
Abstract
Introduction:
Hyalofast grafting with microfracture is a new minimally invasive treatment method being proposed for joint cartilage defects. This study was done to measure the clinical efficacy of Hyalofast grafting after microfractures.
Methods:
Forty-six patients were assessed for knee function using knee injury and osteoarthritis outcome score (KOOS) after undergoing microfracture and Hyalofast grafting surgery. We further divided the 46 patients into a group of 10 patients who had no associated procedures done with the microfracture and Hyalofast grafting surgery. All patients had magnetic resonance imaging (MRI) of the affected knee pre-surgery and two patients had MRI done post-surgery. Due to another unrelated injury, we were also able to obtain further arthroscopic findings of another patient’s knee 18 months after microfracture and Hyalofast grafting.
Results:
There was a statistically significant improvement in all categories of the KOOS (symptoms, pain, daily living, sports and quality of life) compared between years 1, 2 and 3 against pre-surgery. For the subgroup of Hyalofast only, there was a statistically significant improvement in symptoms, pain and daily living categories of the KOOS compared between years 1, 2 and 3 against pre-surgery.
Conclusions:
Our study shows that Hyalofast grafting after microfracture is a viable alternative to treatment for patients with grade 4 cartilage ulcers.
Keywords
Introduction
Knee pain is a common and often debilitating issue to many patients. This is especially seen in patients above 40 years old. Many patients present with acute severe knee pain on weight bearing and knee flexion due to degenerated or torn meniscus. However, the predominant cause of chronic knee pain is cartilage wear and ulceration. 1 This is particularly pronounced over the patellofemoral and medial tibiofemoral joint.
Articular cartilage plays an important role in absorbing stresses across the knee joint. 2 Unfortunately, due to these stresses, cartilage wear is inevitable. In 2001, it was estimated that 43 million adults in the United States suffered from arthritis. 3 Of those, 26.9 million adults had osteoarthritis 4 with one in four people expected to develop symptomatic osteoarthritis in their lifetime. 5,6
Pain from cartilage injury is often due to exposed bone pressing against each other. 7 Cartilage healing potential is feeble at best and often absent due to persistent friction across the joint. 8 This is due to joint malalignment or constant grating by a loose meniscus fragment. 9
Present-day solutions aim to reduce the wearing down of cartilage and promote cartilage healing. 2 Conservative measures include correcting malalignment issues with knee braces, foot orthotics and special shoes or off-loading the knee with walking sticks and crutches. 10 However, these solutions are usually not an acceptable long-term solution, especially for younger patients. Glucosamine has been touted to help cartilage regenerate but results from clinical trials have been mixed. 11 Medically, intra-articular injections with viscosupplementation and platelet-rich plasma therapy help to reduce intra-articular friction and regenerate cartilage. 12 However, these intra-articular solutions have limited effect when malalignment factors or large and deep cartilage defects are present. 13 Surgical management of arthroscopic debridement for knee osteoarthritis has been shown to have limited long-term beneficial effect. 14 Joint replacement surgery is an effective solution for painful arthritic knees but is an expensive and invasive procedure. 15 With its limited life span, joint replacement is not the best option for younger patients.
In recent years, Hyalofast, a bioscaffold that promotes new cartilage growth, has started to be offered as an alternative to manage painful arthritic knees. This case series was done to assess the outcome of managing osteoarthritic patients with grade IV articular cartilage ulcer, who failed conservative treatment, with the bioscaffold, Hyalofast.
Hyalofast is a non-woven 2 × 2 cm2 or 5×5 cm2 biodegradable hyaluronic acid (HA)-based scaffold for hyaline-like cartilage regeneration. Hyalofast entraps mesenchymal stem cells (MSCs) to treat both chondral and osteochondral lesions in the knee and ankle. Once implanted, it maintains its structure to support MSC attachment, proliferation and differentiation. This results in the complete filling of the lesion with new cartilage. As the Hyalofast scaffold degrades, it releases more HA into the lesion, resulting in an embryonic-like microenvironment that further promotes cartilage growth. 16
Methods
Forty-six patients with grade 4 cartilage ulcers underwent arthroscopic surgery after failed conservative treatment. All patients were routinely reviewed and their knee functional status before and after the procedure was evaluated using the KOOS score. Ethics approval was received from the Ethics Committee, Mount Alvernia Hospital Singapore. Verbal consent was received from all participating patients.
Surgical procedure
The surgery is done with patient under general anaesthesia with the usual aseptic knee arthroscopy procedure and equipment. Two parapatellar portals are used. Initial assessment of the joint is performed with special attention on meniscal tears, depth, site and size of cartilage ulcers as well as evidence of excessive patellar compression syndrome or tilt. Meniscus tears are treated with partial meniscectomy or repaired with fast-fix meniscal sutures. Excessive patellar compression or tilt is treated with lateral retinaculum release.
After noting the depth of the ulcer, loose cartilage edges will then be debrided with motorised shaver until a stable edge is obtained. The size of the ulcer is then measured with a probe. The base of the cartilage ulcer is microfractured until marrow contents are seen to ooze out. Hypertrophied synovium, especially synovium near the cartilage ulcer, will be debrided as it may occlude visualisation of the ulcer. The joint is lavaged and all bleeding points cauterised to ensure no active bleeding from synovium and lateral retinaculum. This is to ensure a dry field which enables a good visualisation of Hyalofast implantation.
The knee joint is then dried with the help of sucker and rolled up gauze or patties. Carbon dioxide is then pumped in through the cannula at 10 mmHg pressure at a flow rate of 7 l in a minute to distend the joint. The Hyalofast patch graft is cut with an additional 20% as the patch shrinks on contact with the marrow exudate. The patch graft is rolled up and introduced into the knee joint with a cannula made with a 3 cc plastic syringe with the end sawn off.
Once inside the joint, the rolled-up Hyalofast patch graft is unfurled with the help of a needle and McDonald’s dissector. The patch graft is then press-fitted into the ulcer with the McDonald’s dissector. In femoral condyle ulcers, it is further compressed using the ‘rolling-pin’ technique. No tissue glue is used, even in overhanging patellar facet ulcers. This is because Hyalofast is hydrophilic and marrow exudates act as a glue to gel the patch graft to the ulcer.
Post-surgery, the knee is kept locked in full extension. This prevents flexion and extension of the joint, which may dislodge the patch graft. Partial weight bearing with crutches is encouraged. After 2 weeks, the knee is allowed gradual flexion of 10° a day. Physiotherapy to regain range of movement and knee function will continue in earnest.
All patients were assessed with the knee injury and osteoarthritis outcome score (KOOS) 6–14 months after surgery. Patients who were agreeable were invited every year subsequently. The KOOS consists of five subscales: pain, other symptoms, function in daily living (ADL), function in sport and recreation (sport/rec) and knee-related quality of life (QOL). 17 Individual subscales of all patients KOOS scores were compared using paired t-test between year 1, year 2 and year 3 against year 0 (all patients group). Patients were further separated into two groups: all patients group and Hyalofast-only group. Patients who only had a concurrent lateral release with the Hyalofast procedure deemed to be the Hyalofast-only group. Individual subscales of patients from the Hyalofast-only group (with no meniscectomy/repair or ligament reconstruction, that is, with only microfracture and Hyalofast grafting) were also compared using paired t-test between year 1, year 2 and year 3 against year 0. All statistical analyses were done using Stata/IC 15.1.
Results
Of the 46 patients, there were 23 males and 23 females with an age range of 52.67 ± 8.06. Most (41) of the grade 4 chondral ulcers were from the medial tibiofemoral joint (Table 1). Two patients had associated ACL reconstruction, 36 patients had concurrent partial meniscectomy, 1 patient had a medial meniscus repair and removal of loose bodies and 45 patients had concurrent lateral retinaculum release. Twenty-six patients had multiple grade 4 chondral ulcers.
Grade 4 ulcers site and size.a

No.: number.
a± values are mean ± standard deviation.
Of the 46 patients, 10 patients had only a concurrent lateral release with the Hyalofast procedure and were deemed to be the Hyalofast-only group. Of these 10 patients, 5 had multiple lesions but none had no lesions without treatment.
There was a statistically significant improvement after surgery for all the subscales of the KOOS score (symptoms, pain, daily living, sports and QOL) between pre-surgery and years 1, 2 and 3 post-surgery for the all patients group (Table 2). KOOS scores for the Hyalofast-only group also had statistically significant improvement for the subscales of symptoms, pain and daily living between pre-surgery and years 1, 2 and 3 post-surgery. There was no statistically significant improvement for the subscales of sports and QOL for the Hyalofast-only group between pre-surgery and years 1, 2 and 3 post-surgery (Table 3).
KOOS results of all patients group (includes both patients with Hyalofast only and Hyalofast with other associated procedures).

KOOS: knee injury and osteoarthritis outcome score; pre: pre-surgery; SE: standard error; CI: confidence interval; p value: probability value; QOL: quality of living.
KOOS results of Hyalofast-only patient group.

KOOS: knee injury and osteoarthritis outcome score; pre: pre-surgery; SE: standard error; CI: confidence interval; p value: probability value; QOL: quality of living.
The extent of cartilage regeneration and the quality of regeneration of two patients (A and B) were also accessed with T2 mapping magnetic resonance imaging (MRI) assessment (Figures 1(a), (b), 2(a) and (b)). The MRI comparison between pre- and post-surgery showed filling of the defect with new cartilage-like tissues. T2 mapping of cartilage regeneration in the patient revealed signals similar but not exactly the same to neighbouring normal cartilage.

(a) MRI knee of patient A pre-microfracture and Hyalofast implantation (May 27, 2016). (b) MRI of patient A same knee 21 months after surgery (March 3, 2018). MRI: magnetic resonance imaging.

(a) MRI knee of patient B pre-microfracture and Hyalofast implantation (April 15, 2015). (b) MRI knee of patient B 36 months after surgery (March 26, 2018). MRI: magnetic resonance imaging.
Due to an unrelated meniscus tear, another patient (C) underwent a second arthroscopic surgery 18 months post-surgery. Arthroscopic finding during the second surgery revealed a complete filling of the lateral femoral condyle ulcer with cartilage (Figure 3(a) and (b)). Histological studies revealed the cartilage to be mainly fibrocartilage with islands of hyaline cartilage (Figure 3(c)).
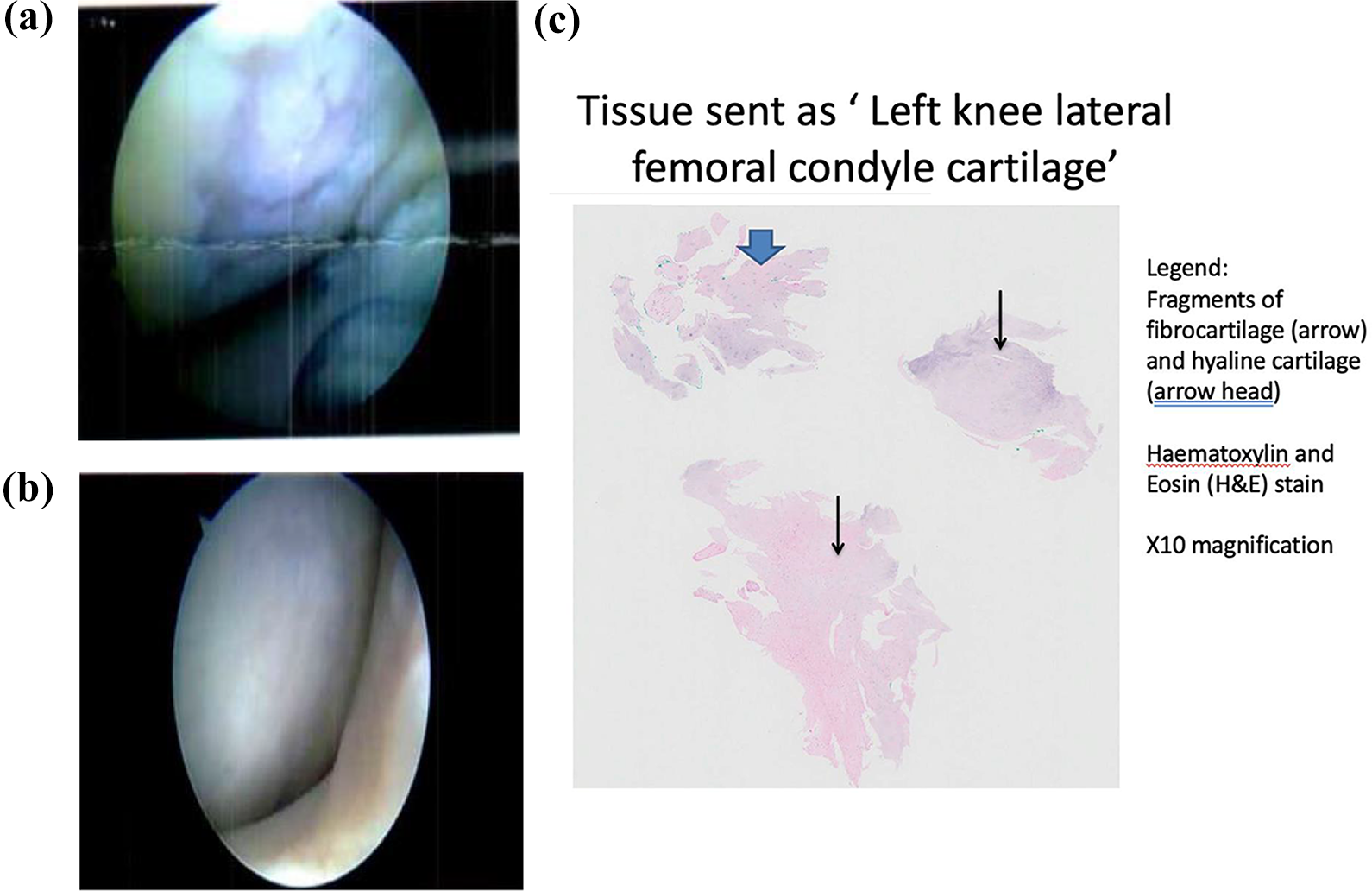
(a) Arthroscopic finding of left knee lateral femoral condyle showing cartilage ulcer pre- and post-microfracture. (b) Arthroscopic finding of left knee lateral femoral condyle showing Hyalofast graft applied and healed ulcer 18 months after microfracture and Hyalofast implantation. (c) Histological studies of left knee lateral femoral condyle 18 months after microfracture and Hyalofast implantation.
Discussion
Osteoarthritis is the result of degeneration, thinning and even denudation of cartilage, which leads to pain and limitation of function. 18 Currently, the only effective solution for osteoarthritis is joint replacement surgery. 19 However, it is an expensive and invasive procedure. The expected 15- and 20-year life span of the implant also limits the procedure to mainly patients older than 60 years of age.
Microfractures
Microfractures allow marrow stem cells to migrate to the surface and repopulate the cartilage ulcers with new cartilage. 20 The current literature shows that microfractures provide effective short-term functional improvement of knee function. 21 However, insufficient data are available on its long-term results. Some issues of the technique include limited hyaline repair tissue, variable repair cartilage volume and possible functional deterioration, 22 which requires further refinement. The regenerated cartilage over the microfractures was generally depressed with respect to surrounding cartilage. 23 However, our findings from the arthroscopy and MRI show that the synergistic effect of microfractures and Hyalofast can give a near restorative filling of the defect.
Autologous chondrocyte implantation
Autologous chondrocyte implantation reportedly regenerates cartilage better than microfractures. 24 Like Hyalofast, current autologous chondrocyte implantation techniques do employ bioscaffolding to augment cartilage repair. However, this method requires a two-stage procedure and is expensive. In our opinion, the Hyalofast graft is also more adaptable to lesions compared to the autologous chondrocyte implantation. Its soft and non-woven structure enables it to be cut and adaptively fitted into irregular lesions. This versatile nature of Hyalofast allows it to be implanted via a mini arthrotomy or arthroscopic surgery.
Hyalofast grafting with microfractures
Our case series suggest that cartilage regeneration in knee joint grade 4 cartilage ulcers with Hyalofast grafting and microfractures is a possible viable alternative for the treatment of osteoarthritis. Considering the simplicity and minimally invasive technique of Hyalofast grafting and microfracture, this will be a viable option for patients with significant cartilage deficiency who are either too young for joint replacement or who do not want an invasive procedure.
Compared to other gel-based cartilage regenerative solutions, Hyalofast can be used to resurface non-contained ulcers. Even with complete loss of the cartilage of the entire femoral or tibial condyle, Hyalofast can be used to resurface the entire joint compartment, quite similar to a unicondylar knee replacement, as seen in patients A and B in Figures 1 and 2 MRI scans.
Conclusion
Hyalofast grafting along with microfractures resulted in statistically significant improvement in symptoms, pain relief, improvement of activities of daily living, sports and QOL when all patients were included in the analysis. When analysing patients who only underwent Hyalofast grafting with microfractures, there was a statistically significant improvement in symptoms, pain relief and improvement of activities of daily living. The improvement is maintained up to 3 years post-surgery. Patients with painful knees due to cartilage defects can now have a less invasive, durable and effective option to treat their problems.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.