
Abstract
Study design:
The present study is a single-center retrospective cohort study.
Objective:
The objective of the study is to verify the hypothesis that sharp elevation of systolic blood pressure at extubation is a risk factor for development of symptomatic epidural hematoma after spinal surgery.
Summary of background data:
Postoperative symptomatic epidural hematoma (she) after spine surgery is a rare but potentially serious complication that may result in paralysis unless removed at an early stage.
Methods:
The subjects were 2611 patients treated with decompression and decompression/fusion of the cervical, thoracic, and lumbar vertebrae at our hospital. Twelve of these patients developed postoperative SEH and removal of hematoma was performed. To investigate the risk factors in these patients, data were analyzed for age at the time of surgery, sex, preoperative complications, medical history, body mass index, preoperative platelet count, surgical procedure, microscope use, operative time, blood loss, surgical site, systolic blood pressure (SBP) at extubation, difference between resting and extubation SBP, ratio of SBP at extubation to that at rest, blood pressure at discharge from the operating room, and use of a drain.
Results:
There was a significantly higher rate of SBP ratio (extubation/rest) ≥1.3 in patients with SEH (p = 0.021, Fisher’s exact test). Among the preoperative complications and medical histories, the frequency of cerebrovascular disorder tended to be higher in SEH cases than in non-SEH cases (p = 0.073). There was no significant difference for all other parameters listed above. In multivariate logistic analysis, the odds ratios were 3.98 (p = 0.018) for an SBP ratio (extubation/rest) ≥1.3 and 4.75 (p = 0.055) for cerebrovascular disorder, suggesting effects of these two items. With simultaneous input into a multivariate model, SBP ratio ≥1.3 had a significant independent association with postoperative SEH (p = 0.021) and cerebrovascular disorder showed a tendency for this association (p = 0.072).
Conclusion:
The risk for symptomatic epidural hematoma is significant in patients with SBP at extubation that is more than 1.3 times that of SBP at rest.
Introduction
The incidence of postoperative symptomatic epidural hematoma (SEH) is low, but diagnosis and treatment at an early stage are important, and a delay in treatment may lead to a sequela of serious paralysis. Including asymptomatic cases, postoperative SEH is found at a rate of 67.6–100% on imaging. 1,2 In contrast, in 2013, the Japanese Society for Spine Surgery and Related Research (JSSSRR) reported a rate of 0.9% for SEH after spine surgery. 3 Not all cases of postoperative asymptomatic and symptomatic hematomas detected on imaging require surgery, and only 0.1–0.4% undergo reoperation. 4 –7 However, appropriate perioperative management and careful follow-up are required based on the possibility of development of SEH. Involvement of various factors in development of epidural hematoma has been reported, and blood pressure has occasionally been proposed as a risk factor. 8 –11
Our observations suggest that sharp elevation of systolic blood pressure (SBP) at extubation may be a risk factor for hematoma. Therefore, the objective of this study was to verify the hypothesis that sharp elevation of SBP is a risk factor for development of symptomatic epidural hematoma after spinal surgery in patients who underwent spinal surgery at our hospital in the last 17 years.
Subjects and methods
A single-center retrospective cohort study was performed in 2611 patients treated with decompression and decompression/fusion for cervical, thoracic, and lumbar vertebrae from May 2000 to March 2017 at our hospital. Postoperative SEH developed in 12 of these patients and removal of hematoma was performed. Patients with trauma, spinal injury, infection, and insufficient withdrawal of antithrombotic drugs were excluded. The indication for removal of hematoma was lower limb pain at rest with difficulty in self-control, and muscle weakness of MMT ≤3 that did not improve with time. The 12 patients (8 males and 4 females) had a mean age of 70.2 years (range 54–82 years), and preoperative diagnoses of lumbar spinal canal stenosis (n = 6), degenerative spondylolisthesis (n = 2), and cervical disc herniation, lumbar disc herniation, lumbar nonunion after vertebral fracture, and destructive spondyloarthropathy (n = 1 each). The surgical procedure was anterior cervical fusion in one case, lumbar decompression in four cases, lumbar decompression/fusion in six cases, and endoscopic discectomy in one case. The mean body mass index (BMI) was 23.5 kg/m2 (range 19.2–27.9 kg/m2). Hypertension, diabetes, cerebrovascular disease, and coronary artery disease (overlapping) were present as preoperative complications or medical history in 6, 1, 2, and 1 patients, respectively.
To investigate risk factors in patients who developed SEH after surgery, the following items were evaluated: age at time of surgery (≥70 vs. <70), sex, preoperative complications/medical history (hypertension, diabetes, cerebrovascular disorder, coronary artery disease), BMI (≥25 vs. <25 kg/m2), preoperative platelet count (≥1.5 × 106 vs. <1.5 × 106), surgical procedure (decompression, decompression/fusion), use of a microscope (yes vs. no), operative time (≥180 vs. <180 min), blood loss (≥300 vs. <300 mL), surgical site (lumbar spine vs. all other sites), SBP at extubation (≥170 vs. <170 mmHg), SBP at extubation minus SBP at rest (≥50 vs. <50 mmHg), SBP ratio (extubation/rest) (≥1.3 vs. <1.3), SBP at discharge from the operating room (≥130 vs. <130 mmHg, diastolic blood pressure (DBP) ≥85 vs. <85 mmHg), and drain placement (yes vs. no).
The 12 patients who developed SEH were divided into those with a SBP ratio (extubation/rest) of ≥1.2, ≥1.3, and ≥1.4. Six patients each had a SBP ratio >1.3 and <1.3, showing that 1.3 was the median. Thus, a SBP ratio of ≥1.3 was used as a potential risk factor. For the SBP difference between extubation and rest, 50 mmHg was used as a potential risk factor for consistency with Yamada et al. 8 For operative time and blood loss, ≥180 min and ≥300 mL were defined as thresholds for a long surgery and high blood loss, respectively, and both were used as potential factors.
Fisher’s exact test and multivariate logistic analysis were used for statistical analysis, using STATA version 15 (STATA Corp., College Station, Texas, USA). The significance level was 5%. This study was performed after approval by the Ethics Committee of Toho University Omori Medical Center (#M18071).
Results
Twelve (0.46%) of the 2611 patients required urgent removal of SEH, which manifested as MMT3 or lower muscle weakness in 10 cases and lower limb pain at rest with difficulty in self-control in 2 cases. The onset time ranged from immediately after surgery to within 3 h in all, except in one of the patients, and reoperation was performed 4 h after onset on average. During reoperation, hematoma had expanded vertically at the surgical level in many cases and laminectomy was added. Hemostasis was performed using anticoagulants and oxycellulose hemostatic agents when the bleeding point was clearly observed. A suction drain was used in the first surgery in all patients, but the effect may have been insufficient. Therefore, two drains were placed in the second operation. Pain disappeared after reoperation in all patients and favorable recovery from muscle weakness was also acquired, except for one patient. There was a significant difference in the rate of SBP ratio (extubation/rest) ≥1.3 between the SEH and non-SEH groups (p = 0.021, Fisher’s exact test). Among preoperative complications/medical histories, cerebrovascular disorder (p = 0.073) tended to differ between these groups, but there were no significant differences in age at time of surgery, sex, hypertension, diabetes, or coronary artery disease as an underlying disease, BMI, preoperative platelet count, surgical procedure, use of a microscope, operative time, blood loss, surgical site, SBP at extubation, SBP difference, SBP at discharge from the operating room, and use of a drain (Table 1). In multivariate logistic analysis, factors associated with postoperative SEH were examined after the removal of confounders of age and sex. The odds ratios were 3.98 (p = 0.018) for an SBP ratio ≥1.3 and 4.75 (p = 0.055) for cerebrovascular disorder, suggesting effects of these two factors. In a model including both of these items, SBP ratio ≥1.3 was independently associated with SEH (p = 0.021), and cerebrovascular disorder showed a tendency for an association (p = 0.072) (Table 2). These results were similar after excluding age and sex.
Comparison of variables for patients with and without symptomatic epidural hematoma.
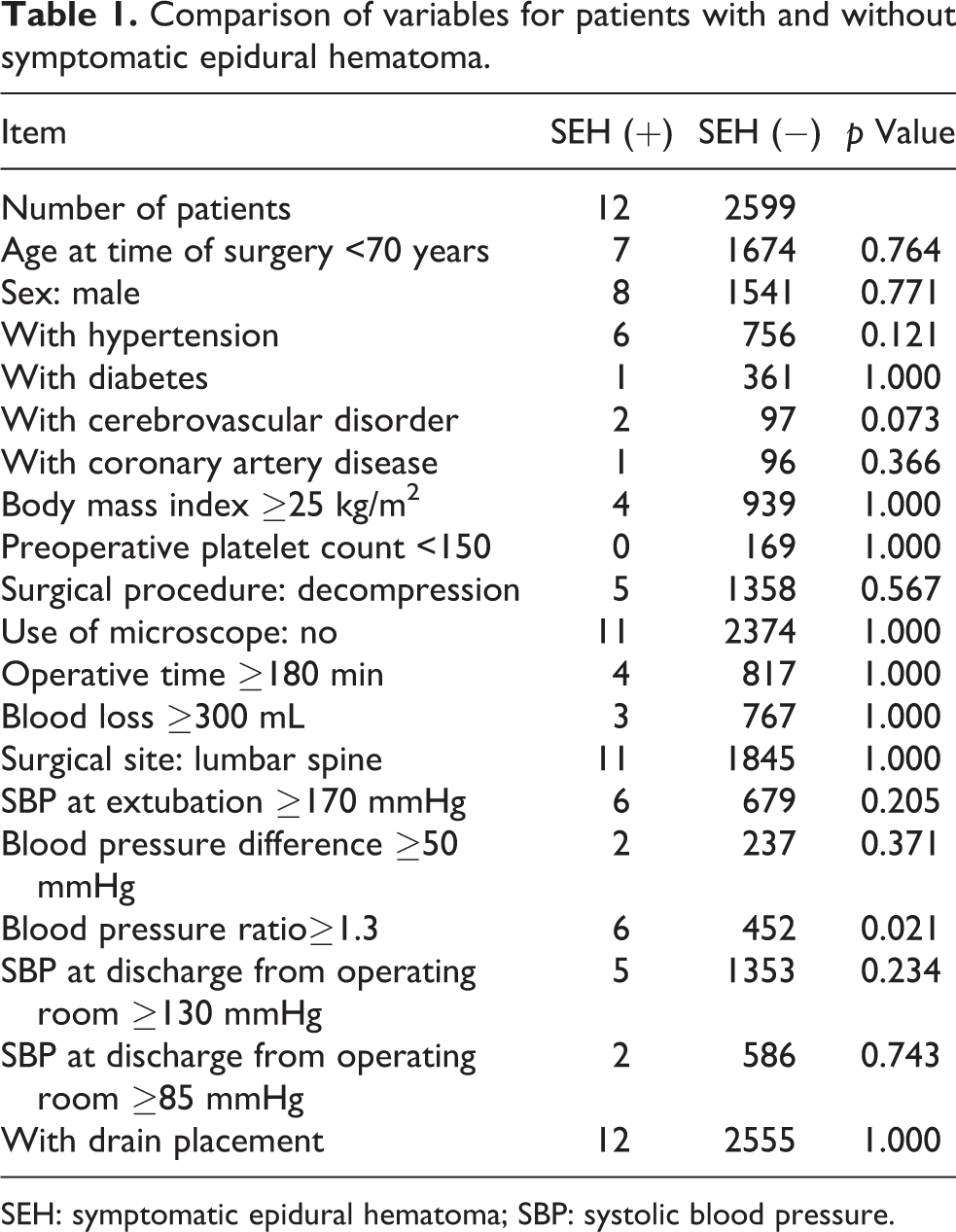
SEH: symptomatic epidural hematoma; SBP: systolic blood pressure.
Results for analysis of potential risk factors for symptomatic epidural hematoma

SBP: systolic blood pressure.
Discussion
The JSSSRR reported an incidence of postoperative SEH of 0.9% (288 of 31,380), 3 while Aono et al. found a rate of 0.41% (26 of 6356 patients) for SEH requiring reoperation. 4 Therefore, although the incidence is very low, urgent removal of hematoma is often necessary, and a delay of surgery may result in permanent paralysis.
Several studies have investigated the incidence of postoperative epidural hematoma on imaging. Kobayashi et al. reported that postoperative asymptomatic epidural hematoma was formed in all patients on MRI within 24 h after surgery. 1 Nakagawa et al. found rates of intra- and extraspinal canal epidural hematomas of 67.6% and 91.1%, respectively, on MRI performed 2 days after surgery, with a mean area of epidural hematoma occupying the spinal canal of 22.1% and a cutoff value of this area of 41.5% for the risk of SEH. 2 Kou et al. suggested that development of postoperative SEH is not due to a single factor alone and that many factors are involved, such as multilevel spinal surgery and preoperative antithrombotic therapy. 6 Awad et al. reported that these factors include age ≥60 years, preoperative use of nonsteroidal anti-inflammatory drugs (NSAIDs), Rh-positive blood type, surgery on five or more intervertebral segments, preoperative hemoglobin <10 g/dL, intraoperative blood loss >1 L, and prothrombin time–international normalized ratio >2.0 within 48 h after surgery. 5
Blood pressure as a risk factor for postoperative SEH has occasionally been suggested in previous reports. Tokioka et al. found that 83.3% of cases were in a hypertensive state with postoperative SBP ≥160 mmHg, 9 and development of clinically problematic hematoma can be prevented by thorough management of blood pressure by continuous intravenous injection of nicardipine hydrochloride. 10 Kao et al. focused on DBP and drainage volume in patients with an incidence of postoperative SEH of 0.16% (25 of 15,562). The mean preoperative DBP was significantly higher in SEH cases compared to asymptomatic cases (81.16 vs. 70.96 mmHg), and the postoperative drainage volume was significantly smaller in SEH cases (465.44 vs. 900.32 mL). 11 Yamada et al. suggested SBP elevation by ≥50 mmHg at extubation and high BMI as risk factors and found that hematoma was reduced on imaging in patients in whom a drain was placed. 8
In our institution, SBP is controlled at ≤100 mmHg to reduce intraoperative blood loss, but sharp blood pressure elevation is often noted at extubation. Since we had the impression that the incidence of SEH is high in these patients, we investigated SEH with a focus on changes in SBP, and especially preoperative SBP at rest and blood pressure elevation at extubation. The SBP ratio (extubation/rest) was examined as a risk factor for SEH and subjected to statistical analysis using cutoffs starting from a ratio ≥1.2, and a significant difference was found at a ratio of ≥1.3. Multivariate analysis was then performed with the following potential risk factors for development of SHE selected from past reports: age at time of surgery, sex, concomitant diseases, such as hypertension, diabetes, coronary artery disease, and cerebrovascular disorder, BMI, preoperative platelet count, surgical procedure, presence or absence of use of a microscope, operative time, blood loss, surgical region, SBP at extubation, blood pressure difference, SBP and DBP at discharge from the operating room, and placement of a drain. In this analysis, a SBP ratio (extubation/rest) ≥1.3 emerged as a significant factor. This may not be the only important factor for development of SEH and multiple factors may be involved, as mentioned in previous studies, but the odds ratio was about 3.9, suggesting that the SBP ratio (extubation/rest) is a strong risk factor. We also performed a study replicating reported cases, but no significant difference was noted in any case with SBP elevation at extubation ≥50 mmHg, SBP at extubation ≥170 mmHg, or DBP ≥85 mmHg at discharge from the operating room. We also found no difference due to the surgical region, in contrast to the finding of Aono et al. that the incidence of SEH was significantly higher after surgery on the thoracic vertebral region. 4
As countermeasures against postoperative SEH, we control the intraoperative blood pressure at ≤100 mmHg as much possible, very carefully confirm hemostasis, and place a drain before closing the wound. However, sharp blood pressure elevation at extubation may cause hemorrhage in the wound and hematoma formation. Moreover, hematoma tended to develop in the presence of cerebrovascular disorder as an underlying disease, and the rate of patients with this disease taking oral antiplatelet agents may be high. In our hospital, antiplatelet agents are withdrawn before surgery in all patients, but our findings suggest that this may have been a factor associated with postoperative wound hemorrhage. High-risk patients are managed by control of pre- and postoperative blood pressure as much as possible, with a return to the average blood pressure and careful application of hemostasis before extubation, placement of a drain after surgery, and consideration of extension of the period of drain placement based on the drainage volume.
The limitations of this study include data collection from a single institution and positive cases accounting for only 0.46% of all cases. Moreover, the frequency of asymptomatic epidural hematoma was unclear because imaging was not performed in cases other than those with suspected postoperative SEH. Furthermore, in patients using antithrombotic drugs, surgery was performed after withdrawal of the drugs, following the ‘Guidelines for management of anticoagulant and antiplatelet therapy in cardiovascular disease’. 12 Since patients with an insufficient washout period were excluded, we consider that there was no influence of antithrombotic drugs, but no comparison between users and nonusers was performed.
Conclusion
Of the 2611 patients who underwent spine surgery at our hospital, 12 required reoperation for postoperative symptomatic epidural hematoma. A ratio of preoperative resting blood pressure to blood pressure at extubation of 1.3 or higher is a risk factor for postoperative symptomatic epidural hematoma, and this ratio may serve as a simple index for development of this condition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.