
Abstract
Background:
Lateral femoral bowing causes a higher tensile mechanical load on the lateral side of the femur, which plays a critical role in the pathogenesis of atypical femoral fractures (AFFs). There are many ways to measure lateral femoral bowing on plain radiographs, and there are difficulties in finding a correspondence point between measurements among multiple measurers. The purpose of this study is to prove the best method of correspondence between the investigators by analyzing the reliability of various methods for measuring lateral femoral bowing.
Materials and Methods:
We retrospectively collected data from 85 patients (87 femurs) diagnosed with AFF who had plain radiographs of entire femur from October 2013 to March 2018. The femoral bowing was measured in coronal view of femur plain radiographs using five methods (Sasaki, Morin, Jang, Kim, and Yau) by three examiners, respectively. The intra- and interobserver reliability of each method was assessed using intraclass correlation coefficient (ICC) for continuous variables.
Results:
All methods showed excellent intra- and interobserver reliability with ICC of >0.8. Among five methods, the Yau’s method was the highest reliable method (ICC = 0.980, 95% confidence interval = 0.971–0.986).
Conclusions:
All methods of measuring lateral femoral bowing in the coronal plane of plain radiographs are reliable. And, we recommend Yau’s method, which has a clear reference point for measuring femoral bowing and is highest reproducible.
Introduction
According to previous large database studies, the incidence of atypical femoral fractures (AFFs) is estimated to be 1.8–50 per 100,000 persons years. 1 –3 Despite the low incidence of AFFs, there is a considerable concern for AFFs as the aging society and increasing number of osteoporosis patients. Studies on femoral geometry as a risk factor for AFFs have been actively conducted recently. 4 –6 Anterolateral femoral bowing causes a higher tensile mechanical load on the lateral side of the femur, which plays a critical role in the pathogenesis of AFF. 7 In addition, there have been recent reports comparing the location of AFFs according to the degree of femoral bowing. 8
Predicting the risk of AFFs and managing for fracture prevention has recently become an important issue, 9 so it is important to make reliable measurements of anterolateral femoral bowing, an important risk factor for AFFs. There are many ways to measure lateral femoral bowing on plain radiographs, and there are difficulties in finding a correspondence point between measurements among multiple measurers. 7,10 –14 For the accurate description and communication between the measurers, the measurement method should have high reliability and high agreement between the observers. However, there was no study to evaluate the reliability and agreement between measurements of lateral femoral bowing.
The purpose of this study is to determine the best method of correspondence between the investigators by analyzing the reliability of various methods for measuring lateral femoral bowing.
Materials and methods
To evaluate the reliability of measurement of anterolateral bowing of femur, we identified 118 patients who were treated for AFF at our hospital from October 2013 to March 2018.
The inclusion criteria were (1) patients who had radiographs before complete and (2) the availabilities of anteroposterior (AP) view of entire femur. We excluded 33 patients who did not have radiographs of the entire femur before complete fracture. Finally, we included 85 patients in this study. The mean age was 73.0 years (standard deviation, 8.5; range, 45.6–88.4 years). There were 2 men and 83 women. Two of them were treated with bilateral AFFs and the final 87 femurs with AP view of entire femur before complete fracture were included.
All radiographs were taken in the same radiology unit using a standardized protocol. AP radiographs of femur were obtained in supine position at a source to film distance of 110 cm. Hips were kept in extension, and knees were kept in extension and neutral rotation with patella facing anteriorly. In all cases, X-ray beam was centered on the middle of the thigh and the X-ray beam was perpendicular to the patients. All radiographic images were digitally acquired using a picture archiving and communication system (PACS; Impax: Agfa. Antwerp, Belgium), and all measurements on radiographs were subsequently carried out on 19-inch LCD monitor using PACS software.
Three observers who were orthopedic surgeons with 5 (HK), 4 (BS), and 4 (HJ) years of experience and were familiar with radiographs of femur. Consensus building sessions for each method were held before measuring lateral bowing of femur by three orthopedic surgeons and two senior surgeons (YK and KH).
Methods for measurement of lateral bowing of the femur on radiograph
Sasaki’s method
Two lines along the proximal and distal portions of the femoral shaft were drawn on AP X-rays. Lateral femoral shaft bowing angle is defined as the angle between the two lines on the AP view 13 (Figure 1(a)).
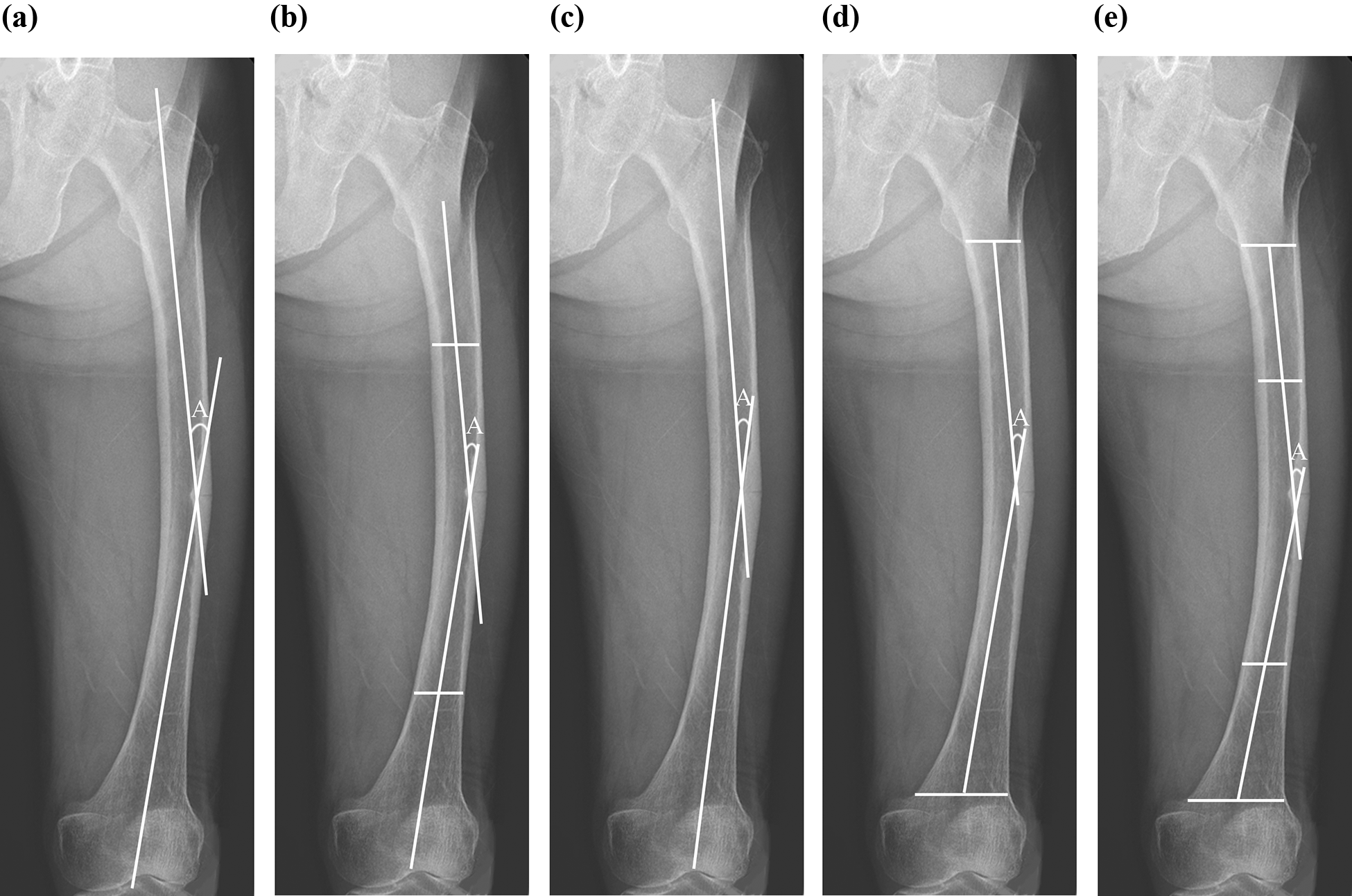
Assessment methods for measuring lateral femoral bowing on plain radiography. (a) Sasaki’s method, (b) Morin’s method, (c) Jang’s method, (d) Kim’s method, and (e) Yau’s method. (A = angle of lateral femoral bowing.).
Morin’s method
Lateral bowing is the angle between axes of 20% proximal and distal sections of femur diaphysis on AP view 7 (Figure 1(b)).
Jang’s method
Femoral bows were defined as the angle formed by two lines which are parallel to the proximal and distal portions of femoral shaft. At this point, the proximal line goes through greater trochanter tip and the distal line through intercondylar notch 10 (Figure 1(c)).
Kim’s method
Lateral bowing was measured as the angle formed at the bisection of the two lines drawn through the long axis of the proximal and distal parts of the femur. 11 Each line was drawn from the midpoint of the endosteal canal at the level of lesser trochanter for the proximal part and supracondylar ridge for the distal part (Figure 1(d)).
Yau’s method
To measure lateral femoral bowing, the diaphysis of the femur was divided into four equal parts and a line was then drawn in each quarter to highlight the midpoint of the endosteal canal. The degree of lateral femoral bowing was defined as the angle formed between the central line of proximal femoral diaphysis and the central line of distal femoral diaphysis 14 (Figure 1(e)).
Assessment of reliability of measuring lateral bowing of femur
Reliability is defined as consistency of measured values. The femoral bowing was measured in AP view of femur plain radiographs using six methods (Sasaki, Morin, Jang, Kim, Yau, and Park) by three examiners (HK, BS, and HJ), respectively.
Each observer was blinded to other measurements and patients’ data. Orders of measurements were assigned randomly to each observer and all data were collected by a research assistant who did not participate in the reliability sessions. The intraobserver reliability of each method was assessed using the values measured by one examiner, who performed the reassessment 3 weeks later. 15 The interobserver reliability of each radiographic measurement was evaluated with an intraclass correlation coefficient (ICC).
Statistical analysis
The ICC with 95% confidence interval (CI) was used to analyze interobserver reliability of the obtained continuous data among the three observers. The intra- and interobserver reliability was evaluated using the two-way random effects model assuming a single measurement and absolute agreement. And ICC of 1 means perfect reliability and 0 means the opposite. Values of ICC were characterized as poor (<0.20), fair (0.21–0.40), moderate (0.41–0.60), good (0.61–0.80), or excellent (0.81–1.00). 16 Statistical analyses were performed using SPSS version 25.0 (SPSS Inc., Chicago, Illinois, USA).
This study was approved by the institutional review board at our hospital, who waived informed consent.
Results
In five radiological measurements which consisted of continuous data, the intra- and interobserver reliabilities were >0.80. Among five methods, the Yau’s method showed highest intra- and interobserver reliability (Table 1). And, Kim’s method tend to underestimate the lateral bowing angle of femur (Table 2).
Intra- and interobserver reliability of femoral bowing measurements on radiography.
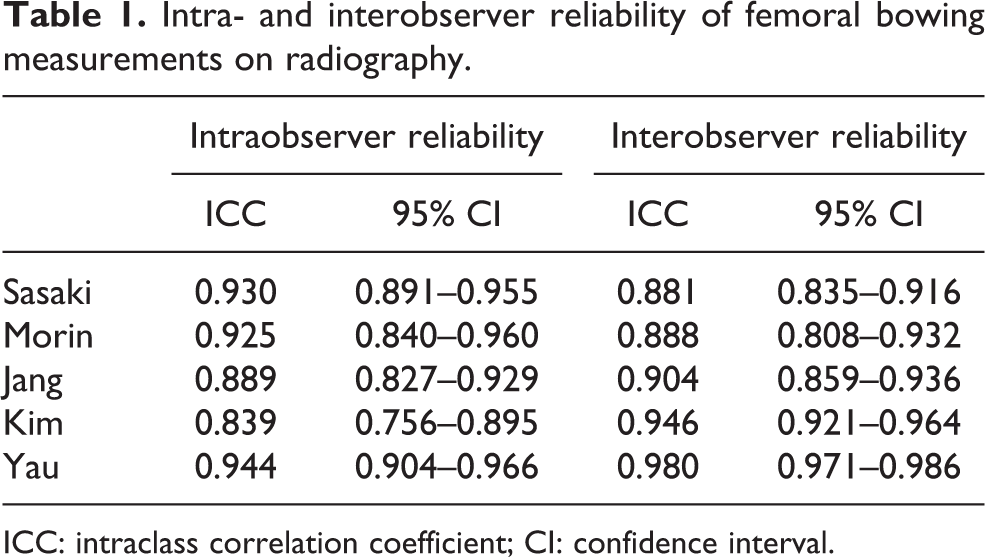
ICC: intraclass correlation coefficient; CI: confidence interval.
Measurement of each observer according to each method.

Discussion
The femoral shaft receives compressive and bending forces when loading is applied. At this time, buckling occurs in long bones with thin cortex. 17 And buckling of the femoral shaft can proceed to femoral shaft bowing, which is the result of bone remodeling from the bending force. Excess lateral bowing of femur shaft can cause low energy fractures such as AFFs by increasing tensile stress on the lateral femoral cortex. 18 Sasaki et al. 13 reported that femoral curvature in low energy femoral shaft fractures group is statistically significantly greater than in the age- and gender-matched control group. And other studies have shown that anterolateral femoral bowing is most strongly associated with the occurrence of AFFs compared with other factors such as suppression of bone turnover. 7,10
Various methods have been developed to measure lateral femoral bowing, using radiographs, 2D–3D X-ray scanner (EOS™), or CT scans. 7,13,19 Because femoral bowing seen in plain radiography may be affected by the patient’s position or femoral torsion, femoral bowing on reconstructed CT is more accurate than plain radiographs. 19 However, because of the high amount of radiation and the high cost of CT, plain radiographs are often used. The fact that there are many ways to measure femoral bowing on plain radiographs suggests that one ideal measurement was not revealed.
A good measurement method should have high reliability for proper communication between measurers. Reliability in statistics is the overall consistency of a measure and has to do with the quality of measurement. A measure that are highly reliable are accurate, reproducible, and consistent from one testing occasion to another. In its everyday sense, reliability is the “consistency” or “repeatability” of one’s measures. 20
In this study, all five methods consisted of continuous data showed a result of ICC 0.80 or higher. And these methods can be considered as a method of high agreement between measurers. The method with the lowest ICC was Sasaki’s method with ICC 0.881 (95% CI 0.835–0.916), and ICC was the highest in Yau’s method with ICC 0.980 (95% CI 0.971–0.986). The reason for the relatively low interobserver reliability in Sasaki’s method is that the reference points on the proximal and distal parts are ambiguous. On the other hand, the reason for the higher reliability in the Yau’s method is that the reference point for measuring the bowing is relatively accurately specified as the midpoint of the medullary canal in the proximal and distal quadrant. In addition, in the Morin’s method, the midpoint of the endosteal canal at 20% of the femoral shaft was specified as the reference point and showed good reliability with ICC 0.888 (95% CI = 0.808–0.932).
Recently, Park et al. presented their own classification. In their method, the reference line is drawn from the tip of the greater trochanter to the center of the intercondylar notch on AP radiograph. Grade A (nearly straight) indicates that the reference line is located in the middle one-third of the medullary canal at the apex of the curve. Grade B (mild) describes a reference line located in the medial one-third of the medullary canal. Grade C (moderate) refers to a reference line that begins outside of the medullary canal medially and passes through the medial cortex. Grade D (severe) describes a reference line that runs medial to the medial cortex. 12 We did not include the Park’s method, because their classification was categorical variables, unlike the included methods with continuous variables.
There were some limitations in this study. First, the validity value was not obtained because there was no gold standard for lateral bowing of femur. Second, considering the small differences of ICC between the five methods, positioning of the patients during obtaining radiographs might be more significant in measurement of lateral bowing of femur.
Despite these limitations, this is the first study on the reliability of lateral femoral bowing measurement. Among the methods of measuring lateral femoral bowing in the coronal plane of plain radiographs, five methods of continuous value (Sasaki, Morin, Jang, Kim, and Yau) are reliable. And, we recommend Yau’s method, which has a clear reference point for measuring femoral bowing and showed highest reliability.
Footnotes
Acknowledgement
We appreciated that HK, BS, and HJ measured the parameters for this study.
Authors’ contribution
Y-KL and JY contributed equally to this work as co-first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.