
Abstract
Purpose:
Modular fluted tapered stems are one of the most commonly used implants in femoral revision surgery. Due to the relative lack of studies on the Restoration modular fluted tapered stem, we conducted a study to evaluate its short- to mid-term clinical, radiographic, and survival outcomes.
Methods:
We identified all 45 patients treated with this revision stem at our institution. Five patients did not complete the minimum 2-year follow-up, leaving 40 patients (41 hips) for assessment. Mean follow-up was 5.1 years (range 2–11 years). Clinical outcomes were assessed using the Harris hip score (HHS). Radiographs were evaluated for subsidence and loosening. Kaplan–Meier survival analysis was performed using revision of the stem for any reason as end point.
Results:
The mean HHS improved from 44.6 points preoperatively to 78.4 points at the most recent follow-up (p < 0.0001). Nonprogressive subsidence occurred in 83% of the hips (mean 2.8 mm; range 1–7 mm). One stem (2.4%) showed progressive subsidence (20 mm) and was considered loose. The most common cause for reoperation was dislocation (three hips, 7.3%). The 10-year survivorship with revision of the stem for any reason as the end point was 93.5% (95% CI, 84.9–100%).
Conclusion:
There was a significant improvement in the HHS and a low likelihood of revision at short- to mid-term follow-up, adding to the current evidence base for use of this implant in revision surgery. A longer follow-up and a larger number of cases are necessary to fully evaluate its role and performance.
Introduction
A steady increase in the number of revision surgeries after total hip arthroplasty (THA) has been reported in the literature in the last two decades 1,2 and this trend is expected to continue in the next years. 3,4 In the United States, the revision burden for THA has been reported to range between 14.6% and 17% over the last decade 5,6 and is projected to double by 2026. 7 This occurrence has been attributed to the increasing absolute number of primary THA performed, expansion of the indications of THA to include younger patients, and increasing life expectancy, among other factors. 4,6,8,9
A number of different femoral stem designs and reconstructive techniques have been proposed to manage cases of revision THA, including cemented stems with 10,11 or without 12 impaction bone grafting, allograft-prosthetic composites, 13 extensively porous-coated cylindrical stems, 14,15 and modular fluted tapered stems. 16,17 In this challenging scenario, modular stems are a popular and attractive choice since implant version, offset, and leg length can be handled independently of each other, thus having the potential to better restore hip biomechanics and make the surgical procedure easier. 18,19
The aims of this study were to determine the short- to mid-term clinical and radiographic outcomes and the survivorship of a modular fluted tapered stem in revision THA.
Materials and methods
We identified all 45 patients treated with a modular fluted tapered stem (Restoration modular stem, Stryker Orthopedics, Mahwah, New Jersey, USA) during revision THA at a single university hospital between June 2007 and May 2016. The patients were identified through a prospectively collected institutional database used to follow all patients who have undergone a primary or revision THA at our institution. Of the 45 patients, five did not complete the minimum 2-year follow-up: three died from causes unrelated to the revision THA and two were lost to follow-up; none of these five patients were known to have undergone any additional surgery as of our last evaluation. Thus, 40 patients (41 hips) were available for review. Our Institutional Review Board (IRB) approved the study (IRB file number 2.579.381) and all patients provided written informed consent.
There were 24 men (25 hips) and 16 women (16 hips), with a mean age of 63.8 years at the time of the revision THA (range 33–89 years). The most common indication for surgery was aseptic loosening (29 hips, 70.8%), followed by periprosthetic fracture (eight hips, 19.5%), periprosthetic joint infection requiring two-stage revision (three hips, 7.3%), and stem fracture (one hip, 2.4%). Minimum follow-up period was 2 years and the mean follow-up period was 5.1 years (range 2–11 years).
The Restoration modular stem used in this study consists of a distal fluted tapered stem with a grit-blasted surface and a proximal cone body with a hydroxyapatite plasma-sprayed surface; both parts are made of titanium alloy. The stems are available in three lengths (155, 195, and 235 mm) and each is available in 15 diameters in 1-mm increment (14–28 mm). The cone bodies are available in four lengths (70, 80, 90, and 100 mm) and each is available in seven diameters in 2-mm increments (19–31 mm); they have a 132° neck angle and accept cobalt–chromium heads with diameters of 22, 26, 28, 32, and 36 mm or alumina ceramic heads with diameters of 28, 32, and 36 mm.
All revision THA were performed by two surgeons through a direct lateral approach. 20 An extended trochanteric osteotomy (ETO) 21 was performed in 17 hips (41.5%) to allow component or cement removal. For each of the ETO cases, the osteotomy was then reduced and held in place with two or three cerclage cables; a prophylactic cerclage wire was placed approximately 1 cm distal to the osteotomy to decrease the risk of fracture during stem insertion and cortical strut allografting was not used in any patient. Twenty-nine hips (70.8%) underwent a combined acetabular and femoral revision, six hips (14.6%) underwent an isolated acetabular liner exchange with the femoral revision, and six hips (14.6%) had the femoral revision performed alone. The femoral revision was performed according to the operative technique recommended by the designers of the implant. After removal of the failed stem, the femoral canal was debrided and sequentially reamed guided by preoperative templating until a firm resistance in supportive bone was achieved. A distal stem of adequate length and the same diameter as that of the final reamer was inserted so that the stem was anchored in cortical bone for at least 5 cm or two canal diameters below the tip of the existing implant or femoral defect. The proximal femur was prepared with reamers to receive the trial cone body and determine the best offset, anteversion, and length. After trialing, the definitive proximal cone body was inserted and locked to the distal stem. Wound lavage and closure were done in a standard manner. Suction drains were used in all cases and removed after 24 h. The median stem length and diameter were 195 mm (range 155–35 mm) and 18 mm (range 14–24 mm), respectively. The median cone body length and diameter were 80 mm (range 70–100 mm) and 23 mm (range 19–27 mm), respectively. Cobalt–chromium heads were used in all cases and the median diameter was 28 mm (range 22–36 mm).
Patients received standard postoperative care with analgesics and physical therapy. Thromboprophylaxis was performed using graduated compression stockings and unfractioned heparin for 4 weeks. Antibiotic prophylaxis with a first-generation cephalosporin was used in all patients other than the three cases of two-stage revision (periprosthetic joint infection); in such cases, antibiotic treatment was set up on individual basis according to the results of antimicrobial susceptibility testing and under the supervision of the infectious disease specialist. The standard postoperative rehabilitation program included early mobilization, toe-touch weight-bearing with a walker during the first 6 weeks, followed by partial progressive weight-bearing during the next 6 weeks and total weight-bearing thereafter.
Clinical outcomes were assessed using the Harris hip score (HHS) 22 preoperatively and at the most recent follow-up. Anteroposterior (AP) digital radiographs of the pelvis and AP and lateral digital radiographs of the femur were obtained preoperatively, immediately after surgery, and then at each of the follow-up intervals (6 weeks, 3 months, 6 months, 1 year, and annually thereafter). Using a computer-based picture archiving and communication system, all radiographs were evaluated by consensus of two experienced arthroplasty surgeons who were not involved in the patients’ care and were blinded to the clinical outcomes. The preoperative femoral bone defects were categorized according to the Paprosky classification 5 ; the most common bone defect was Paprosky type IIIB (14 hips, 34.2%), followed by type II (11 hips, 26.8%), type IIIA (10 hips, 24.4%), and type IV (6 hips, 14.6%). All periprosthetic fractures were type B3, according to the Vancouver classification. 23 The postoperative radiographs were analyzed to assess stem subsidence, stem loosening, fracture healing (in cases of periprosthetic fracture), and osteotomy site healing (in cases that required an ETO). The initial postoperative radiographs served as the baseline with which the subsequent radiographs were then compared. Stem subsidence was defined as any amount of distal migration of the stem and was measured from the shoulder of the stem to the most medial point of the lesser trochanter, as described by Malchau et al., 24 but when the lesser trochanter was not visible on the radiographs, the measurement was performed using other fixed landmark on the femur such as the most proximal point of the greater trochanter or a cerclage cable 25 ; in all cases, the measured values were corrected for magnification using the known prosthetic head diameter as a reference. Stem loosening was diagnosed if there was progressive subsidence or if there were progressive circumferential radiolucent lines of >1 mm around the fluted tapered portion of the implant. 25,26 Radiological fracture union or osteotomy site union was defined as the presence of bridging bone across the main fracture site or osteotomy site in two orthogonal planes. 27 All intraoperative or postoperative complications were also recorded, including fractures, dislocations, nerve palsies, infection, or need for subsequent surgeries.
Kaplan–Meier survival analysis was performed using revision of the stem for any reason, revision of the stem for aseptic loosening, and any reoperation as end points. Revision of the stem was defined as any operation for removal or replacement of this component. For each end point, the survival probability with 95% confidence interval (95% CI) was calculated using the R software (R Development Core Team, Vienna, Austria). Student’s t-test for paired samples was used to compare the mean values of preoperative and postoperative HHS. The SAS 9.4 software (SAS Institute Inc., Cary, North Carolina, USA) was used in this analysis and significance was set at p <0.05.
Results
All patients had an improvement in the HHS. The mean HHS improved from 44.6 points (range 19–63 points) preoperatively to 78.4 points (range 56–98 points; p < 0.0001) at the most recent follow-up (Figure 1).

Box plot of the HHS values preoperatively (pre-OP) and at the latest follow-up (post-OP). HHS: Harris hip score, OP: operative.
Six stems (14.6%) had no subsidence, 34 stems (83%) had nonprogressive subsidence (mean 2.8 mm; range 1–7 mm) detected within the first 6 months after surgery, and one stem (2.4%) that used to treat a Paprosky type IV femoral defect had a progressive subsidence of 20 mm (Figures 2 and 3). No cases of progressive circumferential radiolucent lines around the fluted tapered portion of the implant were detected. Thus, only one stem was considered loose. All periprosthetic fractures and ETOs showed radiological union, which occurred typically between the third and sixth months after surgery.

Distribution of the degree of stem subsidence in the series. Subsidence of up to 5 mm was noted in the majority of cases.
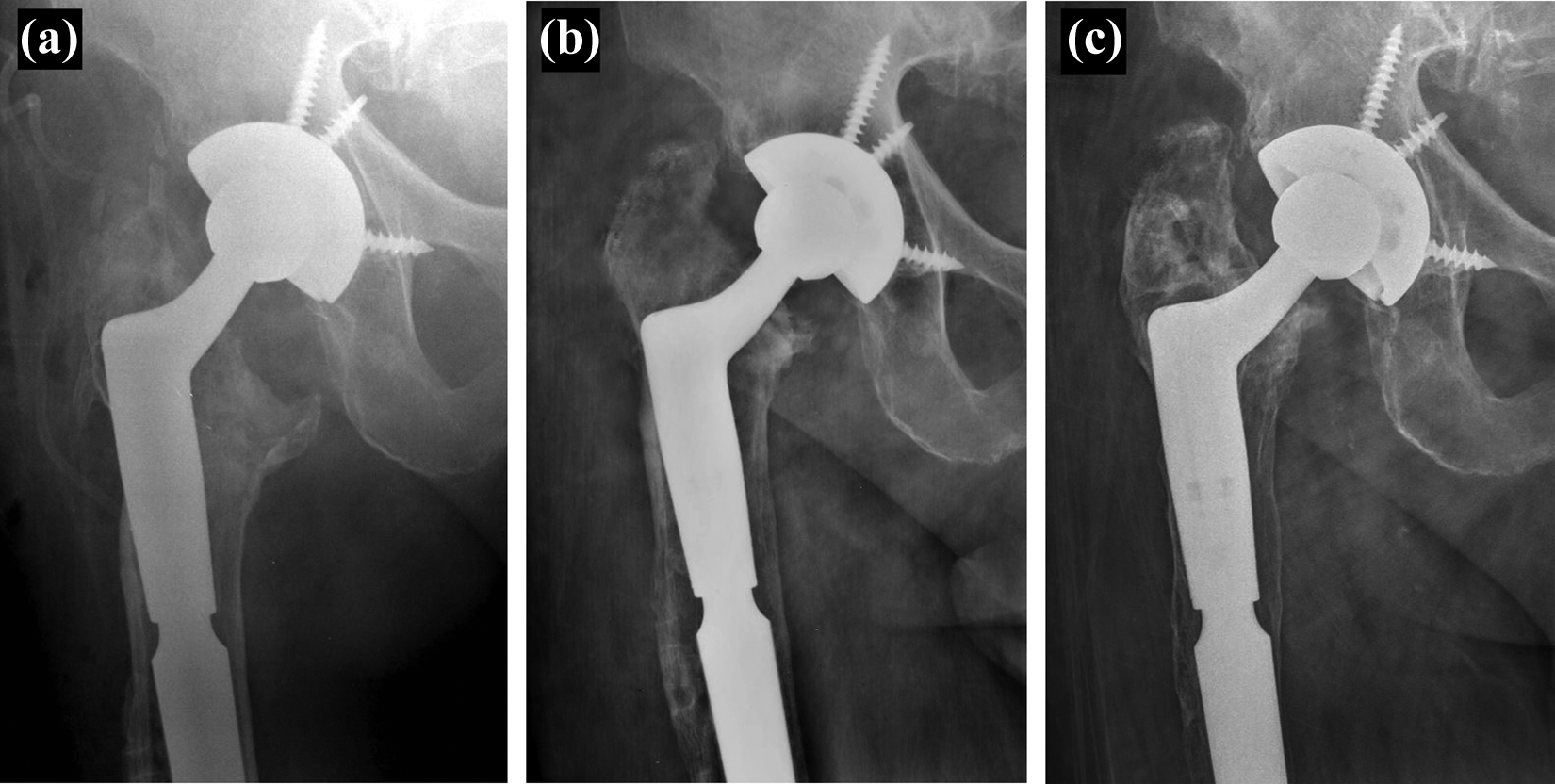
Radiographs illustrating progressive subsidence of the stem. (a) Immediate postoperative control, (b) 3 months after surgery, and (c) 1 year after surgery.
There were three intraoperative fractures (7.3%). One was a small, incomplete fracture of the anterior femoral cortex at the level of the distal tip of the stem that occurred during its insertion and required no additional treatment other than delayed weight-bearing. The other two fractures involved the greater trochanter during proximal reaming and were treated with tension band wiring. No postoperative periprosthetic fractures were observed.
Seven hips (17%) required some sort of reoperation. Wound hematoma occurred in one hip (2.4%) and was treated with surgical drainage. Dislocation occurred in three hips (7.3%) and all were treated successfully with closed reduction and temporary bracing without recurrence. Periprosthetic joint infection occurred in two hips (4.9%); in one hip, early surgical debridement with modular head and liner exchange and prosthesis retention was successful, but the other hip required a resection arthroplasty due to persistent infection. Aseptic loosening occurred in one hip (2.4%); this patient presented with progressive subsidence (20 mm) of the stem, as already mentioned in this section, and was also treated with resection arthroplasty due to multiple medical comorbidities and extensive femoral bone loss (Paprosky type IV). Thus, two stems (4.9%) had been removed in the series.
Lastly, one patient developed sciatic nerve palsy and showed only partial recovery during follow-up. There were no other complications related to the revision THA.
Kaplan–Meier survival rates at 10 years were as follows: 93.5% (95% CI, 84.9–100%; Figure 4) with revision of the stem for any reason as the end point, 97.6% (95% CI, 93–100%; Figure 5) with revision of the stem for aseptic loosening as the end point, and 78.4% (95% CI, 64.4–95.5%; Figure 6) with any reoperation as the end point.
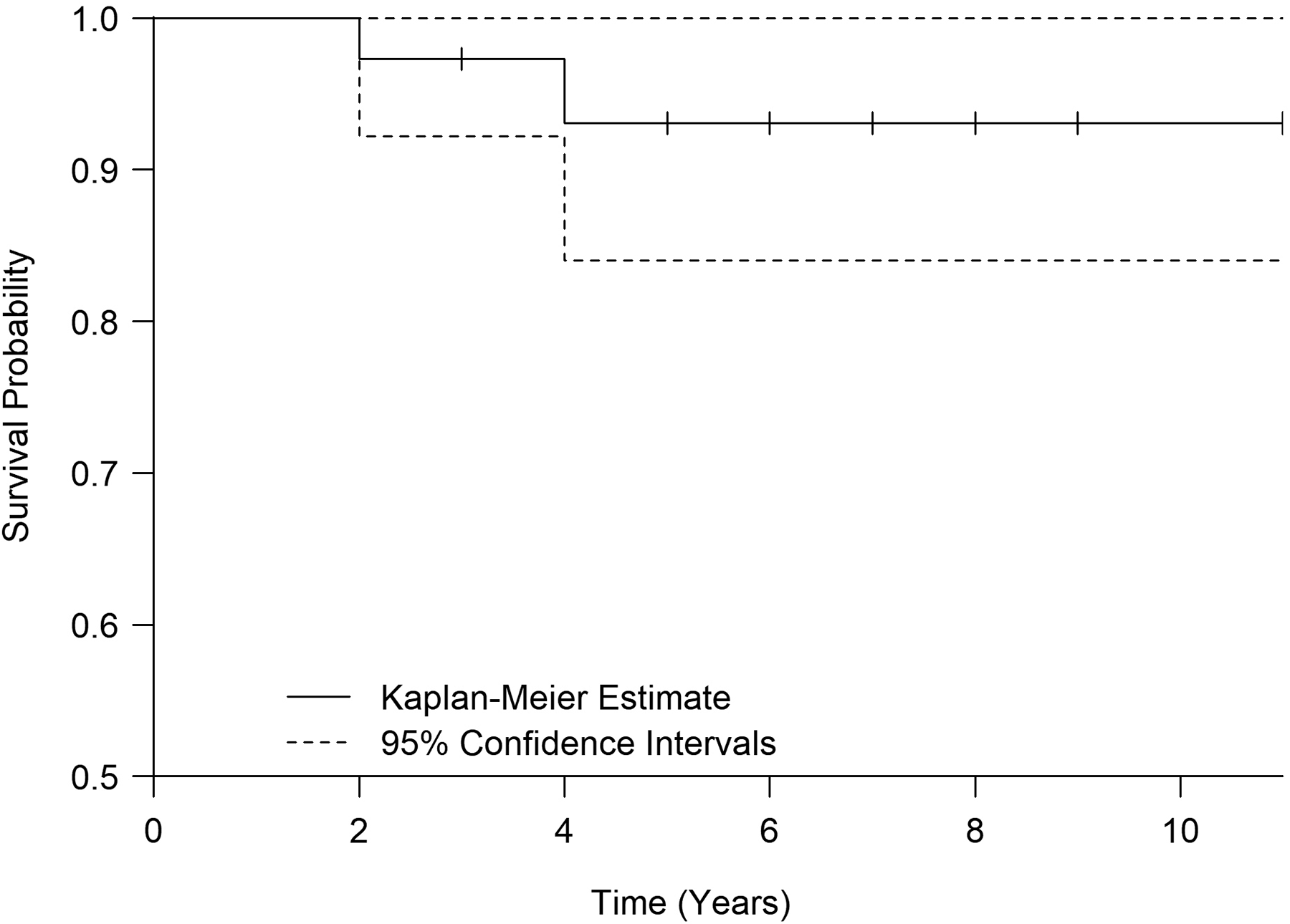
Kaplan–Meier survival analysis with revision of the stem for any reason as the end point.

Kaplan–Meier survival analysis with revision of the stem for aseptic loosening as the end point.

Kaplan–Meier survival analysis with any reoperation as the end point.
Discussion
Modular fluted tapered stems are one of the most commonly used implants for femoral revision arthroplasty in North America. 16 This implant design allows surgeons to bypass the proximal femoral bone deficiency and achieve secure stem fixation distally, as well as addressing offset, joint stability, and leg length discrepancy independently of each other with the proximal body. 18,28,29 Other potential advantages of this implant design are immediate axial and rotational stability, reduced stress shielding, and lower rates of thigh pain and intraoperative fractures compared with extensively porous-coated monoblock stems. 16,25
There is a relative lack of studies on the Restoration modular fluted tapered stem. Compared to the previous studies on this implant, 18,27 –32 the current investigation has one of the longest mean follow-up times (5.1 years). The previous studies (Table 1) have shown positive functional outcomes across Paprosky classifications I–IV, with low rates of aseptic loosening. We found a mean increase of 33.8 points in the HHS, in line with these previous studies, which reported a mean increase in the HHS ranging from 15 18 to 34.3 28 points. The aseptic loosening rate in our investigation was 2.4%, which was also comparable to the rates reported previously for this stem (Table 1).
Comparison of data from current and previous studies.
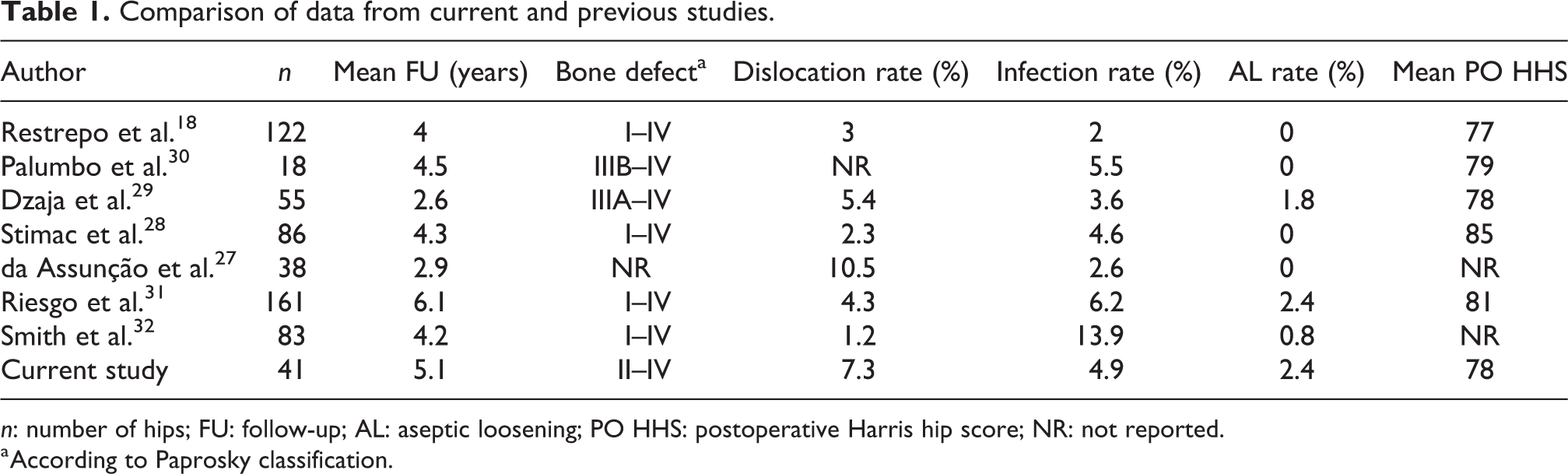
n: number of hips; FU: follow-up; AL: aseptic loosening; PO HHS: postoperative Harris hip score; NR: not reported.
a According to Paprosky classification.
Overall, 17% of the hips required reoperation for any reason in our study, a higher rate than previously reported for the same stem, which ranged from 8% 18 to 15.7%. 27 According to Brown et al., 33 a relatively high reoperation rate is somewhat anticipated given the complexity of the reconstructions and the poor medical condition of many of the revision patients. The most common reason for reoperation in our study was instability, which was seen in 7.3% of the hips, a rate comparable to the previous reports (Table 1). Given the high risk of dislocation in revision hip arthroplasty, we now favor the use of large-diameter femoral heads routinely. 33,34
Stem subsidence is a concern in femoral revision arthroplasty 30,31 and uncontrolled subsidence has been regarded as a major cause for failure of uncemented revision stems. 35,36 Stem subsidence has been reported with a variety of implant designs, such as monoblock fluted tapered stems, 37,38 extensively porous-coated cylindrical stems, 39,40 and modular fluted tapered stems. 16,41,42 Subsidence of the Restoration modular fluted tapered stem has been reported to occur in 3.6–100% of the cases 29,30 ; such heterogeneity in subsidence rates may be related to the variability of the severity of preoperative bone defects and criteria used to define subsidence. In fact, while some authors, 28,30 like ourselves, consider subsidence as any amount of distal migration of the stem, others define it as a distal migration that exceeds 5 mm 42,43 ; using this last threshold, the subsidence rate in our series would be 12.2% instead of 85.4%. The mean subsidence of the stem in our series was 2.8 mm, in accordance with previous studies on the same implant, which have reported mean subsidence ranging from 0.6 mm 31 to 3.5 mm. 30 In line with the findings of Park et al., 44 all cases of nonprogressive subsidence in our investigation were detected within 6 months after surgery.
The intraoperative fracture rate of 7.3% noted in this study was higher than reported by previous studies on the same implant, which ranged from 0% 18 to 5%. 32 Most of our intraoperative fractures involved the greater trochanter during proximal reaming; to prevent such fractures, we recommend that proximal reaming always be initiated with the smallest diameter reamer, that is, the 19-mm proximal reamer and progressively larger diameter reamers be used with great care until adequate contact with the metaphyseal bone is achieved.
Using revision for any reason as the end point, the stem survival rate in this study was 93.5% at 10 years. Using this same end point, three previous studies have also reported survival rates for the Restoration modular fluted tapered stem: Palumbo et al. 30 found a rate of 94% at 4.5 years, while Riesgo et al. 31 reported 85.1% at 6.1 years, and Smith et al. 32 reported 82% at 6.1 years. Thus, even at a later follow-up time point, our stem survival rate was similar or better than the rates reported previously; the lower infection rate in our series, compared with that of these other authors (Table 1), may have contributed to this finding.
Although rare, one possible complication of modular fluted tapered stems is the stem fracture. Risk factors for this complication include high body mass index, high level of activity, small medullary canal diameter, and severe bone loss with the lack of proximal medial support. 45 It occurs usually at the modular junction of the stem and has been reported with stems from a variety of manufacturers. 16,46 –50 We have not observed any stem fracture in our series, but Rueckl et al., 51 in 2017, reported the first two cases of fracture of a Restoration modular fluted tapered stem; interestingly, both fractures occurred at the mid-portion of the distal stem and not at the modular junction. Another potential complication of modular fluted tapered stems is the generation of wear debris and release of metal ions from the modular junction. 52 However, to the best of our knowledge, there have not been any reported data on adverse local tissue reactions (ALTR) associated with this stem design in revision THA. One possible reason for the supposed absence of ALTR with these stems until now is the fact that they are made of titanium alloy, which shows less fretting and crevice corrosion than cobalt–chromium–molybdenum implants. 53
Several other modular fluted tapered stems have also demonstrated favorable outcomes in revision arthroplasty at short- to mid-term follow-up, 41,54 –58 indicating that this stem design is useful clinically. It must be emphasized, however, that is not possible to claim that modular fluted tapered stems perform better than other implants in femoral revision arthroplasty. The diversity of stem designs and reconstructive techniques that have been described for this purpose indicates that controversy still exists about the best choice of treatment. 59,60
Some limitations of this study must be addressed. Our data, although collected prospectively, were reviewed retrospectively and thus subject to the limitations of this study design. Next, the study was noncomparative, and therefore, it is uncertain if different reconstructive techniques or stem designs would have led to analogous results; large prospective controlled trials are needed on this topic. Furthermore, subsidence was measured using anatomical radiographic landmarks, which are not as accurate as radiostereometric analysis. Finally, we had only short- to mid-term follow-up; a longer follow-up is required to confirm the effectiveness of this implant regarding its long-term survivorship and evaluate possible failures and adverse issues related to its modularity.
Conclusion
In conclusion, our investigation demonstrated a significant improvement in a functional hip scoring system (HHS) and a low likelihood of revision at short- to mid-term follow-up with the Restoration modular fluted tapered stem, adding to the current evidence base for use of this implant in revision surgery. However, a longer follow-up and a larger number of cases are necessary to fully evaluate the role and performance of this implant.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.