
Abstract
Medial collateral ligament injury of the first metatarsophalangeal (MTP) joint is rare. If it is missed, chronic instability and traumatic hallux valgus develop, requiring surgical treatment. Different methods have been reported in the limited available literature aiming to restore the balance between the lateral and medial stabilizers by tightening the medial joint capsule with or without additional tendon graft. Our described method utilizes a suture button device (Mini TightRope, Arthrex, Naples, Florida) for reconstruction. This device applies tension to hold the hallux in the correct position, providing stability. Relevant diagnostic regimen, surgical technique, and postoperative care are described, along with a case of a handball player who underwent this procedure. He continues to perform at the same level 38 months postoperatively. Mini TightRope fixation for chronic medial first MTP instability has not been reported. It does not require postoperative immobilization and allows faster return to sport, so it seems superior to other methods when treating athletes.
Keywords
Introduction
The frequency of first metatarsophalangeal (MTP) joint injuries in the athlete population is increasing, and therefore, this area has gained more importance recently. 1 These injuries could be challenging to diagnose and treat. Most of these cases are affecting the plantar MTP-sesamoid complex resulting in a classical turf toe, which is a more easily recognizable entity. However, forces from the horizontal direction can result in medial collateral ligament injury, which is very rare and therefore could be overlooked. If it remains unrecognized, it can lead to chronic instability of the first MTP joint and traumatic hallux valgus deformity. 2 Very limited number of publications are accessible in this topic due to the rarity of the condition. If there is no treatment in the acute stage or the nonoperative treatment fails, then chronic medial instability can develop, which may require surgical treatment. 3 For athletes, the reconstruction is expected to be powerful and should allow fast rehabilitation.
Case report
A 23-year-old handball player sustained a valgus trauma to his right hallux when another player’s foot crashed onto his foot while landing from a jump. Six days after the injury, he presented at the clinic with swelling and painfully restricted movements of the first MTP joint. The physical examination revealed tenderness at the metatarsal origin of the medial collateral ligament and a positive valgus stress. Medially, the joint showed abnormal laxity without firm end point compared to the contralateral foot (Online Supplemental Video 1). No hallux valgus deformity was seen and no clinical evidence of systemic ligamentous laxity was observed. X-rays showed no bony abnormality.
Immobilization in a plaster cast positioned in slight varus was applied for 6 weeks, then he started physiotherapy and gradually returned to sport in an additional 3 weeks. Taping was used for sport activity for another 4 weeks. After being complaint free for a few months, his right hallux sustained another twisting injury during playing. At that time, the clinical presentation was similar to the previous occasion, regarding swelling, pain, and laxity. Still no remarkable hallux valgus deformity was noted. Magnetic resonance imaging (MRI) scan was done, which showed thickening of the medial collateral ligament at its metatarsal origin indicating ligament lesion (Figure 1). The same nonoperative treatment was tried with 6 weeks cast immobilization, which failed this second time. After the removal of the cast, he felt the instability during normal walking and was not able to get back to training. Hence, surgical reconstruction became necessary.
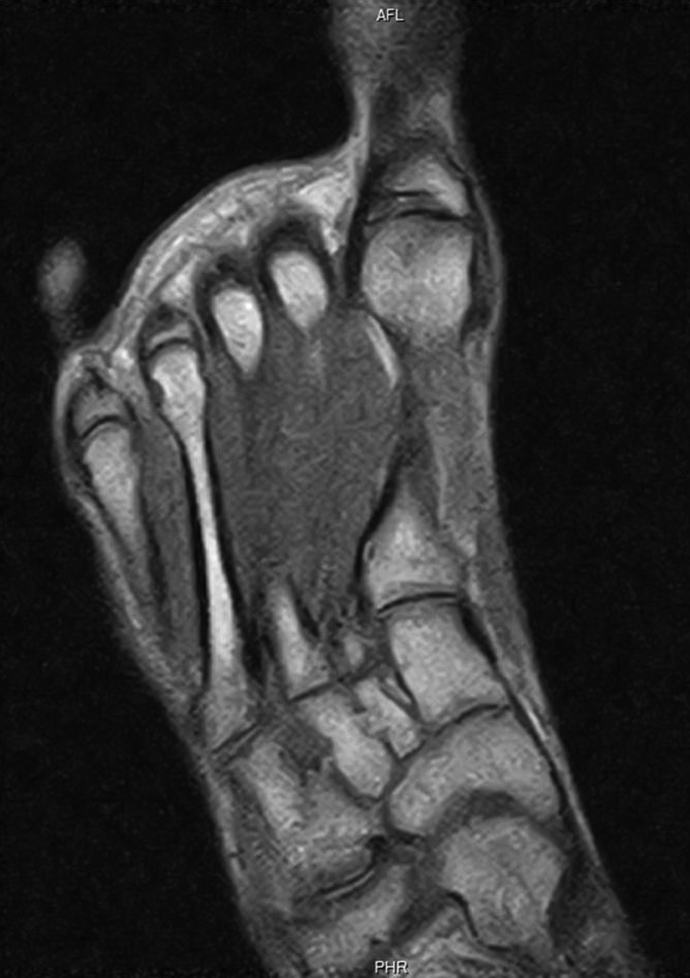
MRI of the injured foot. Thickening of the medial collateral ligament is shown at its proximal attachment indicating the lesion. MRI: magnetic resonance imaging.
Reefing of the medial joint capsule and additional dynamic stabilization was done using Mini TightRope® (Arthrex, Naples, Florida, USA) fixation system. It includes a nonabsorbable four-strand #2 thread and two endobuttons, one being oval and the other one is rounded in shape. A medial longitudinal incision was used over the first MTP joint and another shorter one in the distal first intermetatarsal space, identical to what is used for lateral soft tissue release in bunion surgery. Intraoperatively rupture of the medial collateral MTP ligament was found. After opening the medial capsule, two transosseal tunnels were created using 2.7 mm diameter cannulated drill over guide wires placed in the center of the metatarsal head and into the base of the proximal phalanx at its inferior third. The guide wires were placed in a divergent way from the joint line (Figure 2). The suture button device was pulled through the proximal tunnel from the lateral aperture of the tunnel with the oval button being in the front and then pulled through the distal tunnel from medial to lateral (Figure 3). Then, plication of the medial capsule was done by mattress sutures using #1 Vicryl. Subsequently, the oval button was flipped and the hallux was placed in the desired position. The Mini TightRope was tightened and the suture tied over the rounded button (Figure 4). The stability of the first MTP joint was assured (Online Supplemental Video 2). Consequently, neither temporary pinning nor plaster cast was needed. Only a corrective bandage was applied and he was heel weight-bearing in a wedge shoe for 6 weeks. Physiotherapy was commenced after 6 weeks. The range of movements of the first MTP joint remained slightly below the preoperative range but this resulted in no restriction in the normal daily activities and the patient was able to get back to training. He returned to play after 16 weeks postoperatively and he has been playing handball at preinjury level with no limitation and no discomfort ever since. At 38 months after the operation, he is free of complaints (Figure 5).

The guide wires are placed in a divergent way from the joint line. The distal tunnel is being created using a 2.7-mm diameter drill.

After the suture button device is pulled through the proximal tunnel, then it is placed into the distal tunnel and pulled through it from medial to lateral direction.

The hallux is shown in a proper alignment. In the distal part of the lateral incision, the oval button is shown, while in the proximal part of the incision, the knot is visible over the rounded button.

(a) A 38-month postoperative AP view radiograph showing distally the oval and proximally the rounded shaped endobuttons. (b) The same buttons are demonstrated on the lateral view radiograph. AP: anteroposterior.
Discussion
Diagnosis
Obtaining a detailed patient history, including a detailed description of the injury, along with a thorough physical examination is essential to obtain the right diagnosis. There is usually an acute valgus trauma to the great toe, such as an awkward landing on the great toe with some twisting of the foot. Swelling of the first MTP joint with painfully limited range of movements resulting in limping is usually noted. Tenderness over the medial collateral ligament and rarely ecchymosis can be indicative of medial collateral ligament injury, especially with positive valgus stress and laxity in 30 degrees of flexion compared to the contralateral side. In acute stage, there is no remarkable malalignment, only some insignificant hallux valgus and rotational difference could be seen compared to the hallux of the noninjured foot.
Plain radiographs are usually unremarkable, only some minimal lateral deviation of the hallux might be observed with relatively normal intermetatarsal angle and sesamoid position. 4 MRI could reveal disruption of continuity of the ligament or thickening of its attachment. Ultrasound scan in experienced hands can show thickening of the ligament tissue or a gap in its substance. Dynamic ultrasound scan can demonstrate laxity and abnormal opening of the joint medially, especially when comparing it with the uninjured foot. 5 Arthroscopy of the first MTP joint is also a possible option. 6 However, it requires very special skills and appropriate instruments for small joints.
Treatment
If the first MTP collateral ligament injury is recognized in an early stage, then nonoperative treatment may work. It involves plaster cast fixation in slight varus for 6 weeks or keeping the great toe’s position in a hallux valgus brace for the same period. Wearing a wedge shoe is recommended to unload the forefoot. Additional anti-inflammatory treatment locally by non-steroidal anti-inflammatory drug (NSAID) containing gel and/or oral anti-inflammatory medication for the initial days may also be considered. After the 6 weeks of immobilization and heel weight-bearing, the patient could commence full weight-bearing. For sporting activity, use of either a brace or taping is recommended. 7
If chronic first MTP instability develops, then surgical treatment is needed. Different ways of stabilization can be used. The simplest is plication of the medial capsule with mattress sutures. 8 A stronger reconstruction could be achieved with extensor hallucis brevis tendon autograft, which requires temporary postoperative fixation of the first MTP joint. 4 Tendon allograft could be used, as well. Any of these procedures require temporary pinning of the joint, postoperative plaster cast, or bracing for 6 weeks.
In our case, we used a novel method of dynamic stabilization, which has not been reported so far to our knowledge for this indication. Due to the immediate very strong stability allowing relatively fast rehabilitation, we believe that the technique used by us may be superior to other former techniques when treating athletes.
Mini TightRope has been used to treat several conditions in other locations, such as suspension of the first metacarpal after trapeziectomy, 9 forearm interosseus ligament reconstruction, 10 Lisfranc joint instability, 11 and acquired hallux varus due to lateral first MTP instability. 12,13 Its usage was also reported in conjunction with hemiarthroplasty of the first MTP joint for severe hallux abducto-valgus deformity in a diabetic woman with history of deep vein thrombosis, in whose case bony procedure and cast immobilization was preferably avoidable and immediate weight-bearing was desirable. 14
In our case, Mini TightRope was proven as an effective method for medial collateral ligament reconstruction of the first MTP joint. Compared to former methods, it provides immediate strong fixation. Consequently, there is no need for transarticular pinning or plaster cast, which may result in some initial stiffness and could delay the return to training.
Conclusion
First MTP collateral ligament rupture is a rare injury that can happen after valgus trauma to the hallux. In case of an acute injury, nonoperative treatment may be successful. Chronic MTP instability in the majority of cases should be managed surgically to provide stability and prevent the development of traumatic hallux valgus deformity. The presented method using Mini TightRope has not been reported so far for this indication. It provides a well-controlled tensioning opportunity, where the exact position of the great toe can be fine-tuned before committing to the position. In addition, it does not require immobilization of the joint and therefore allows faster rehabilitation, which is advantageous, especially for athletes. However, further research is required to ascertain the effectiveness and longevity of such treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.