
Abstract
Purpose:
This study aimed to determine the prevalence of incomplete atypical femoral fractures (iAFFs) in postmenopausal women using bisphosphonates and to investigate the potential risk factors for the development of iAFF.
Methods:
The national health-care records system indicated that 2746 postmenopausal women in our region aged ≥50 years were taking bisphosphonates. Using an assumed iAFF prevalence of 10% and levels of 5% α significance and ±5% precision, we calculated that a sample size of 132 participants was needed for this study. The patients were randomly selected and invited to the hospital. Radiographs and bone scans were used to evaluate each patient for iAFF. Bone mineral density, 25-hydroxy vitamin D, parathyroid hormone, and alkaline phosphatase measurements were performed.
Results:
The mean age of the study population was 72.79 ± 7.35 years, and the mean duration of bisphosphonate use was 7.7 ± 3.4 years. We found iAFF in 14 (10.6%) patients, and 3 patients had bilateral involvement. Of the 17 femurs with iAFF, a proximal third location was seen in 2 patients (11.8%), a mid-third location in 14 (82.4%), and a distal third location in 1 (5.9%). The duration of bisphosphonate use was longer, and parathyroid hormone levels were higher in patients with iAFF compared to those without an incomplete fracture.
Conclusion:
We found a relatively higher prevalence of iAFF in postmenopausal women using bisphosphonate. Early identification and treatment of iAFF is crucial for reducing potential patient morbidity and hospital costs.
Introduction
Osteoporosis is a common disease in the elderly population. The increased risk of bone fractures causes significant morbidity and mortality in patients and poses an economic burden for health-care systems. 1 –3 Bisphosphonates are the most commonly used antiresorptive agents for the first stage of osteoporosis treatment. 4,5 Bisphosphonates are potent inhibitors of osteoclast-mediated bone resorption. The efficacy of these drugs in reducing the risk of osteoporotic fracture has been demonstrated in extensive clinical studies, and they have generally been found to be safe. 6 However, particularly after the mid-2000s, an increasing number of atypical subtrochanteric and femoral diaphysis fractures began to be reported. It is thought that these fractures could be related to the long-term use of bisphosphonates. 7 –11
The American Society of Bone and Mineral Research (ASBMR) working group has defined complete atypical femoral fractures (AFFs) as noncomminuted, transverse, or short oblique subtrochanteric or femoral shaft fractures that extend across the entire femoral shaft, often with the formation of a medial spike. 12 Incomplete atypical femoral fractures (iAFFs) may also be encountered in the form of a stress fracture or a periosteal or endosteal thickening in the lateral cortex. AFF incidence has been reported in numerous studies at low rates of 1/100,000–5/10,000, and an increase in AFF incidence has been shown to correlate with the duration of bisphosphonate treatment. 13,14
To the best of our knowledge, there are many studies about incidence or prevelance of AFF, but there are no previous reports in the literature of a randomized study related to the prevalence of iAFF in postmenopausal, osteoporotic women. This study aimed to determine the prevalence of iAFF in postmenopausal women using bisphosphonates and to investigate the potential risk factors for the development of iAFFs.
Materials and methods
Study population
Approval for the study was granted by the Clinical Research Ethics Committee of Mugla Sitki Kocman University (decision no: 11/VII, dated: June 17, 2016). Informed consent was obtained from all individual participants included in this study. The inclusion criteria were defined as: age >50 years, female gender, a diagnosis of osteoporosis, and the use of bisphosphonates. Patients were excluded from the study if they had a history of fracture or previous surgical intervention to a lower extremity, a history of trauma in the previous 6 months, a malignancy, or any metabolic bone disease other than osteoporosis.
This study was conducted in Mentese district, province of Mugla, Turkey, where a population of approximately 110,000 people lives. The national health-care records system indicated that aged ≥50 years 2746 postmenopausal women in this region were using bisphosphonates. The sample size of 132 participants was estimated using the Epi Info™ version 7.2.2.2 software (Centers for Disease Control and Prevention, Atlanta, Georgia, USA). As the actual prevalence of iAFF in bisphosphonate using osteoporotic cohort is unknown, we assumed an iAFF prevalence of 10%, and α level of 5% significance with ±5% precision was used. Patients were randomly selected and invited to the hospital until desired number of patients was reached. Of these, 21 women chose not to participate, and 9 women were excluded based on the exclusion criteria (4 based on previous surgeries, 3 due to a history of trauma, 1 with a malignancy, and 1 with osteitis fibrosa cystica). The flowchart of the study is shown in Figure 1.

Flowchart of the study.
Imaging studies
To confirm iAFF diagnosis and to avoid missing any early insufficiency fractures, antero-posterior and lateral radiographs together with a whole-body bone scintigraphy (Symbia E Dual-Head Gamma Camera, Siemens™, Illinois, USA, 2011) were taken in all recruited subjects. The images were evaluated by a team comprising two orthopedic surgeons, a radiologist and a nuclear medicine specialist (each of whom had 8–22 years of experience), and a consensus diagnosis was reached. The presence of increased isotope uptake on the lateral cortex of femur with bone scintigraphy was accepted as the mainstay of iAFF diagnosis, along with a wide range of radiographic features. 15,16 The sites of involvement were separated into three groups: proximal, mid, or distal femoral diaphysis.
Scoring
Scoring system recommended by Min et al. was used to calculate the risk for impending complete fracture among iAFFs. 17 According to this weighted scoring system, four identified risk factors: the site (subtrochanteric: three points, diaphyseal: two points, others: one point), severity of pain (functional: three points, mild: two points, none: one point), status of contralateral femur (intact: three points, iAFF: two points, complete AFF: one point), and the ratio of the extent of radiolucent line to the femoral diaphsis diameter (>1/2: three points, <1/2: two points, focal change: one point) were evaluated.
Laboratory tests
The following measurements were taken for all patients: bone mineral density (BMD), 25-hydroxy vitamin D, parathyroid hormone (PTH), and alkaline phosphatase (ALP). The BMD measurements of femoral neck and anteroposterior lumbar spine were performed using a dual-energy X-ray absorptiometry (DXA) machine (Stratos DR 2D Fan Beam DEXA, DMS™, Perols, France, 2009). In accordance with the World Health Organization (WHO) criteria, normal BMD was defined as a value less than one standard deviation (SD) below the young adult peak BMD (T-score), osteopenia was defined as a value ranging from 1.0 to 2.5 SD below the young adult peak BMD, and osteoporosis was defined as a value equal to or greater than 2.5 SD below that of the young adult peak BMD. 18
Clinical information such as age, height (cm), weight (kg), and duration of bisphosphonate treatment was recorded for all patients. In addition, patients were asked whether they had been diagnosed with diabetes mellitus (DM) and whether they had been prescribed steroids or proton pump inhibitors (PPIs).
Statistical analysis
The data obtained in the study were analyzed using IBM SPSS Statistics™, version 22 software (IBM Corp.™, Armonk, New York, USA). The independent samples Student’s t-test and the χ2 test were used to compare patients with and without evidence of iAFF in terms of each numeric imaging and laboratory study end point. Age was stratified into three categories (50–64, 65–74, and ≥75 years), and duration of bisphosphonate use was divided into three categories (1–4, 5–9, and ≥10 years). Age-adjusted odds ratios with 95% confidence intervals (CI) were calculated by logistic regression for the relative risk of incomplete atypical fracture with bisphosphonate use. All reported p values are two-sided and have been corrected for age. A value of p < 0.05 was accepted as statistically significant.
Results
The mean age of the study patients was 72.79 ± 7.35 years, and the mean duration of bisphosphonate use was 7.74 ± 3.43 years. The mean body mass index (BMI) was 28.71 ± 5.14 kg/m2. For the whole study group, the mean femoral neck T-score was−1.78 ± 0.78, and the lumbar T-score was −2.49 ± 1.13. The presence of iAFF was detected in 14 (10.6%) patients. The demographic and laboratory data of the groups with and without iAFF are presented in Table 1.
Demographic and clinic characteristics distributed in the overall sample and according to the presence of incomplete atypical femoral fracture.a

iAFF: patients with incomplete atypical femoral fracture; non-iAFF: patients without incomplete atypical femoral fracture; BP: bisphosphonate; DXA: dual-energy X-ray absorptiometry; PPI: proton pump inhibitor.
a Variables are expressed as numbers and percentages or mean ± standard deviation. Percentages are calculated on the entire size of each row. Continuous variables were inspected using t-test and analysis of variance when testing differences among more than two groups. Age-adjusted statistical significance is also displayed in the last column (p*).
In the 14 patients with iAFF, right-side involvement was found in 4 (28.6%), left-side involvement in 7 (50%), and bilateral in 3 (21.4%). Of the 17 femurs with iAFF, a proximal third location was seen in 2 (11.8%), a mid-third location in 14 (82.4%), and distal third location in 1 (5.9%). Dreaded black line was observed in 2 (11.8%), focal periosteal or endosteal thickening of the lateral cortex was seen in 12 (70.5%; Figure 2), and vague striations was present in 3 (17.7%; Figure 3) of 17 femurs. 15,16 None of the iAFF-detected patients had specific functional or acute-onset pain. Some of these patients had nonspecific knee and hip pain that cannot be distinguished from osteoarthritis. The characteristics of the femurs with iAFF are presented in Table 2.
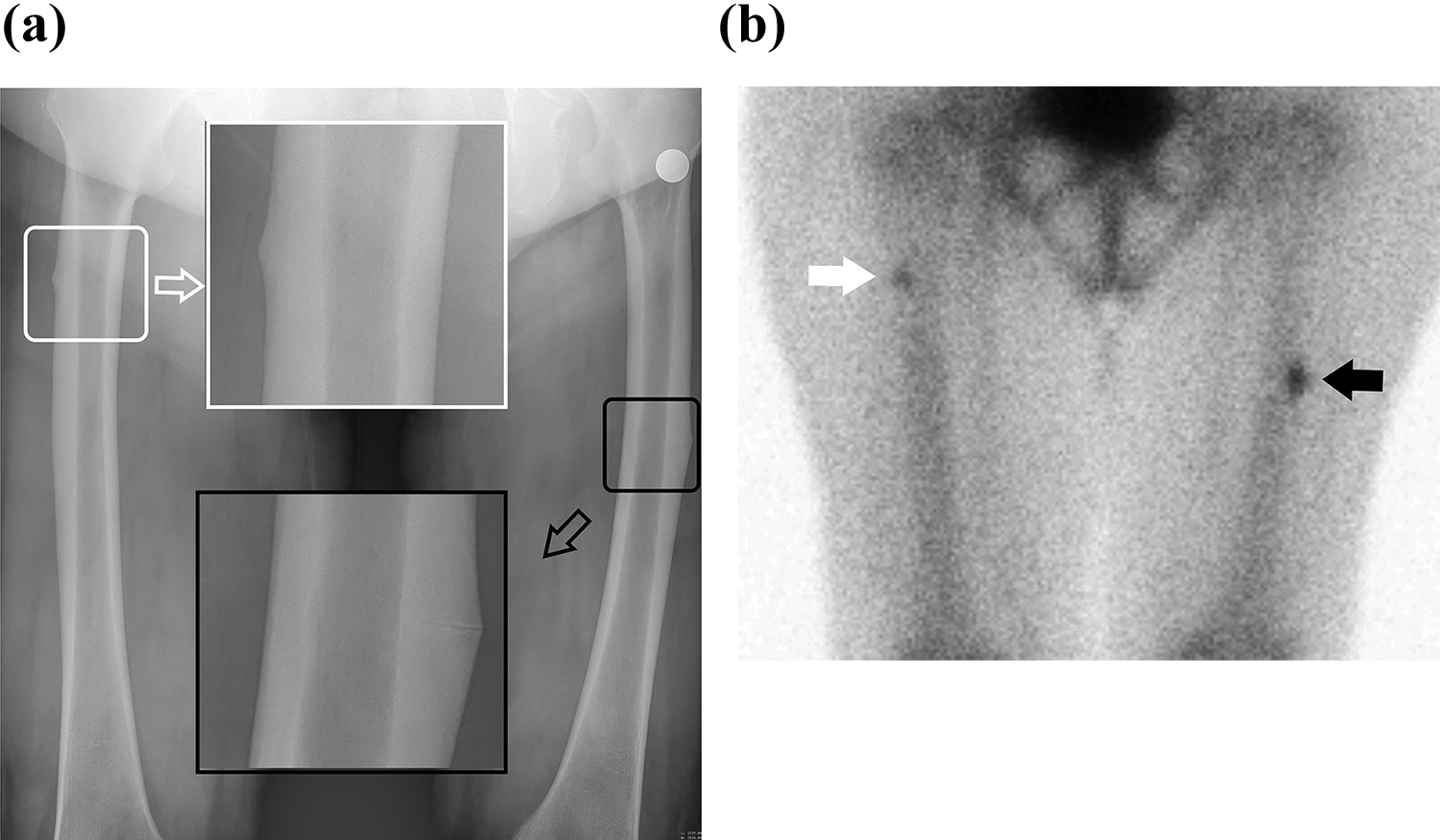
(a) Plain radiograph of a patient aged 82 years with bilateral incomplete atypical femoral fractures. A lucent line at the mid-diaphysis of left femur (black arrow shows enlargement of black box) and cortical thickening at the proximal third of right femur (white arrow shows enlargement of white box) are seen. (b) Increased uptake is seen at right proximal femur (white arrow) and left mid diaphyseal femur (black arrow) with bone scintigraphy of the same patient.
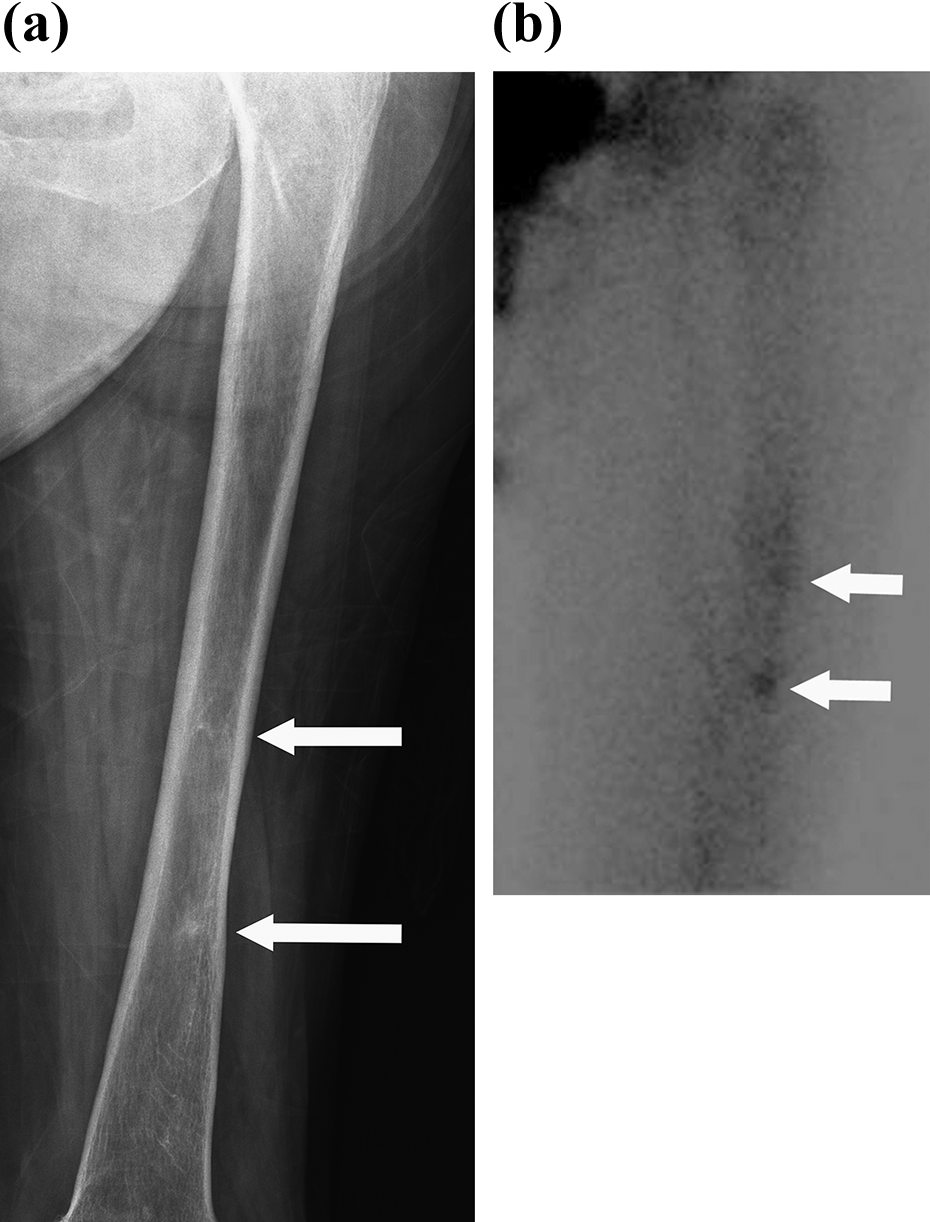
(a) Plain radiograph of a 78-year-old patient shows only vague striations (white arrows) at the left femur. (b) Bone scintigraphy shows increased uptake (white arrows) on the lateral cortex of the left femur.
Characteristics of femurs with incomplete atypical femoral fractures.a

BP: bisphosphonate; PPI: proton pump inhibitor; PTH: parathyroid hormone; ALP: alkaline phosphatase; DM: diabetes mellitus.
a Variables are expressed as numbers. Steroid and proton pump inhibitor treatment history and patients diagnosed with diabetes mellitus are shown with (+) or (−) as its presence.
b Patients with bilateral incomplete atypical femoral fractures.
According to the statistical analyses, no significant differences were identified between the groups in terms of age, height, weight, BMI, femoral neck and lumbar T-scores, 25-hydroxy vitamin D levels, and ALP levels. No correlation was found between iAFF and DM or the use of steroids or PPIs. In the patients with iAFF, the duration of bisphosphonate use was longer, and the PTH levels were higher compared to those without iAFF. The age-adjusted relative risk of having an incomplete atypical fracture was found three times higher after 5 years of bisphosphonate usage (odds ratio: 3.003, 95% CI: 0.644–13.997) and about 10 times higher after 10 years of bisphosphonate usage (odds ratio: 9.644, 95% CI: 3.286–28.303). The comparative distribution of bisphosphonate therapy duration according to age groups is shown in Figure 4.

The box plot graphic shows the comparative distribution of bisphosphonate therapy duration according to age groups.
Discussion
Osteoporosis is the most important risk factor for hip and spinal fractures in postmenopausal women, and bisphosphonates are currently the most commonly used treatment. Data from randomized trials as well as clinical experience indicate that bisphosphonates are generally safe; however, in recent years, an increasing number of studies have suggested a relationship between AFF and long-term bisphosphonate use. 19 Although the mechanism of fracture formation has not been proved, it is thought that by inhibiting osteoclast-mediated bone resorption, long-term bisphosphonate use slows bone turnover, resulting in the accumulation of microdamage that cannot be repaired. 20
ASBMR formed a working group related to femoral fractures and, in 2010, defined the major and minor characteristics of these fractures. 21 In 2014, the diagnostic criteria were reviewed and published. 12 According to these criteria, the fractures can be classified as incomplete or complete. The iAFF characteristics are defined as only the lateral cortex involvement, generalized or localized cortical thickening in the femur diaphysis, the presence of unilateral or bilateral prodromal symptoms, and periosteal or endosteal thickening in the lateral cortex.
While the definition of complete fractures is more detailed, we believe that the definition of incomplete fractures is not excellent. Some patients with incomplete fractures are asymptomatic, and the definition of generalized cortical thickening is ambiguous. 15 Niimi et al. found no significant difference with respect to femoral cortical thickening between osteoporotic patients with long-term bisphosphonate use histories and those not receiving bisphosphonate treatment. 22 In addition, Koeppen et al. compared femoral cortical thickening in patients >55 years old with ordinary femoral fractures and those with AFFs, and they found no significant difference. 23 Direct radiographs may not be sufficient to identify early iAFF, so advanced imaging techniques such as magnetic resonance imaging (MRI) or bone scintigraphy are preferred. 24 Bone scintigraphy was used in this study as the sensitivity of this imaging technique is high. 12 Bone scintigraphy helped to locate the lesions for radiographic scrutiny. iAFF could be ruled out when there is generalized thickening of the lateral cortex but not a hot lesion on bone scan. While MRI also has a high sensitivity for iAFF, this method was not selected due to costs and patient comfort.
Several noteworthy studies have been conducted on the incidence of AFF. Schilcher et al. examined 12,777 femoral fractures in patients aged >55 years and found an AFF incidence of 5.5/10,000 in patients using bisphosphonates. 25 In a study by Meier et al., subtrochanteric and femoral fractures were examined in hospitalized patients aged >50 years, and an AFF incidence of 32/1,000,000 in patients using bisphosphonates was reported. 26 Black et al. reviewed three extensive randomized bisphosphonate treatment studies; in the secondary analysis, subtrochanteric/femur diaphysis fractures following bisphosphonate use were determined to be 0.8%. 27 Studies have also revealed that AFF incidence is related to the duration of bisphosphonate exposure. Dell et al. reported that 1.78/100,000 cases per year were seen in patients with less than 2 years of bisphosphonate use, and 113.1/100,000 cases per year were seen in patients after 8 years of bisphosphonate use. 13
Studies determining AFF incidence have generally used retrospective analyses of an extensive series of femoral fractures identified by International Classification of Diseases (ICD) diagnostic codes; alternatively, the studies have reviewed the records of patients hospitalized with femoral fractures. Both methods have biases. ICD diagnostic codes may include incorrect data, and hospital records may not be representative of the population.
Determining iAFF incidence is even more problematic. La Rocca et al. prospectively followed 100 asymptomatic patients who had been treated with bisphosphonates for more than 3 years. 28 iAFFs were found in three femurs of two patients. In another study, McKenna et al. reported an iAFF prevalence of 2.7% in patients who presented at the hospital and who had been treated with bisphosphonates for more than 5 years. 29 Ernat et al. also examined the fractures and radiographical changes in patients treated with bisphosphonates for more than 5 years; they reported an iAFF prevalence of 2.02%. 30 All these studies included patient groups who presented at the hospital for several reasons. However, some patients with iAFF are asymptomatic, while others may be symptomatic but chose not to seek hospital treatment.
In our country, health insurance for all citizens is provided by a single national social security institution, and all drugs are prescribed through an online network. Bisphosphonate treatment can be administered to patients younger than 75 years of age with DXA results when the WHO criteria are met; the drug can be administered to patients older than 75 years of age without DXA results. An examination of the social security institution’s data indicated that there were 2746 patients aged >50 years in our region who had been diagnosed with osteoporosis and who were using bisphosphonate. A representative sample of 132 patients was selected at random from this data set for inclusion in the study.
In this study, iAFFs were identified in 14 (10.6%) patients. This prevalence was higher than the rates found in other studies. This difference could be attributed to several factors, including regional and racial differences, the use of a highly sensitive imaging method, and the high number of patients in the current study who had been using bisphosphonates for 10 years or more. We think that awareness of medical practitioners in our country about drug holiday of bisphosphonates is low, judging the number of patients who have been using bisphosphonates for a long time without interruption. Although rates are unknown, some of the iAFF remain quiet, while some of them lead to a complete fracture. Previous reports about iAFF are studied with patients who attended to hospitals. We also believe that the presence of patients who do not have severe complaints to visit a hospital in our study may have caused the higher prevelance than the previous studies.
Although AFF is a rare complication in patients treated with bisphosphonates, as the length of treatment increases, so does the incidence of AFF. 13,21 The current study also found an increase in iAFF incidence with prolonged exposure to bisphosphonates as 3 times higher after 5 years of bisphosphonate usage and about 10 times higher after 10 years of bisphosphonate usage. After 3–5 years of treatment with a bisphosphonate, a reassessment is recomended on every patient to determine whether further treatment is warranted or whether to stop the bisphosphonate. 15 Although there is no high-level evidence about the efficacy of discontinuation of bisphosphonates on its adverse effects, a 2- to 3-year drug holiday is recomended after 5 years of oral bisphosphonate or 3 years of intravenous bisphosphonate treatment to reduce the risk of iAFF in women with low risk for osteoporotic fractures. 31 The cessation of biphosphanate treatment is not reasonable in women with high risk for osteoporotic fractures, as the benefits of these drugs in preventing quite common vertebral and hip fractures are more important than their rare harms. 32
In a review of 147 AFFs, Kim et al. found that 35.4% of the AFF were located in the subtrochanteric area and 64.6% in the femoral diaphysis. 33 No similar studies could be found in the literature related to the frequency of iAFF localization. iAFFs are thought to start from the areas of highest tension, especially when the femur’s geometry is impaired, such as with bowing. Chen et al. examined 13 patients with iAFF and found a relationship between femoral bowing and iAFF localization. 34 In the current study, iAFFs were observed in the mid-third diaphyseal region at a rate of 82.4%.
The incidence of bilateral AFF has been reported in the literature as 25–44.2%. 21 In the current study, the bilateral iAFF rate was 21.4%, similar to the AFF rate. The ASBMR task force notes that when AFFs develop after the long-term use of bisphosphonates, incomplete fractures can form on the contralateral side. Screening of contralateral side of patients who have sustained a femoral insufficiency fracture is recommended. 12
In the current study, no statistically significant difference was found between the groups with and without iAFF in terms of the serum vitamin D and ALP levels or the total femur and spinal T-scores. PTH levels were significantly higher in the iAFF group. In contrast, La Rocca et al. reported that PTH levels were lower in an iAFF group; they attributed this PTH reduction to increased bone turnover. 28 A PTH analog, teriparatide, demonstrated to exhibit potent anabolic effects on bone and used for acceleration of bone healing in AFFs. 35 However, bisphosphonates could cause hypocalsemia with secondary hyperparathyroidism as an adverse effect. 36 Although serum calcium levels are not evaluated in our study, high PTH levels may have been encountered because of this side effect.
No randomized, controlled studies related to AFF treatment could be found in the literature. Treatment algorithms are generally opinion-based and tend to follow the consensus of the orthopedic surgeons on the ASBMR task force. When an incomplete stress fracture is identified, bisphosphonate treatment is terminated, and supplements are recommended according to the patient’s serum calcium and vitamin D levels. If the patient has no symptoms, follow-up is recommended with reduced weight-bearing; if the patient has symptoms, prophylactic nailing is recommended. 15 In 2017, Min et al. developed a weighted scoring system to identify the risk for impending complete fractures in iAFF based on radiographic and clinic findings. 17 They found that if the score is 9 or more, the probability for transforming a complete fracture is high and warrants prophylactic fixation. All of the scores of the patients in this study were 8 or below with this scoring system. For all iAFF-detected patients in this study, the antiresorptive therapy stopped immediately and protected weight-bearing with gait aids as tolerated was advised.
There were some limitations to our study. Bisphosphonate subgroups were not examined, and bone turnover markers were not measured. In addition, since the results were focused on a specific geographic region, regional and racial differences may have impacted the outcome. Besides that, a cohort with high number of patients using bisphosphonates for a long time may not represent a population with regulated and justified bisphophonate treatment. Also, the study did not search for iAFF that occurred in patients who were not taking bisphosphonates. Therefore, further extensive controlled studies including patients who have not taken bisphosphonate could provide more valuable results.
Conclusion
This study found iAFF in 10.6% of patients who were taking bisphosphonate, and 82.4% of these fractures were in the mid-third of the diaphysis. A higher iAFF incidence was found in patients with longer periods of bisphosphonate treatment and in patients with higher PTH levels. Some iAFF patients do not present at hospital, either because they are asymptomatic or do not have severe symptoms, so iAFF prevalence cannot be correctly calculated based only on patients who present at the hospital. Bisphosphonates have been proved to be effective in reducing the risk of hip and spinal fractures in patients with osteoporosis; therefore, the results of this study do not mean that these drugs should be discontinued. Increased iAFF awareness could lead to early diagnosis of these fractures. Early iAFF identification could prevent the catastrophic transformation to complete fractures, reducing patient morbidity and hospital costs.
Research Data
Research Data abstract for Incomplete atypical femoral fractures after bisphosphonate use in postmenopausal women
Research Data abstract for Incomplete atypical femoral fractures after bisphosphonate use in postmenopausal women by Umut Canbek, Ulas Akgun, Deniz Soylemez, Tugba Dubektas Canbek and Nevres Hurriyet Aydogan in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.