
Abstract
Objective:
This study evaluated the efficacy of surgery for femoral neck fractures in children after a 24-h delay and the factors affecting the risk of complications.
Methods:
The study included 16 children who underwent surgery after the first 24 h for femoral neck fractures. According to Delbet’s classification, there were 2 type I, 11 type II, and 3 (four hips) type III cases. The mean time from injury to surgery was 85 h (range 27–240 h). According to Garden’s classification, there were 1 type II, 14 type III, and 1 type IV (two hips) cases. Initial surgery consisted of closed reduction and hematocele drainage with a 20-mL needle tube. If the procedure failed, open reduction was performed. Internal fixation (K-wire pinning, screw) was performed after closed (n = 9) or open (n = 8) reduction. The results were assessed using the Ratliff criteria after a mean follow-up of 23.2 months. Patient age, type of fracture, complications, treatment, and avascular necrosis (AVN) were evaluated.
Results:
The results were good in 15 hips (88.2%) and fair in 2 hips (11.8%, one type II case with closed reduction and one type I case with open reduction). The most frequent complication was AVN (4 of 17; 23.5%; three Ratliff good and one fair), which was significantly related to poor outcomes. AVN occurred in one hip in the closed reduction group (Delbet’s type II, 12.5%) and in three in the open reduction group (one Delbet’s type I, 50%; two Delbet’s type II, 66.7%). There were no significant differences in the time from injury to operation (27, 54, 64, and 116 h) and AVN incidence or Ratliff criteria.
Conclusions:
The efficacy of delayed reduction fixation of the femoral neck was better in the closed reduction group than in the open reduction group. Fracture location closer to the femoral head and older age affected the incidence of AVN.
Introduction
Pediatric femoral neck fractures are exceedingly rare and account for less than 1% of pediatric fractures and adult femoral neck fractures; most of these fractures are caused by high-energy trauma, such as traffic accidents or a high fall. 1,2 These fractures are associated with high rates of premature physeal closure, delayed union, coxa vara, lower limb length discrepancy, and avascular necrosis (AVN) without internal fixation. 3 There are no effective treatments for AVN, and proper primary treatment of this hazardous fracture is the key to a successful outcome. Surgery is recommended within 24 h after injury (even in 12 h) to avoid AVN. 4 However, in China, many parents and some doctors do not pay enough attention to pediatric femoral neck fractures, and patients often present at the hospital more than 24 h after the injury. We share our experience and understanding of this fracture by retrospectively reviewing 16 patients who underwent surgery for femoral neck fractures in our institution after the first 24 h and analyze the effects of age, fracture type, delayed hours, and surgery type. The patients were treated with closed or open reduction and internal fixation and underwent conservative management in spica.
Patients and methods
Patients
We retrospectively reviewed all children with femoral neck fractures treated in our department between September 2010 and December 2015. Sixteen children (17 hips, 10 boys and 6 girls, 1–14 years, mean 10.4 years) who completed a mean follow-up of 23.2 months (range 10–58 months) were included in the study (Table 1). Patients underwent surgery at 27–240 h (mean 85 h) after the injury. Written consent for participation in this retrospective study was obtained from the parents we were able to contact at the time of drafting the study.
The demographics of each patient.

AVN: avascular necrosis.
Treatments
The fractures were classified according to Delbet’s system, as described by Colonna. 5 The treatment modalities used were conservative management, open reduction and internal fixation (ORIF), or closed reduction and internal fixation (CRIF), depending upon the patient profile and fracture pattern.
Assessment
The final outcome was assessed at the last follow-up visit using Ratliff’s method. A good outcome was rated as a “satisfactory outcome,” and “fair” and “poor” outcomes or the presence of complications were rated as an “unsatisfactory outcome.” Radiographs were also evaluated for joint congruency, arthritic changes, neck-shaft angle, and AVN, which was further classified according to Garden’s classification (Table 2) 6 and Ratliff’s classification (Table 3). 7
Garden’s classification for clinical and radiographic assessment.

Ratliff system of clinical and radiographic assessment.

AVN: avascular necrosis.
Statistical analysis
Data were analyzed using the Student’s t-test with SPSS 19.0. Differences with p value <0.05 were considered statistically significant.
Results
General clinical data
As presented in Table 1, of the 16 cases (17 hips), 2 were type I (transepiphyseal separation; two ORIF), 11 were type II (transcervical; three ORIF and eight CRIF), and 3 were type III (cervicotrochanteric; four hips, two ORIF, and two CRIF). There were no cases of Delbet’s type IV (intertrochanteric). According to Garden’s classification of femoral neck fractures, 1 was type II (without displacement), 14 were type III (partial displacement), and 1 was type IV (two hips, total displacement). The mechanisms of injury included traffic accidents in three cases, falls (falls from height) in four, slips (slip or fall) in eight, and reason unknown in one case. All the 16 fractures underwent surgery ≥24 h after injury because of delayed arrival at the hospital and extensive associated injuries.
Of the 16 fractures, the associated injuries included pubic fracture in one; olecranon, supracondylar humeral, and pubic fractures in one; skull and pubic fractures in one; and ilium, thoracic vertebral fractures, pneumothorax, and pulmonary contusion in one.
Outcomes of the two treatments
Displaced fractures were treated by CRIF under fluoroscopy or by open reduction if closed anatomical reduction failed after three attempts. The Watson-Jones approach or Smith-Petersen approach was used, and patients underwent internal fixation after reduction. The patients began to move in bed and walked at 2 months after lying in the bed in a hip cast.
According to the Ratliff classification, 15 hips had satisfactory outcomes and two hips had fair outcomes (one case of CRIF, Delbet’s type II; one case of ORIF, Delbet’s type I); there were no poor outcomes.
AVN incidence in the patients undergoing CRIF or ORIF
As presented in Table 4, four hips (23.5%) developed AVN. Of the four AVN cases, three hips had Ratliff good outcomes and one case had a Ratliff fair outcome. In the CRIF group, one hip developed AVN (Delbet’s type II, Garden’s type III, 1/9 hips, 11.11%). In the ORIF group, three hips developed AVN (3 of 8 hips, 37.50%), of which one was Delbet’s type I or Garden’s type II (1 of 2 hips, 50%) and two were Delbet’s type II or Garden’s type III (2 of 3 hips, 66.7%).
The AVN incidence in the treatment of CRIF or ORIF.

AVN: avascular necrosis; CRIF: closed reduction and internal fixation; ORIF: open reduction and internal fixation.
a p Value <0.05 compared with CRIF group.
Correlation between time from injury to operation and AVN incidence
In patients who developed AVN, the interval times from injury to operation were 27, 54, 64, and 116 h (Table 5). There was no statistically significant correlation between the outcome and the occurrence of further AVN, or low Ratliff score and interval time.
The correlation between duration from injury to operation and AVN incidence.

AVN: avascular necrosis.
Correlation between Delbet’s type or Garden’s type and complications (hips)
There was a significant correlation between the type of fracture and the outcome. A smaller distance between the fracture and the femoral head was correlated with a higher rate of AVN. Delbet’s type I or Garden’s type II fractures had the worst outcomes and the highest incidence of AVN (Table 6).
The correlation between Delbet’s type or Garden’s type and complication (hips).
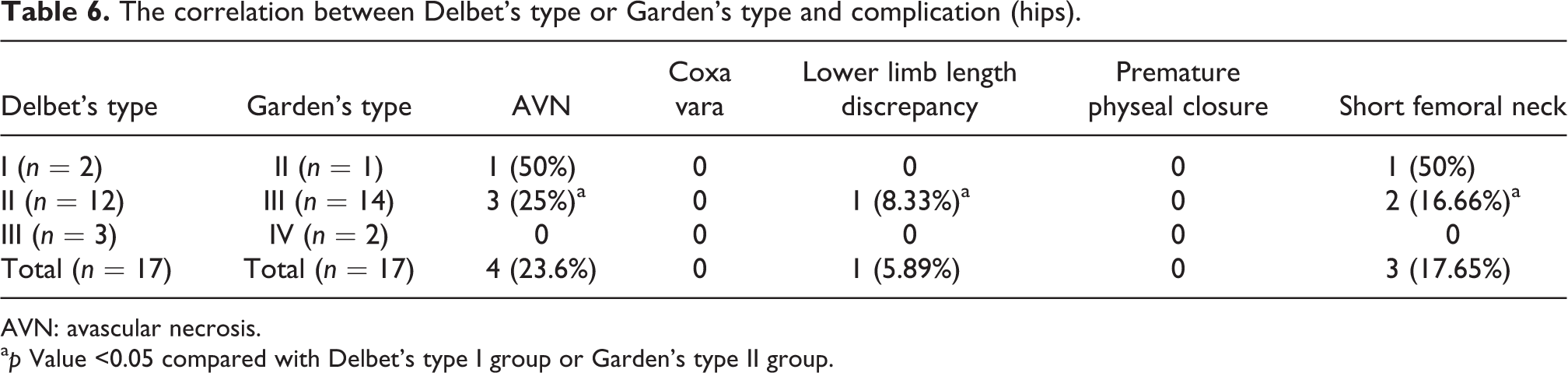
AVN: avascular necrosis.
a p Value <0.05 compared with Delbet’s type I group or Garden’s type II group.
Correlation between age and AVN incidence
One hip developed AVN in the 1- to 8-year group (six hips, mean 5.67 years), and the incidence was 16.67%; three hips developed AVN in the 11- to 13-year group (11 hips, mean 12.72 years), and the incidence was 27.27% (Table 7).
The correlation between age and AVN incidence.

AVN: avascular necrosis.
Discussion
Femoral neck fractures in children are caused by high-energy trauma because the femoral neck of children is dense and hard compared with the adult femoral neck. 1 Femoral neck fractures are believed to have a better outcome when they are treated by early reduction and internal fixation after injury, and some researchers suggest that surgery should be performed within 12 h. 8 However, patients and doctors often do not consider pediatric femoral neck fractures as an emergency, and because of distance from the hospital or other concomitant injuries, many patients present at the hospital more than 24 h after injury. There is no consensus regarding the treatment of these injuries or the factors affecting outcomes. These fractures are relatively rare in children, and long-term follow-up is difficult. Collecting sufficient data on these fractures is difficult because there are few reports on delayed management of pediatric femoral neck fractures. This retrospective study focused on the factors affecting the outcomes, such as age, delayed interval time, fracture type, and CRIF/ORIF.
The incidence of AVN ranges from 70% to 100% in type I fractures. 9,10 Moon and Mehlman 11 reported that the incidence of AVN decreases from type I (38%) to type II (28%), type III (18%), and type IV (5%). Type I AVN represents the most serious condition and is associated with a poor prognosis. The location of the fracture contributes to the risk of developing AVN, and fractures closer to the femoral head are more likely to develop AVN. In the present study, the correlation between the incidence of AVN and fracture type was consistent with the results reported by Moon et al. (type II 25% and type III 0%). However, the incidence rates were lower than those reported by Moon, which could be attributed to factors such as internal fixation and rigid external fixation. 12,13
Blood flow to the pediatric femur head has specific characteristics. 1,2,14 In infants, the metaphyseal artery from arteriae circumflexae femoris lateralis and arteriae circumflexae femoris medialis passes through the femoral proximal epiphyseal growth plate and supplies femoral head. At 2 years of age, the metaphyseal artery cannot pass through the growth plate, and the basilar artery from the arteriae circumflexae femoris lateralis and arteriae circumflexae femoris medialis supplies the femoral head. The basilar artery is in the boundary within the bone rather than within the joint capsule, which on injury leads to AVN. At 4 years of age, the lateral epiphyseal arteries from the deep branch of the medial circumflex femoral artery supply the femoral head. In children older than 8 years, the round ligament of the femur passes through the femoral head to connect the epiphyseal artery and supply blood to the femoral head surface, not to the femoral head. Therefore, even in minimally displaced fractures, the arteries around the femoral head are exposed to increased intracapsular pressure, which may compromise blood flow to the femoral head through a tamponade effect. 15 To determine whether the displacement degree of femoral neck fracture is related to AVN, we used Garden’s classification and found that although the femoral neck displacement was the most serious in one patient (two hips) with Garden type IV, AVN did not occur because Delbet III was located at the base of the femoral neck and had no effect on the femoral neck blood supply ring. The displacement of children with Garden II and III was not as severe; however, the corresponding Delbet classification was types I and II, and the blood supply ring of the femoral neck was destroyed. These cases developed AVN, which also indicates that AVN is mainly caused by the vulnerability of the blood supply to the femoral head and neck.
In delayed surgery for femoral neck fractures, it is difficult to determine whether to perform CRIF or ORIF. Researchers differ regarding the optimum type of operation. The incidence of AVN is lower and efficacy is better in ORIF because ORIF reduces the pressure in the hip capsule and promotes recovery of blood circulation. 16 –19 However, there are few cases of surgery performed 24 h after injury. Other scholars report that CRIF is better than ORIF because open reduction can destroy the blood supply to the femoral head. 20
Many scholars support that femoral neck fractures should be treated within 24 h. 21 The risk of AVN increases with increased time after injury. However, whether the increased incidence of AVN is proportional to delayed fracture reduction time remains unclear. In the present study, the incidence of AVN was not proportional to delayed time in operations performed at 24 h after injury. We speculate that because the femoral neck blood supply is destroyed after 24 h, the risk of AVN does not differ in surgeries performed after 24 h, although this needs to be verified in future studies.
Previous studies showed that age is a statistically significant predictor of outcome, and older children have a 1.14-fold higher likelihood of developing AVN for every year of increasing age. Therefore, the incidence of AVN should be 2.82-fold higher (47%) in patients aged 12.67 years than in those aged 5.67 years. 11 In the present study, the incidence was 1.5-fold higher, suggesting that older children were more likely to develop AVN, but the incidence was not as high as that reported previously.
The results of our statistical analysis validate previous observations that specific risk factors can predict the occurrence of AVN. Fracture type, displacement, age, and treatment may all contribute to the development of AVN. Older children with type I and II fractures are at the highest risk for developing AVN. This was a retrospective study, and the treatment option for closed reduction depended on the fracture characteristic, and the treatment was not randomized. The efficacy of delayed reduction and fixation of the femoral neck was better in the closed reduction group than in the open reduction group. This may be related to the fact that the closed reduction group was preselected by the fracture characteristics as a group with a better outcome. The probability of a fracture location closer to the femur head, a higher incidence of AVN, and a poor prognosis increased with age. There were no correlations between delayed reduction fixation and high AVN incidence or other severe complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.