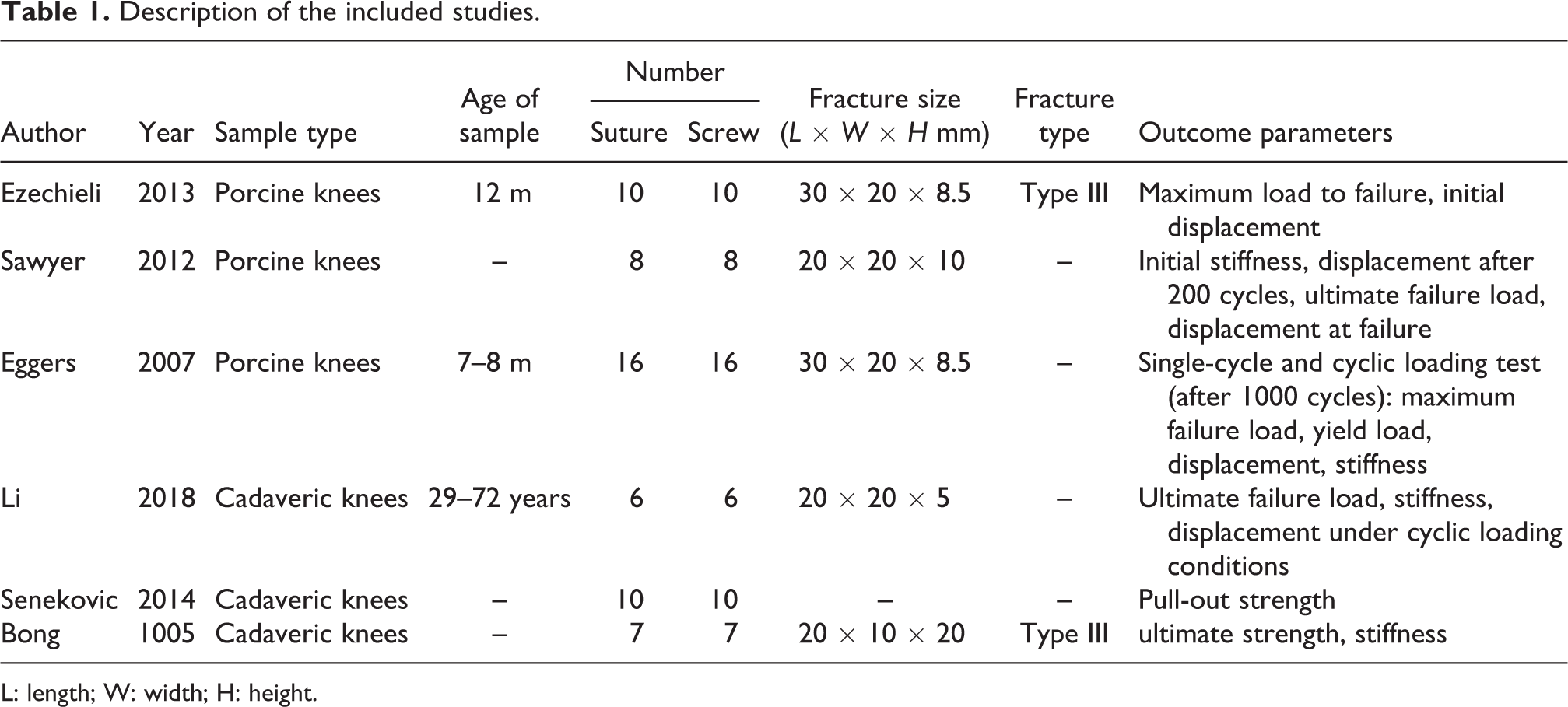
L: length; W: width; H: height.
Outcome measures of suture group versus screw group.

STAIR list.a

✓, satisfied criterion; ✗, did not satisfy criterion. STAIR: the initial stroke therapy academic industry roundtable.
a Criteria: 1. sample size calculation; 2. inclusion and exclusion criteria; 3. randomization; 4. allocation concealment; 5. reporting of animals excluded from analysis; 6. blinded assessment of outcome; and 7. reporting potential conflicts of interest and study funding.
Stiffness
Four studies reported stiffness, and obvious heterogeneity was found among these studies (p = 0, I 2 = 85.2%). Using the random-effects model in the analysis, with 37 knees in suture group and 37 knees in the screw group, the results showed no significant difference in any adverse events between the two groups (WMD = 11.85, 95% CI (−2.4, 26.1), p = 0.103). Subgroup meta-analysis based on different specimens demonstrated that initial stiffness in the suture group was greater than that in the screw group in both porcine knees and cadaveric knees. However, there was no significant difference between the two groups (WMD = 14.53, 95% CI (−2.16, 31.22), p = 0.088; WMD = 16.58, 95% CI (−21.11, 54.28), p = 0.389, respectively) (Figure 2).

Forest plot of stiffness.
Ultimate failure load
Six studies included ultimate failure load with heterogeneity being found among the studies (p = 0, I 2 = 90.7%). Using the random-effects model, 57 knees in the suture group and 57 knees in the screw group were analyzed, and a significant difference was found between the two methods (WMD = 128.2, 95% CI (60.7, 195.7), p = 0). Subgroup meta-analysis based on different specimens demonstrated that ultimate failure load in the suture group was greater than that in the screw group in both porcine knees and cadaveric knees. However, there was a statistically significant difference between the suture group and the screw group in cadaveric knees (WMD = 149.4, 95% CI (61.3, 237.4), p = 0.001), while there was no significant difference between the two groups in porcine knees (WMD = 102, 95% CI (−44.99, 248.9, p = 0.174) (Figure 3).

Forest plot of ultimate failure load.
Displacement after the cyclic testing
Two studies included displacement after the cyclic testing, and obvious heterogeneity was found among the studies (p = 0.086, I 2 = 66%). The 24 knees in the suture group and 24 knees in the screw group were analyzed using the random-effects model. The result showed no difference in displacement between the two groups (WMD = 0.08, 95% CI (−2.45, 2. 61, p = 0.95) (Figure 4).

Forest plot of displacement after the cyclic testing.
Publication bias
For ultimate failure load, used as an indicator in most studies as an example, Begg’s test was used to access the publication bias, showing the lack of bias among the included studies (Begg’s test, p = 1, Figure 5).

Funnel plot of publication bias for ultimate failure load.
Discussion
TEF is a rare knee injury, 33 and no randomized controlled test until now reported the comparison of different fixations. A systematic review of Gans et al. 34 identified 26 studies with extractable clinical results, however, most of the included studies were level 4 articles. There is insufficient evidence to conclude the superiority of suture versus screw fixation techniques. Similarly, Coyle et al. 35 in another review failed to show any conclusive evidence that any method was superior to the others. It may be necessary and significant to compare the biological properties of the suture fixation and screw fixation for TEF, thus providing reference for their future clinical research.
This is the first meta-analysis that has compared the biomechanical outcomes of suture fixation and screw fixation for the treatment of TEF. A total of six studies, including 114 knees were included in the integrated analysis. The evidence from the current study suggests that the FiberWire suture fixation seems to be a superior fixation with regard to significantly higher ultimate failure load compared with the single screw fixation for TEF treatment. However, there is no statistically significant difference between the suture fixation and the screw fixation in stiffness and displacement after the cyclic testing.
Stiffness represents the quality of the initial fixation structure, 30 and a more rigid suture material showed superior structural properties than a less rigid suture. 31 In the present study, compared with the screw fixation, the suture fixation had higher stiffness, but there was no statistically significant difference between these two methods. Among the included studies, Sawyer et al. 30 and Li et al. 1 reported that stiffness is similar using both the suture fixation and the screw fixation. However, Eggers et al. 31 and Bong et al. 32 found that stiffness in the suture fixation method was significantly higher than that in the screw fixation method for TEF treatment.
Ultimate failure load is used to measure the top limit of the graft fixing structure, which reflects the potential for the graft to bear a sudden trauma during the recovery period. 31,36 In the treatment of TEF, the fixation with a higher ultimate failure load may allow for more aggressive rehabilitation protocols and minimize complications followed by long-term fixation after surgery. The results of this study showed that the FiberWire suture fixation provided superior fixation with regard to higher ultimate failure load compared with the single-screw fixation in TEF treatment. Based on the results of subgroup analysis, we found that there was a significant difference in cadaveric knees, but not in porcine knees. In our study, all the porcine knees were skeletally immature models, while cadaveric knees were mature models. This may mean that the FiberWire suture may allow for more aggressive rehabilitation protocols than screw in adult patients, while the ability to face the unexpected injuries is similar between the two groups in children or adolescents. 37
The displacement is used to quantify the loss of graft fixations and compare the initial stability of different fixation techniques. Furthermore, it represents the ability to provide a stable initial fixation. The cyclic loading was intended to simulate an early rehabilitation process including continuous passive motion and partial weight bearing. 38 In the meta-analysis, there was no significant difference between the two fixations in displacement after cyclic testing, which indicated that these two techniques are comparable at withstanding an early rehabilitation and recovery process. The result was in line with some previous studies. 1,30 However, Eggers et al. 31 reported that displacement after cyclic testing in FiberWire suture fixation was statistically lower than that in the screw fixation.
The advantages of this study were as follows. Firstly, only studies of FiberWire suture fixation versus single screw fixation were included in the present meta-analysis. Some factors, including suture material and numbers of screws, can increase the heterogeneity of results. It is known that the structural properties of suture fixation depend strongly on the suture material used to fix the fracture. 31 Both Lo et al. 39 and Wust et al. 40 reported that FiberWire sutures had improved biomechanical properties compared with Ethibond sutures in arthroscopic repairs. Similarly, Eggers et al. 31 demonstrated that single-screw fixation exhibited superior maximum failure load compared with screw fixation with two screws. All of the included articles used the same technique for fixation. The FiberWire suture was used for suture fixation, and the single cannulated screw was used for screw fixation. Secondly, all the specimens in the included studies were porcine knees or cadaveric knees, and studies with specimens from other animals were excluded. Since only few studies chose specimens from other animals 27 and outcome indicators in these animals were incomplete to conduct a meta-analysis. Finally, all the porcine knees were skeletally immature models, while cadaveric knees were mature models. Subgroup analysis was conducted according to the specimen sources, and the biomechanical properties between the suture fixation and the screw fixation were compared in porcine knees and cadaveric knees, as well as in immature knees and mature knees. Thus, the result of this meta-analysis is more objective and persuasive in the comparison of the two fixation techniques for TEF treatment.
Several limitations in this meta-analysis should be noted. Firstly, the whole sample size seems small. However, it may be large enough to provide a more comprehensive and objective evaluation of the two fixation techniques for TEF treatment, considering that the sample size in most experimental articles is relatively small. Secondly, outcome indicators like initial displacement and yield load were referred to respectively in only one of the included studies and could not be used as an outcome parameter in the present study. Finally, the study aims to compare the biomechanical properties without follow-up functional results. Further clinical studies comparing these fixation techniques may be needed in future research work.
Conclusion
The FiberWire suture fixation may be biomechanically superior to a single screw fixation in TEF treatment in mature knees regarding ultimate failure load, while no significant difference was found between the two fixations in terms of stiffness and displacement after the cyclic testing. These indicated that both of these two fixations could withstand an early rehabilitation and recovery process. However, the FiberWire suture fixation might be safer to bear a sudden trauma during the recovery period.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Hubei Province health and family planning scientific research project [Grant No. WJ2019Q051].