
Abstract
Purpose:
To evaluate intraoperatively the effects of femoral offset and head size on stability of the hip joints in total hip arthroplasty (THA) via posterior approach.
Methods:
Thirty cementless THAs were included in this study. After acetabular shell and femoral broach fixation, trial reduction was repeated using a femoral neck (5- to 8-mm higher or standard offset) and a head (26 mm or 32 mm). To evaluate joint stability, range of internal rotation (IR) in hip flexion prior to posterior subluxation and range of external rotation (ER) in hip extension were measured.
Results:
The high-offset neck provided significantly (approximately 10°) greater range of IR to subluxation than the standard-offset neck. No hips ended in anterior subluxation by ER. The head size did not have significant effects on the stability.
Conclusion:
Results suggest that the 5- to 8-mm greater femoral offset might be effective in preventing instability in primary THA.
Keywords
Introduction
Postoperative dislocation is one of the most frequent and distressing early complications after total hip arthroplasty (THA). In order to prevent dislocation, it is important to avoid prosthetic impingement and osseous impingement. One of implant-related factors affecting the impingement is the ratio of head diameter to neck diameter. 1,2 A smaller femoral head has a smaller prosthetic range of motion of the total hip components (oscillation angle) and would be a risk factor of dislocation. 2 The oscillation angle can be easily increased using a larger head, which has become widespread due to the advent of highly cross-linked polyethylene. 3,4 A previous review of primary hip arthroplasties showed that a larger femoral head diameter was associated with a lower long-term cumulative risk of dislocation, 5 although other clinical studies failed to demonstrate a significant effect of the head size on the rate of dislocation after primary THA. 6,7
Another factor affecting postoperative instability is muscular imbalance, which is influenced by total component offset. This is a perpendicular distance between the head center and the long axis of the femoral stem. Both the neck-shaft angle and the neck length affect the femoral component offset, and thus affect muscular imbalance following THA. 8 Therefore, femoral component offset could be one of the implant-related factors affecting postoperative instability, although a review of 560 primary and revision hip arthroplasties detected no significant difference of the mean offset between the cases with and without postoperative dislocation. 9 The purpose of this study was to evaluate the effects of both the femoral component offset and head size on joint stability after THA.
Materials and methods
Data were obtained from 30 patients (30 hips) undergoing primary cementless THA. Average patient age was 63.0 years (44–80), and 66% of the patients were female. Preoperative diagnosis was osteoarthritis secondary to hip dysplasia (Crowe’s classification 10 type 1) in 22 cases, osteonecrosis of the femoral head in 5 cases, and inflammatory arthritis in 3 cases. The proportion of these diseases was usual among patients receiving THA in Japan. According to preliminary results, a sample size of 14 patients was needed to achieve a power of 80% for comparison between different offsets. 11 Twenty patients were recruited in a similar previous study. 12 In consideration of additional comparison between different head sizes, the authors recruited 30 patients in this study.
Surgeries were performed using a posterior approach in a lateral decubitus position with the patient securely positioned using a pelvic positioner (Innovative Medical Products, Plainville, CT, USA). The Super Secur-Fit™ HA hip system (Stryker, Mahwah, NJ, USA) was used in all cases. The femoral side was prepared first. As a general rule, the acetabular shell was fixed in an abduction angle of 40° and in an anteversion angle decided in accordance with the anteversion angle of the final femoral broach.
After the insertion of the final femoral broach and the fixation of the acetabular shell, trial reduction was repeated using provisional femoral heads and necks and provisional acetabular liners. The provisional neck with a neck-shaft angle of 132° (“standard-offset neck”) or 127° (“high-offset neck”) was combined with the provisional head in diameters of either 26 mm or 32 mm. Depending on the stem size, the high-offset neck had a 5- to 8-mm larger offset than the standard-offset neck (Figure 1). A 3- or 4-mm longer neck was used for the 127° neck to equalize the vertical height of the neck, evaluating exclusively the effect of femoral offset by eliminating the effect of leg length on soft-tissue balance. In no case, a head with an extended flanged neck was used. According to the manufacturer, the 32-mm heads with this system had approximately 5° greater maximum oscillation angle than the 26-mm heads (e.g. 125° for a 32-mm head and 120° for a 26-mm head when a #7 stem, a +0-mm neck, and a flat liner were used). During the period of the study, the 26-mm head was used most frequently for THA, and the 32-mm head was the largest size available in this implant system.

Femoral broaches with a high-offset neck (127° neck-shaft angle, left) and a standard-offset neck (132° neck-shaft angle, right). The high-offset neck had a 5- to 8-mm larger offset (a) than the standard-offset neck (b).
Joint stability was evaluated intraoperatively using trial reduction instruments. To evaluate the joint stability against posterior dislocation, internal rotation (IR) was forced manually, and the limit of range of IR prior to subluxation was measured at 45° and 90° hip flexion, neutral hip abduction/adduction, and 90° knee flexion. 8 Subluxation was predefined as the point at which the head began to lose total contact with the liner surface and was determined by palpation and inspection independently by one of the authors (TJ). When the head was in subluxation, it was checked to see if there was prosthetic impingement between the neck and the liner. Additionally, the range of external rotation (ER) was also measured. It was measured at 0° hip extension and 90° knee flexion but, after the measurement, ER was forced again at hip hyperextension and 0° knee extension to test anterior instability.
Measurement of the range of IR and ER was done independently by another one of the authors (DK) using a goniometer with one arm on the tibia and the other perpendicular to the floor by gravity (to measure the supplementary angle of the range of IR and ER). The data were statistically analyzed using analysis of variance and paired t-tests. The data of 26-mm head-/standard-offset group was used as a control, and the data from the cases of 32-mm head/standard offset, 26-mm head/high offset, and 32-mm head/high offset were compared with the control. Accuracy of intraoperative positioning of the acetabular shell was evaluated by comparing the postoperative measurement of the angles of cup abduction and anteversion using an anteroposterior radiograph and a computed tomography image. 13
Results
The result of range of IR and ER of each group is shown as an average and a standard deviation (Figure 2). The average range of IR to subluxation of all the cases was 68.4 ± 17.1° at 45° hip flexion and was reduced to 46.8 ± 13.4° at 90° hip flexion. The average range of ER was 37.3 ± 7.7°. None of the hips in any group ended in anterior subluxation by ER. The head size did not affect the range of IR and ER significantly, whereas the femoral component offset did affect it significantly (p = 0.03). The average ± standard deviation of difference of range of IR and ER compared with the control (26-mm head/standard neck) is shown in Figure 3.

Range of IR to subluxation at 45° and 90° hip flexion, and range of ER at 0° hip flexion/extension, shown as an average and a standard deviation. None of the hips ended in subluxation by ER. Std: standard offset; High: high offset; IR: internal rotation; ER: external rotation.
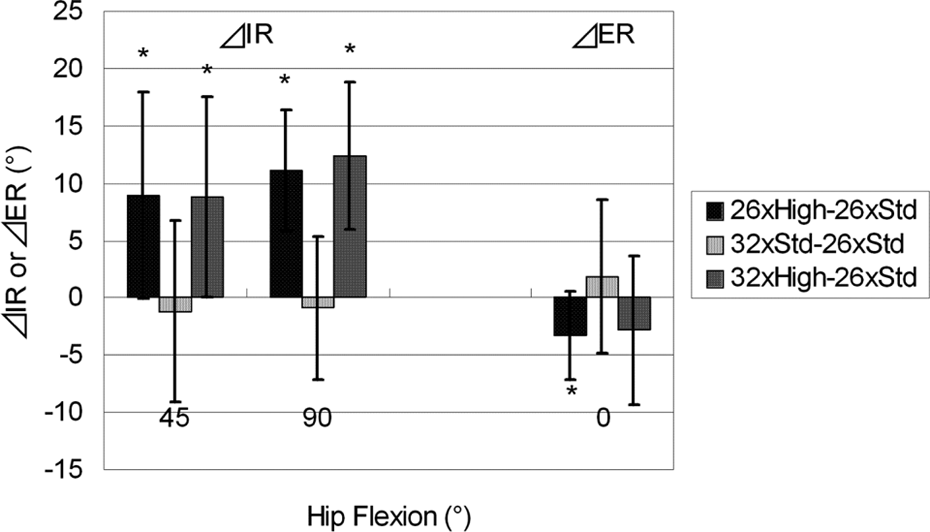
Increase of range of IR (ΔIR) and ER (ΔER) compared with the group of 26-mm head and standard-offset neck, shown as an average and a standard deviation. Std: standard offset; High: high offset; IR: internal rotation; ER: external rotation. * p < 0.01.
Increasing the head diameter from 26 mm to 32 mm did not improve the range of IR, whereas increasing the offset improved the range of IR significantly (p = 0.0009). Increasing the offset achieved approximately 10° more IR on average, whether in combination with the 26-mm head or the 32-mm head. Conversely, increasing the offset decreased the range of ER significantly (p = 0.008).
By intraoperative inspection, it was revealed that the posterior subluxation occurred without apparent prosthetic impingement but most likely with osseous impingement, except with two hips that each had a 26-mm head. Positions of the acetabular shells were considered to be within appropriate and intended range (Figure 4). None of the hips in this study had postoperative dislocation.

Distribution of cup position.
Discussion
In this study, the theoretical advantage of a larger head size was not demonstrated, while a high-offset neck apparently improved the joint stability. Reasons that the head size did not have a significant effect on the stability would include that the difference of oscillation angle between 26-mm and 32-mm heads was so slight (approximately 5°) that the small difference of range of IR could not be detected. Another reason could be related to the intraoperative findings that the primary cause of subluxation was not the prosthetic impingement, but was most likely the osseous impingement between the greater trochanter and the pelvis with intervening soft tissue. Bartz et al., using a cadaveric THA model where the acetabular component was fixed in 20° of anteversion and 45° of inclination, showed that increasing the head size from 28 mm to 32 mm did not significantly increase the range of motion because of limitation of joint motion by the osseous impingement. 14 The most frequent cause of dislocation was the osseous impingement with the 32-mm head, while it was the prosthetic impingement with the 22-, 26-, and 28-mm heads in their study. In the present study, the primary cause of dislocation was the osseous impingement, even with the 26-mm head, and it might have been related to our surgical procedure. We prepare the femoral side first prior to acetabular side to decide the cup anteversion in accordance with the anteversion of the final femoral broach and to achieve the maximum range of motion without prosthetic impingement. When the implants are situated in a proper position and the implant system with a sufficient oscillation angle is used, it is likely that the osseous impingement occurs in advance of the prosthetic impingement. Thus, the result of this study may also be explained by saying that the 26-mm head of this implant system was large enough to prevent prosthetic impingement within the osseous impingement-free range.
In cases where the prosthetic impingement occurs prior to the osseous impingement, for example, cases with implant malposition, such as inadequate anteversion of the cup and/or the stem, the large head might be more effective to prevent prosthetic impingement. With highly abducted acetabular component orientation, however, it has been pointed out that the use of the large head can result in little contribution to joint stability. 15
In addition to the greater oscillation angle of the larger head, the greater amount of transposition of the larger head needed for dislocation can provide improved joint stability. 4,15 –17 In this study, we chose the point of subluxation, not the complete dislocation, for measurement of the range of IR as a parameter to evaluate the instability. Sultan et al. reported that a 32-mm head provided significantly greater (8°) IR compared with a 28-mm head using an intraoperative evaluation method similar to ours, but they determined the instability using the point at which “the head began riding out of the liner.” 12 We also have found that when the range of IR was measured by dislocation point, the 32-mm head achieved a significantly greater range than the 26-mm head due to increased head transposition after subluxation before complete dislocation. 18 However, this is apparently not an ideal mechanism to improve joint stability, because there should be excessive stress concentration in the articular surface while the head is in subluxation within the acetabular liner. 15,19
Previous studies have shown favorable effects of the femoral offset on postoperative hip abductor function 20,21 and polyethylene wear. 22 Although theoretical effects of the femoral offset on joint stability also have been suggested, 8,17 previous clinical studies have failed to show the effects of femoral offset on postoperative dislocation rate. 1,9,23 In the present study, the femoral offset, unlike the head size, had a significant effect on the joint stability. This also would be related to the fact that, in most of the cases, the subluxation occurred without prosthetic impingement but with osseous impingement. The increase of femoral offset results in posterolateral displacement of the femur with reference to the acetabular cup and the pelvis. This would lessen the likelihood of osseous impingement between the proximal femur and the pelvis at IR of the hip, 8 and thus would contribute to the enhanced stability with the larger offset in this study. Furthermore, it is possible in the clinical situation that abductor strength increased by lengthening the functional lever arm 20,21 also enhances the joint stability postoperatively. 8 In this study, ER caused none of the hips to dislocate anteriorly. However, the range of ER was decreased with the high-offset neck, probably due to tightness of anterior capsule of the hip joint, which was usually intact through the posterior approach. Should the limitation of ER be found to be severe intraoperatively, incision or resection of the anterior capsule would improve the range of ER.
There were some limitations to this study. Stability was evaluated under anesthesia and before soft-tissue repair. Repair of the posterior capsule and the short external rotators, known to be effective for prevention of dislocation when a posterior approach is used, 24 may be difficult if the greater trochanter is over-lateralized with a high-offset stem. The cup size could also be an implant-related factor predisposing a hip to dislocation, 1 but that could not be assessed in this study because the cup sizes did not range widely enough due to the generally smaller acetabulae of Japanese patients compared with those of Caucasians. For the same reason, we could not investigate the stability by testing on a greater range of femoral offset and head size, such as 36 mm or 40 mm, which has become available recently. Although the larger heads may improve joint stability, they also may cause problems such as risk of thin polyethylene liner fracture, soft-tissue impingement resulting in groin pain, and fretting and corrosion damage at the head–neck taper leading to adverse reactions to metal debris. 4 The measurements of range of motion by a goniometer could have been subject to error, and it might be another limitation of this study, especially in evaluation of the effect of head size, since the difference of oscillation angle between 26-mm and 32-mm heads was small. It would be more precise if the measurements and the hip positions were confirmed by a navigation system. However, errors in the data of difference when compared with 26-mm head/standard offset (Figure 3) could have been minimized because of consecutive, repeated measurements for each case. Finally, the majority of the patients in this study have dysplastic hips. Dysplastic hips have wider variety of anatomy including acetabular version and femoral version than the normal hips. 25 The results of impingement analysis and variation of cup positions in this study were likely to be affected by the anatomical variation, and thus, the result of this study may be less applicable to other etiologies.
Adequate restoration of the femoral offset is an important but complex issue. 8 Multiple factors other than stability also should be considered in deciding the femoral offset. 20 –22,26 Moreover, the anatomical restoration of the femoral offset is often complicated by inherent anatomical abnormalities, especially when the hip is dysplastic as is seen often in secondary osteoarthritis. 27 From a standpoint of hip instability, however, this study indicated that a longer femoral component offset might be more effective than a larger head size in preventing instability after primary THA via a posterior surgical approach. In an intraoperative situation where the joint is not considered as stable enough, the femoral offset should be evaluated, and the use of high-offset femoral stem can be a helpful option.
Footnotes
Acknowledgment
The authors thank Drs Kenichi Shinomiya and Masaaki Matsubara for their clinical support during this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.