
Abstract
Purpose:
The purpose of this study was to determine the effect of low-pressure and pulsed lavage irrigation on suture knot security.
Methods:
Ninety-tied suture loops were measured for baseline circumference and then subjected to no irrigation, bulb syringe irrigation, or pulsed lavage irrigation. The sutures were placed under a load and then measured for final circumference. A larger circumference difference indicated poorer knot security.
Results:
There was a statistically significant difference in the knot security between all three groups (p < 0.001). Pulsed lavage resulted in the greatest circumference increase (0.52 ± 0.19 mm), followed by bulb syringe (0.24 ± 0.18 mm), and lastly no irrigation (0.08 ± 0.00 mm). None of the groups had any catastrophic failures. No knots met the predetermined criteria for knot failure.
Conclusion:
Pulsed lavage irrigation resulted in a statistically significant decrease in suture knot security as compared to bulb syringe irrigation and no irrigation. None of the groups met the currently accepted criteria for clinical suture failure, which has a relatively arbitrary value. While the available literature does not discuss increases in loop circumference for specific orthopedic applications, this small difference suggests that pulse lavage is unlikely to have a clinically significant impact on the suture integrity for most orthopedic procedures.
Introduction
Successful open surgery requires tissue healing and the maintenance of the structural integrity of repaired soft tissues. An effective and reliable suturing technique is essential to ensure secure tissue approximation and fixation until healing occurs and involves both knot security and loop security. Loop security is the ability to maintain the diameter of the suture loop once the knot is tied. 1 Knot security is defined as the effectiveness of the knot to resist slippage and breakage when a load is applied. 2,3
During open surgeries, wound irrigation is commonly performed to decrease the concentration of particulate matter, debris, and infectious organisms in the surgical field on the implanted hardware and in the wound bed. Multiple delivery methods for irrigation fluid exist and are commonly used. Pulsed lavage is a high-pressure irrigation technique, differing from more low-pressure methods such as gravity lavage and bulb syringe irrigation. Pulsed lavage has been shown to provide greater cement penetration and interface strength in total knee arthroplasty (TKA), decrease the concentration of bone and other material debris in the surgical field, and remove bacteria from the surgical field. 4 –9 Nonetheless, there are drawbacks to using pulsed lavage, including high rebound bacterial contamination. 10 The high pressure of pulsatile lavage causes increased depth of bacterial penetration and greater deep bacterial retention in soft tissue when compared with low-pressure lavage. 11 In addition to soft tissue damage, pulsed lavage can result in increased macroscopic and microscopic damage to bone. 9,12,13
There has been extensive research on the variability of knot and loop security with differing suture material, knots, and number of throws. However, to our knowledge, the effect of pulsed lavage irrigation on the knot security has not been established. Since suture repair of soft tissue and high-pressure irrigation are both commonly employed techniques in open orthopedic surgery, it is important to determine if pulsed irrigation has a negative effect on the knot security.
In this experiment, we studied the effects of low-pressure bulb syringe irrigation and high-pressure pulsed lavage irrigation on the knot security. We hypothesized that the knot security, manifested as the post-intervention to pre-intervention loop circumference difference, of sutures that undergo pulsed lavage will be worse than both sutures that remain dry throughout the experiment and sutures that undergo low-pressure bulb syringe irrigation.
Methods
Ninety braided ultra-high-molecular-weight polyethylene sutures (Arthrex #5 FiberWire, Naples, FL, USA) were divided into three groups. The control group consisted of 30 sutures that remained dry throughout the experiment. The bulb syringe group had 30 sutures that underwent bulb syringe irrigation between pre-intervention and post-intervention measurements. The remaining 30 sutures (pulsed group) received pulsed irrigation between pre-intervention and post-intervention measurements.
Similar to previous studies, all sutures were tied on a 30 mm post using the Fundamentals of Arthroscopy Surgery Training Workstation (FAST) workstation.3 , 14,15 All sutures were hand tied with the standard knot routinely used during our repair of lesser tuberosity osteotomies during shoulder arthroplasty surgery. The knot consists of two underhand half hitches followed by an overhand half hitch on the same post, subsequently backed up with three square knots (Figure 1). All knots were tied by the same orthopedic surgery resident (AG) under the direct supervision and instruction of the senior author (DS), a fellowship-trained shoulder and elbow orthopedic surgeon. The six throws utilized in this knot are in accordance with a study that recommended FiberWire be tied with this number of throws for optimal knot security. 16 A tensiometer was used to ensure a consistent amount of tension during knot tying (Figure 2). This tension, 22 N, was determined prior to the experiment to be the normal tension used by the senior author when performing hand suturing.

Sutures were hand tied with the standard knot used during repair of lesser tuberosity osteotomies during shoulder arthroplasty surgery: (a, b) two underhand half hitches followed by an overhand half hitch on the same post, and (c, d, e) subsequently backed up with three square knots.
Using a 30 mm post on the FAST workstation to tie the sutures with lesser tuberosity osteotomy (LTO) knots. The tensiometers were used as shown to ensure a consistent tension of 5 lb throughout knot tying.
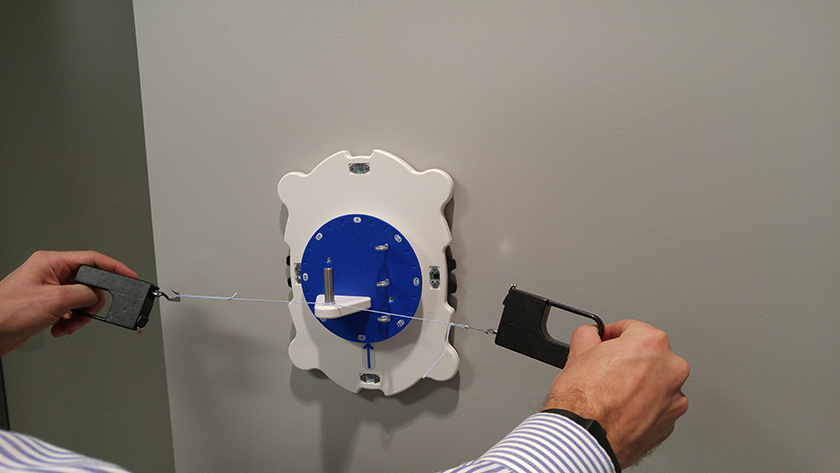
The initial loop circumference was measured to the nearest quarter millimeter on the FAST conical loop sizer (pre-intervention circumference, C Pre); this is a measure of loop security (Figure 3). The amount of suture stretching determines the knot security. After initial measurements, the control group remained dry without irrigation, the bulb syringe group underwent bulb syringe irrigation with 30 cc of water, and the pulsed lavage group underwent 20 s of pulsed lavage irrigation using a Stryker InterPulse pulsed irrigator (Kalamazoo, MI, USA) (Figure 4). These parameters were determined to be the normal amount of volume or time a knot would be exposed to irrigation during a typical surgical procedure. Then, as performed by Pedowitz et al., 15 all groups were tensioned to 15 lb (60 N) for 15 s using the FAST knot tester (Sawbones, Vashon Island, WA, USA) (Figure 5). This measuring device and parameters have been used in a previous study to measure the knot security. 15 The board was determined to have reproducible tension, generating 15.03 lb with a standard deviation of 0.05 lb with two independent operators. After tensioning, the loop circumference of the sutures was measured again (post-intervention circumference, C Post). The difference between the pre-intervention circumference and post-intervention circumference (Diff) was determined. In accordance with the previous studies, we defined the knot failure as 3 mm or greater increase in suture circumference after load application. 17 –21

Using the FAST conical loop sizer to measure the loop circumference of the Arthrex #5 FiberWire that was tied on a 30 mm post on the FAST workstation. Each marker (moving downward) indicates an increase in loop circumference by 0.5 mm. We set the first marker to be equivalent to a baseline circumference of zero. The loop circumference was measured prior to applying tension and irrigation (C Pre) and after to applying tension and irrigation (C Post), and the difference was calculated (C Post − C Pre).

Using the Stryker InterPulse pulsed irrigator to irrigate the knot with water. Each knot in the pulsed lavage group was subjected to irrigation for 20 s, and then tensioned to 15 lb for 15 s with the FAST knot tester.

Using the FAST knot tester to tension the knots to 15 lb (60 N). Tension was held for 15 s, as performed by a prior study (20). The knots were either tensioned immediately after initial circumference measurement for the control group, after bulb syringe irrigation with 30 cc of water for the bulb syringe group, or after 20 s of pulsed lavage irrigation in the pulsed lavage group.
Statistical analysis
Students t tests were used to compare the mean differences between groups. The statistical significance was considered p < 0.05.
Results
Pulsed lavage resulted in the greatest circumference increase (0.52 ± 0.19 mm), followed by bulb syringe (0.24 ± 0.18 mm), and lastly no irrigation (0.08 ± 0.00 mm). The knot security was statistically worse in both bulb syringe irrigation (p < 0.001) and pulsed lavage irrigation groups (p < 0.001) when compared to the control group. The knot security of the pulsed lavage irrigation group was also worse compared to the bulb syringe irrigation group (p < 0.001; Figure 6). None of the sutures failed in tension or exceeded the loop circumference difference threshold of 3 mm.

Box and whisker plot of pre-intervention to post-intervention loop circumference differences. Boxes include the middle two quartiles of data, and whiskers indicate the minimum and maximum, if not contained within the box. Points above and below the “wet” box indicate outliers. *Mean difference of dry group was statistically less than wet group, p < 0.001. †Mean difference of dry group was statistically less than Pulse group, p < 0.001. §Mean difference of wet group was statistically less than Pulse group, p < 0.001.
Discussion
Suturing necessitates the knot security and loop security. The loop security is the ability to maintain the suture loop once the knot is tied. 1 The knot security is the ability of the knot to resist slippage and breakage when a load is applied. 2,3 The knot security is affected by the slack between throws, friction coefficient of the suture, and suture pliability. 1 The knot security and loop security are mutually exclusive; a knot can have adequate knot security but poor loop security and be unable to approximate the wound edges. 2
Wound irrigation is performed in most, if not all, open orthopedic procedures and is used to decrease the concentration of particulate matter, debris, and infectious organisms in the wound bed. Proper wound healing can only occur below a critical bacterial count of 100,000 organisms per gram; above this critical level, wound sepsis occurs and wound healing is significantly more difficult. 22 Pulsed lavage is a high-pressure irrigation technique, differing from more low-pressure methods such as gravity lavage and bulb syringe irrigation. In TKA, pulsed lavage allows greater cement penetration and interface strength (requiring higher pull-out forces) during tibia preparation. 4 –6 Similar findings have been described in unicompartmental knee arthroplasty, where pulsed lavage increases cement penetration, leading to decreased implant subsidence and micromotion. 7 Using pulsed lavage also decreases the concentration of bone and other material debris in the surgical field. 5
Pulsed lavage has been shown to effectively remove bacteria from the surgical field. Mote and Malay demonstrated that pulsed lavage and debridement were successful in 69.86% of 73 surgical patients with lower extremity wounds in decreasing bacteria between the immediate pre-lavage and post-lavage gram stain and cultures. 8 This finding has been substantiated by multiple other studies, showing that pulsed irrigation removes bacteria from contaminated bone and leads to reduced size and faster healing of chronic wounds. 9,23 Since the efficacy of wound irrigation correlates with the irrigant pressure, there are many benefits of using pulsed lavage compared to low-pressure irrigation. Although low-pressure irrigation is efficacious in removing bacteria from wounds and surgical sites, several studies have shown that pulsed irrigation is even more effective in removing bacteria from surgical wounds and orthopedic implants, compared to low-pressure irrigation, even when using less irrigant. 10,24 –26
Nonetheless, there are drawbacks to using pulsed lavage. Owens et al. demonstrated that although both pulsed lavage were effective in initially removing bacteria, bacterial contamination of the wound after 48 h was significantly higher in the pulsed lavage patients compared with low-pressure irrigation. 10 The authors concluded pulsed lavage may not result in the best clinical outcomes due to rebound bacterial contamination. Other authors question the clinical significance of decreased bacterial load. Urish et al. found only a 10-fold reduction in biofilm mass of TKA components, which is still a large enough bioburden to cause periprosthetic infection. 27 Furthermore, the high pressure of pulsatile lavage causes increased depth of bacterial penetration and greater deep bacterial retention in soft tissue when compared with low-pressure lavage. 11 In long bone fractures, this may increase bacterial propagation down the intramedullary canal. 28 This high pressure can also lead to increased penetration of particulate matter and deeper cellular death compared with low-pressure lavage. 29,30 In addition to the soft tissue damage, pulsed lavage can result in increased macroscopic damage to bone, including cortical fissures and periosteal separation. 9 Other studies suggest that high-pressure irrigation can lead to the differentiation of mesenchymal stem cells toward the adipocyte lineage, which may lead to nonunion and delayed union in long bone fractures. 12 Dirschl et al., using a rabbit femur model, found that pulsatile lavage had a detrimental effect on early new bone formation after fracture. 13
To our knowledge, this is the first study investigating the effect of pulsed lavage on the knot security. We demonstrated that pulsed lavage led to a decrease in the knot security compared with both low-pressure irrigation and a control group with no irrigation. During irrigation and loading, the suture can either stretch internally (intrinsic laxity) or can stretch further due to knot slippage. The significant difference between the control and bulb syringe irrigation groups may be attributed to both intrinsic laxity and knot security. Exposing the suture to water may have resulted in lengthening of the suture, and the relative contributions of intrinsic laxity and knot security to the overall difference cannot be determined. The same can be said of comparing the control and pulsed lavage groups. However, when comparing the bulb syringe and pulsed lavage groups, hydration of the suture was controlled for and the difference can be attributed solely to a detrimental effect of pulsed lavage on the knot security.
The mean loop circumference difference in the pulsed lavage group was 0.52 mm, well below the currently accepted threshold of 3 mm increase in suture circumference for detrimental clinical results. This number has been commonly used as a marker of clinical failure because this increase in loop circumference results in the loss of tissue apposition. 17 –21 However, this threshold is relatively arbitrary and may not be applicable to all orthopedic applications, such as repairing the lesser tuberosity osteotomy in total shoulder arthroplasty, performing a humeral suspension procedure in shoulder girdle malignancies or closing an arthrotomy for TKA. 31,32 Nonetheless, this small difference suggests that pulse lavage is unlikely to have a clinically significant impact on the suture integrity for most orthopedic procedures.
There are some limitations to this study. First, investigators were not blinded to the intervention. Sutures were irrigated with water as opposed to saline, blood, or plasma. However, it is currently unknown if using water as opposed to these other irrigants has any effect on the suture intrinsic laxity or knot security. Third, intrinsic laxity—a property unique to each suture material and size, defined as the change in end-to-end distance when applying a given force to an untied suture—was not measured in this study. 3 However, as mentioned previously, the effect of the suture hydration on intrinsic laxity was controlled for when comparing the bulb irrigation and pulsed lavage groups. Nonetheless, a measurement could provide insight into the relative contributions of the knot security and intrinsic laxity when comparing the control and irrigation groups. Lastly, this study investigated the effect of pulsed lavage on the knot security using one combination of suture, knot, and pulsed lavage irrigator commonly utilized at our institution during total shoulder arthroplasty and other common open orthopedic surgical procedures for repair of soft tissues. More studies are needed to determine if the effects seen in this study are reproducible and generalizable with other combinations.
Footnotes
Authors’ note
This study was performed at Loyola University Medical Center, 2160 South First Avenue, Maywood, IL 60153.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.