
Abstract
Objectives:
Acute kidney injury (AKI) is a rare but serious complication after hip fractures. The aim of this study was to evaluate the incidence and the risk factors of postoperative AKI after hip fractures.
Methods:
From January 2011 to December 2016, 550 patients who underwent surgery of hip fractures at our institution were retrospectively reviewed. AKI was defined and classified by AKI Network (AKIN) Classification/Staging System. The incidence, mortality, and risk factors of postoperative AKI were investigated. Receiver operating characteristic curve analysis was conducted to evaluate the ability of markers in predicting AKI.
Results:
The incidence of postoperative AKI was 4.4% (25 cases). The mean onset of postoperative AKI was 8.0 ± 5.3 days and recovered after 7.0 ± 4.2 days after the occurrence of AKI. Of 25 patients with AKI, 6 patients (24.0%) died within 1 year after surgery. The independent risk factors for postoperative AKI are the estimated blood loss (EBL) (odds ratio (OR) 1.64; 95% confidence interval (CI) 1.33–2.58; p < 0.01) and postoperative level of albumin (OR 1.77; 95% CI 1.52–2.74; p < 0.01). The cutoff value of the serum albumin was <2.8 g/dL with a sensitivity of 88.0% and a specificity of 77.1%. The cutoff value of EBL was <766.5 mL with a sensitivity of 84.0% and a specificity of 66.3%.
Conclusion:
Postoperative AKI after hip fractures had low incidences (4.4%) but high mortality (24.0%). The postoperative AKI was correlated with blood loss and low postoperative albumin levels.
Introduction
The worldwide population is steadily aging, thus causing an increase in the incidence of osteoporotic hip fractures. Although surgery for hip fractures has reports of a very low perioperative mortality rate and low medical complication rates, there will also be postoperative complications that lead to death after surgery. 1 –3 A previous report found that the main cause of death after hip fractures was cardiovascular-related. 4 According to Partridge et al., 5 acute kidney injury (AKI) after hip fractures had complications associated with mortality of the second most commonly.
Several studies have mentioned that dehydration or blood loss, nephrotoxic medication (nonsteroidal anti-inflammatory drugs (NSAIDs) and antibiotics), and patient comorbidities (such as hypertension, diabetes, and cerebrovascular disease) have all been reported as significant risk factors for postoperative AKI. 6,7 However, postoperative AKI is often unclear and multifactorial in etiology. The purpose of this study was to evaluate the incidence of AKI after hip fractures and the risk factors affecting postoperative rates of AKI after hip fractures.
Methods
This is a case–control study to evaluate factors that may cause postoperative AKI after hip fractures. This study had been approved by the Institutional Review Board. Informed consent was waived due to its retrospective nature.
Patient selection and demographics
From January 2011 to December 2016, 562 patients who underwent surgery of femoral neck, intertrochanteric hip, and subtrochanteric hip fractures at our institution were retrospectively reviewed. We then excluded 12 patients who had preexisting kidney dysfunction and had already treated with chronic dialysis therapy before hip fractures, leaving 550 patients to be enrolled in this study. Among these patients, 102 patients had undergone primary osteosynthesis and 448 patients had undergone hip arthroplasty by the present study’s senior authors. To identify risk factors that may have predisposition with patients to develop the postoperative AKI, we reviewed retrospectively all patients’ medical records enrolled in this study. Age, sex, weight, height, body mass index (BMI), smoking status, duration for hospitalization, dehydration, diabetes mellitus, shock, heart failure, nephrotoxic medication, and preexisting end-stage renal disease (ESRD) were recorded. The intraoperative changes in blood pressure, urine volume, and transfusion in anesthesia records were used to evaluate the intraoperative risk factors for AKI.
Defintion of AKI
AKI and AKI severity stage were defined by AKI Network (AKIN) Classification System, when the serum creatinine increased 1.5-fold over baseline or when the urine volume per hour was less than 0.5 mL/kg over 6 h (Table 1). 8,9 The level of serum creatinine and the volume of urine output were used to define AKI. Chronic kidney disease (CKD) was defined by Kidney Disease: Improving Global Outcomes guidelines based solely on estimated glomerular filtration rate (eGFR); eGFR < 60 mL/min/1.73 m 2 were regarded to have CKD. Also, when the patients had renal function below 15% and in need of hemodialysis, the patient was diagnosed with ESRD. 10 To evaluate the prognosis of postoperative AKI and CKD, dialysis morbidity and mortality within 1 year were also analyzed.
AKIN classification/staging system for AKI.

AKI: acute kidney injury.
Perioperative laboratory factors and hemodynamic factors
All patients received a laboratory tests including complete blood count, urine analysis, renal function tests, and electrolytes. The biochemical parameters such as albumin, blood urea nitrogen (BUN), and creatinine when admission were defined at baseline blood levels. To identify potential risk factors for AKI that may predispose patients to outcome after hip fracture surgery, the intraoperative parameters including blood pressure, urine volume, and transfusion were verified in anesthesia records. We also investigated whether these factors are significant for AKI. The intraoperative blood loss under anesthesia records cannot be accurately measured due to irrigation and loss of blood. Thus, we calculated the amount of blood loss 5 days after surgery by Mercuriali formula. 11,12 This formula required the blood volume of the patient calculated Nadler’s formula. Mercuriali’s and Nadler’s formula are as follows.



Statistical analysis
Between-group comparisons of variability were conducted utilizing the χ2 test and Fisher exact test, whereas between-groups comparison of continuous variability had been performed using Student’s t-test. Multivariate analysis was then conducted using all risk factors with a p value <0.10 in the univariate analysis. The risk factors for postoperative AKI at a p value of <0.05 had the inclusion of the multivariable logistic regression analysis. The cutoff value of risk factors for patients with AKI was defined using a receiver operating characteristic (ROC) curve. The sensitivity, specificity, accuracy, and Youden’s index were calculated with respect to AKI. Statistical significance had a definition as a p < 0.05. Statistical analysis was pulled off utilizing SPSS software (version 18.0; SPSS, Chicago, Illinois, USA) with a confidence interval (CI) of 95%.
Results
Patient characteristics
Demographic characteristics are compared between AKI and non-AKI groups in Table 2. There were 159 men (28.9%) and 391 women (71.1%) with a mean age of 70.1 ± 8.6 years. Other demographic factors of age, gender, height, weight, BMI, smoking, diabetes, hypertension, and cerebrovascular disease showed no statistical difference (p > 0.05). The mean duration of hospital stay for those who developed postoperative AKI increased compared to patients in non-AKI group (26.0 ± 7.9 days vs. 14.5 ± 1.4 days, p < 0.05). There were no differences in the incidence of AKI according to the surgical method between primary osteosynthesis and hip arthroplasty (p > 0.05).
Demographics of patients.a

AKI: acute kidney injury; SD: standard deviation; CVA: cerebrovascular accident; BMI: body mass index; DM: diabetes mellitus; HTN: hypertension; NSAIDs: nonsteroidal anti-inflammatory drugs; AKIN: AKI Network.
a All other comparisons of categorical variables performed using the χ 2 analysis or Fisher exact test.
b Statistical comparison performed using the independent samples t-test.
c Data presented as mean ± SD.
Incidence and prognosis of postoperative AKI
The overall incidence of postoperative AKI was 4.4% (25 cases). They were classified by AKIN Staging System; 8,9 19 cases (76.0%) at stage 1, 1 case at stage 2 (4.0%), and 5 cases (20.0%) at stage 3. The mean onset of postoperative AKI was 8.0 ± 13.3 days and recovered after 7.0 ± 8.0 days after the occurrence of AKI. Of 25 patients with AKI, 6 patients (24.0%) died of CKD (3 patients), pneumonia (2 patients), and multiple organ failure (1 patient) within 1 year after surgery. In contrast, of 525 patients without AKI, 10 patients (1.9%) died of ischemic heart disease (1 patient), pneumonia (2 patients), cancer (2 patients), septic shock (2 patients), and multiple organ failure (3 patient) within 1 year after surgery. There was a statistically significant difference in the 1-year mortality rate between the two groups (p < 0.01).
Laboratory and hemodynamic finding
The laboratory and hemodynamic data of patients are presented in Table 3. The serum BUN, hemoglobin, and creatinine were not significant factors in both AKI and non-AKI groups. The postoperative level of serum albumin was identified as the significant risk factor (p < 0.01). There were no significantly statistic differences in the intraoperative records of blood pressure, operation time, and amount of transfusion (p > 0.05). The estimated blood loss (EBL) was 860.0 ± 125.7 mL for the AKI group and 709.0 ± 133.6 mL for the non-AKI group showing significant differences in Table 3 (p < 0.01).
Laboratory and hemodynamic data of patients with hip fractures.a
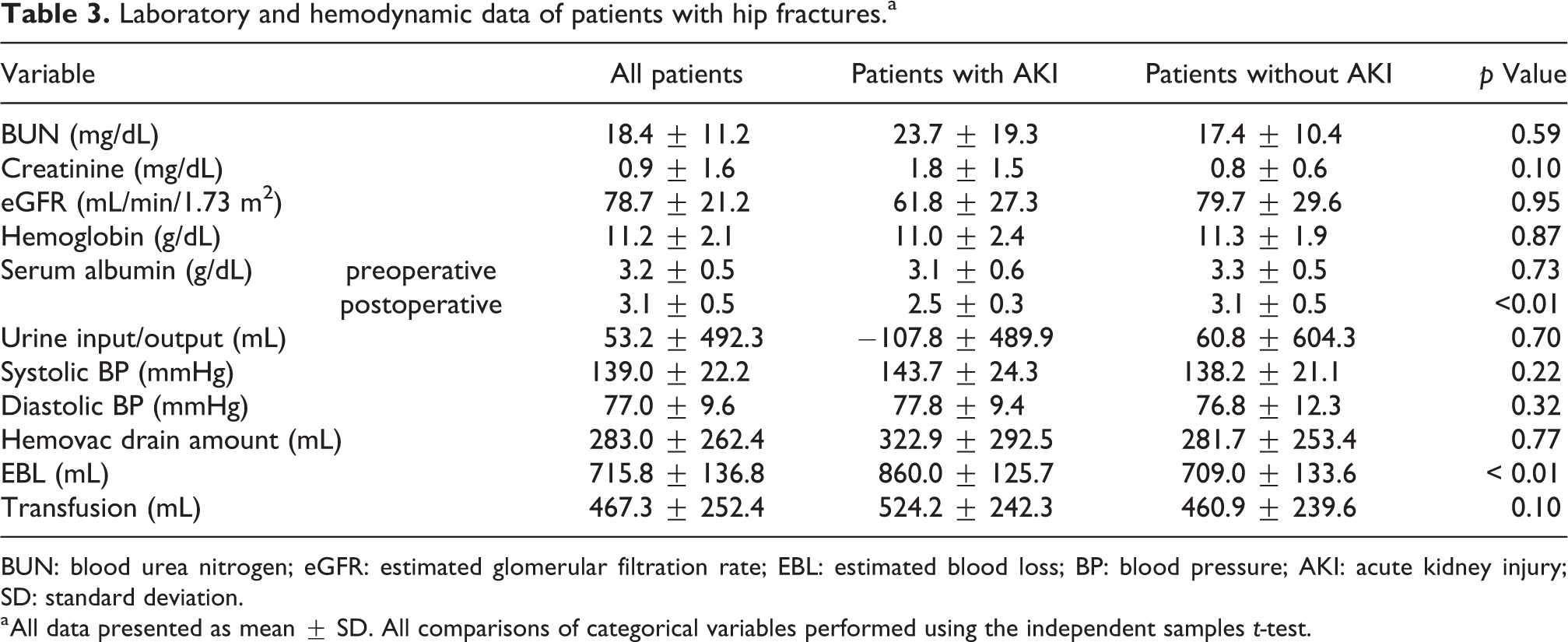
BUN: blood urea nitrogen; eGFR: estimated glomerular filtration rate; EBL: estimated blood loss; BP: blood pressure; AKI: acute kidney injury; SD: standard deviation.
a All data presented as mean ± SD. All comparisons of categorical variables performed using the independent samples t-test.
The significant risk factors of postoperative AKI in multivariate analysis
In univariate analysis, the duration for hospitalization (p = 0.04), EBL (p < 0.01), and postoperative albumin (p < 0.01) were significantly associated with AKI. However, multivariate logistic regression modeling evaluated two significant independent predictors of postoperative AKI. Only EBL (odds ratio (OR) 1.64; 95% CI 1.33–2.58; p < 0.01) and postoperative level of albumin (OR 1.77; 95% CI 1.52–2.74; p < 0.01) evaluated the independent predictors of postoperative AKI (Table 4). Figure 1 shows the ROC curves of postoperative serum albumin levels predicting AKI. The areas under curve (AUC) were 0.86. The cutoff value of the serum albumin was <2.8 g/dL with a sensitivity of 88.0% and a specificity of 77.1%. Figure 2 shows the ROC curves of EBL predicting AKI. The AUC were 0.80. The cutoff value of EBL was 766.5 mL with a sensitivity of 84.0% and a specificity of 66.3%.
Risk factors of AKI as determined by univariate and multivariate analyses.a

AKI: acute kidney injury; OR: odds ratio; CI: confidence interval; EBL: estimated blood loss.
a Multivariate analysis was then created using all risk factors with a p value <0.05 in the univariate analysis. Each additional variable was then sequentially added to the model and removed to ensure that none were significant risk factors (p < 0.05) of postoperative AKI or confounders or effect modifiers.
b The values are given as the OR with the 95% CI in parentheses.

ROC curves for serum albumin level to evaluate the ability of markers in predicting AKI; AUC: 0.86, the cutoff value of the serum albumin: <2.8 g/dL with sensitivity: 88.0% and specificity: 77.1%. ROC: receiver operating characteristic; AKI: acute kidney injury; AUC: areas under curve.

ROC curves for EBL to evaluate the ability of markers in predicting AKI; AUC: 0.80, the cutoff value of EBL: 766.5 mL with sensitivity: 84.0% and specificity: 66.3%. ROC: receiver operating characteristic; EBL: estimated blood loss; AKI: acute kidney injury; AUC: areas under curve.
Discussion
The present study evaluated the incidence of AKI among patients with hip fracture surgery was 4.4% and CKD requiring hemodialysis was 0.8%. The previous studies reported incidences of AKI related with hip fractures widely extended within 8–24%. 4,8 –10 The reports in other studies are attributable to the use of variable definitions of AKI, variety in the monitoring periods, and heterogeneity of the selected patients. Because we diagnosed AKI based on both urine output and serum creatinine, the incidence of AKI in our study is considered to be lower than in other studies.
Ulucay et al. 13 reported that the amount of intraoperative bleeding has influence on AKI and that bleeding amount should be considered as the high-risk factor. In the present study, the amount of intraoperative bleeding recorded in the anesthesia record had no statistical difference. The amount of perioperative bleeding could not be measured precisely due to saline irrigation and loss of blood. Thus, this study used the Mercurier’s formula 11 on the assumption that the actual bleeding amount would be different due to hidden blood loss. In our study, EBL was statistically significant differences between AKI and non-AKI groups and the amount of EBL could be used as the marker in predicting AKI through ROC curve analysis (AUC: 0.80). However, two groups in this study showed similarity in the amount of perioperative transfusion. Thus, it can be inferred that postoperative AKI may occur when appropriate blood transfusion is not performed on patients with massive bleeding.
Shin and Han 14 reported that early postoperative hypoalbuminemia has an independent risk factor for AKI. In our study, the level of postoperative albumin in postoperative AKI group was significantly lower than in the non-AKI group and postoperative albumin level could be used as the marker in predicting AKI through ROC curve analysis (AUC: 0.86). Moreover, the patients who underwent CKD with hemodialysis were significantly lower albumin levels (2.3 ± 0.4 g/dL). Although the mechanism of albumin is uncertain, albumin maintains the colloid osmotic pressure, increases the renal blood flow, and protects renal function. On the subject of renal perfusion, albumin functions with nitrogen oxides to form S-nitroso-albumin, and renal vasodilation via albumin connecting with platelet-activating factor results in improved renal perfusion. 15 Moreover, albumin protects the glycocalyx of endothelial cells and maintains the endothelial barrier, but albumin with damage of endothelial glycocalyx layers may be the cause of postoperative AKI along with early postoperative hypoalbuminemia. 14,15 Therefore, intensive care should be taken as to the possibility of AKI when albumin levels are less than 2.8 g/dL and albumin supplementation is required.
AKI secondary to nephrotoxic medication (antibiotics, NSAIDs, etc.) has been reported as a significant risk factor in other studies. 2 Nephrotoxic medication (3.0%) is reported as the risk factor for AKI after major surgery including invasive surgery. 16 However, the use of NSAIDs had no independent association with postoperative AKI in the present study (p = 0.14). Patients in our study were closely monitored for urine output and level of creatinine, thus immediately stopped using NSAIDs when kidney function decreased.
Most studies have investigated the prognosis of AKI after hip fractures but it is short-term mortality within 90 days. 17 –20 According to Pedersen et al., 19 1717 (12.7%) of 13,529 elderly patients with hip fractures developed AKI within 5 days of surgery. Those with AKI had a 2.8-fold higher risk of short-term mortality within 3 months and a 1.3-fold higher risk of long-term mortality over 3 months had those without AKI. In the present study, perioperative mortality rates are 24.0% (six cases). There were no cases of short-term mortality rates of less than 3 months, but most of them died within 1 year after surgery. Our study found that only three of them died from postoperative AKI and long-term mortality was 50.0%.
The limitations of this study are as follows. First, this study is retrospective. Thus, it would be necessary to conduct a large-scale prospective study and consider about all those differences. Second, this study could not identify the cause of AKI by dividing into three categories; prerenal, renal, and postrenal AKI. Patients with AKI could not be classified because they did not have sufficient urine tests. Third, our results also demonstrated that the incidence of postoperative AKI is relatively low. Because the incidences of AKI vary based on various definitions, the study of review is necessary for several criteria of AKI.
Conclusion
Postoperative AKI after hip fractures had a low incidence (4.4%) but high mortality (24.0%). The important risk factors for postoperative AKI are blood loss and postoperative serum albumin levels. Therefore, surgeons should attempt to adequate transfusion and albumin management strategies especially in the patient with increased expected blood loss.
Footnotes
Acknowledgements
This study was supported by Inha University research grant.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.