
Abstract
The medial collateral ligament (MCL) of the first metatarsophalangeal (MTP) joint is key in maintaining joint stability and function. Evidence-based conservative management strategies for partial tears of the first MTP MCL are lacking. Historically, athletes experiencing persistent pain despite conservative management have required surgical intervention as the next step. In this case, a 34-year-old principal ballet dancer with a partial proximal MCL tear of the first MTP joint failed to improve with conservative treatment, including physical therapy. Treatment with leukocyte-rich platelet-rich plasma to the injured MCL and leukocyte-poor platelet-rich plasma to the first MTP joint was pursued, leading to an improvement of valgus laxity from 5.5 to 3.0 mm on dynamic ultrasound assessments. A full return to dance was achieved at 12 weeks post-injection, and the patient remained symptom-free at 22-month follow-up.
Keywords
Introduction
The medial collateral ligament (MCL) of the first metatarsophalangeal (MTP) joint is a critical stabilizer of the first MTP joint, and when injured, it can lead to the progression of traumatic hallux valgus.1-5 Injuries to the MCL of the first MTP joint are typically associated with an acute event involving dorsiflexion of the first MTP joint while a valgus force is applied.2-4,6 The MCL is also under great stress with a valgus force during sudden acceleration, such as pushing off with leaps and jumps. 2 This mechanism of injury progressively overloads the ligament, leading to ligament failure, partial tear, or complete tear, with gradual symptom development. 2
The first MTP joint and medial column of the foot support 90% of the ground reaction force during the heel rise phase of the gait cycle. 7 Dancing en pointe increases stress on the MCL of the first MTP joint, and leaping and jumping in dancers multiplies the ground reaction force on the forefoot several times that of bodyweight.
“The optimal PRP formulation for ligament partial tears remains unknown, and comparative studies—especially in small joints like the first MTP—are lacking.”
Conservative management of first MTP MCL partial tears includes a period of rest, physical therapy, prevention of joint dorsiflexion and valgus, toe spacer use, and footwear modifications. 4 When diagnosed early, these partial tears may heal without surgery. 4
In cases where MTP joint pain and laxity persist, more invasive treatment is needed. To date, evidence-based management strategies for partial tears of the first MTP MCL are lacking. The aim of this study is to report a case of partial first MTP MCL injury treated with platelet-rich plasma (PRP) in an elite ballet dancer.
Surgical repair is another treatment option. Surgery typically entails a direct repair of the MCL and in cases where hallux valgus has developed a modified McBride bunionectomy.1-3,8 Surgery has an extended recovery period, requiring 6 months to return to full activity.1-3,8 In some cases, surgery leads to restrictions in range of motion of the MTP joint, which can be career-ending for a dancer.1-3,6,8
Platelet-rich plasma has been studied as a surgical sparing alternative treatment for ligament partial tears, with the most evidence involving the ulnar collateral ligament (UCL) of the elbow and the MCL and anterior cruciate ligament of the knee.9,10
Case Presentation
A 34-year-old classical ballet dancer presented with an insidious onset of left first MTP joint pain. Her MTP joint pain was primarily medial and was worse when “en pointe.” The physical examination revealed normal hallux alignment at rest and during weight bearing, significant first MTP valgus laxity on the valgus stress test, and tenderness over the MCL and the first MTP joint line. A left foot radiograph demonstrated normal first MTP joint space, normal alignment, and no signs of arthrosis or fracture. Initial treatment included rest, anti-inflammatory medication, toe spacer, foot intrinsic muscle strengthening, dry needling, and a full-length graphite plate in her shoes. After no improvement, a 0.6-mL injection of ketorolac (30 mg/mL) was administered into the first MTP joint under ultrasound (US) guidance by the head team physician of the ballet company, a physical medicine and rehabilitation physician with subspecialization in sports medicine and extensive experience in US-guided procedures. The US machine used for this procedure was a Samsung HS60 (Samsung Medison, Seoul, South Korea), equipped with a linear transducer (LA3-14AD), operating at a center frequency of 12 MHz, a gain of 46, and a 2-cm depth, with the focal zone set at the level of the MCL. Since her pain persisted despite the ketorolac injection, a magnetic resonance imaging (MRI) of her left foot was ordered. The axial proton-density fat-saturated sequence revealed a partial tear of the proximal MCL of the first MTP joint, involving 50% of the deep ligament fibers, as shown in Figure 1. In addition, dynamic US assessment in the axial plane in relation to the anatomical position of the body (as with all the other US images described in this case report) with valgus stress performed by the aforementioned physician with the same US machine and transducer showed a medial joint widening of 5.5 mm (Figure 2).

Magnetic resonance imaging of the left foot showing the partial tear of the proximal MCL (arrow) of the first MTP involving 50% of the deep ligament fibers, shown in the axial proton-density fat-saturated sequence.
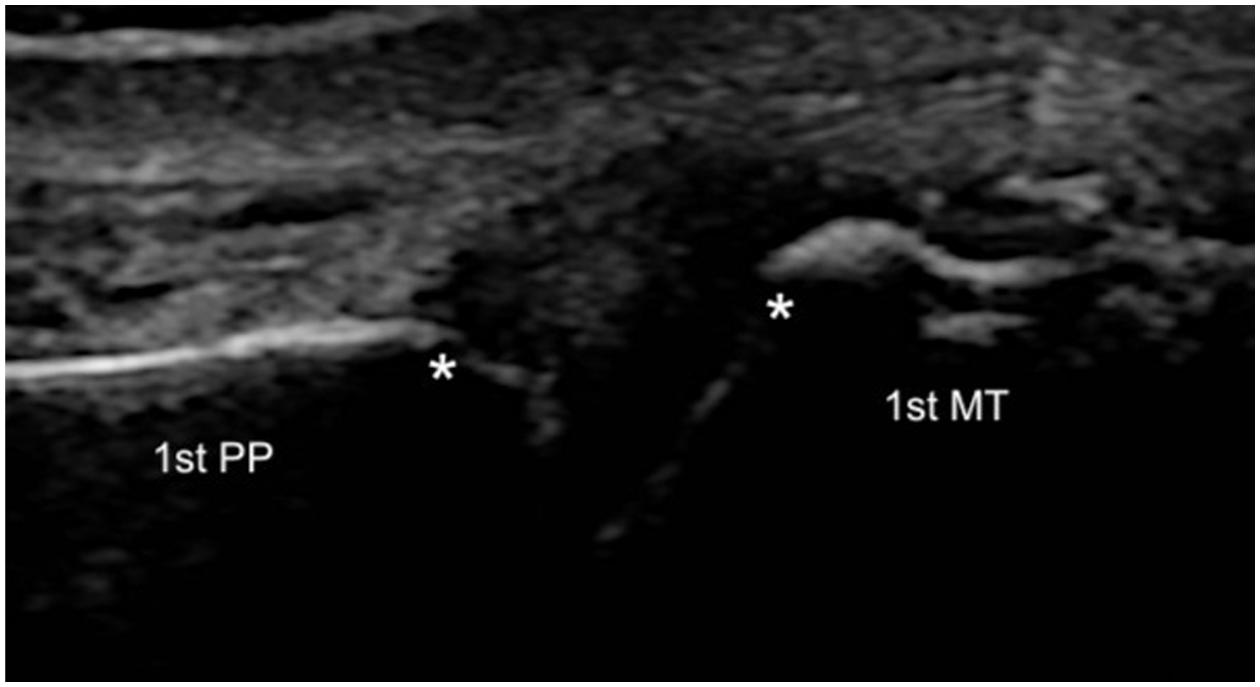
Dynamic ultrasound image of the first MTP joint in the axial plane (longitudinal axis to the first MTP joint) with valgus stress before PRP injection into the MCL, showing a medial joint widening of 5.5 mm. PP: proximal phalanx, MT: metatarsal, stars: joint space.
The medical team and the dancer decided to pursue a leukocyte-rich (LR) PRP injection into the MCL and a leukocyte-poor (LP) PRP into the first MTP joint.
For the PRP preparation, 108 mL of blood was drawn from the cephalic vein in the antecubital fossa with a 17-gauge needle and mixed with 12 mL of anticoagulant citrate dextrose solution, solution A (ACD-A). Using LR and LP settings (Arthrex Angel, Naples, Florida), half was centrifuged at “7% hematocrit” and the other half at “2% hematocrit,” respectively, to produce 1.75 mL each of LR-PRP and LP-PRP. Under US guidance and no platelet activator, the same physician injected the length of the MCL using a peppering technique with 1 mL of LR-PRP (Figure 3) and then 1 mL of LP-PRP into the MTP joint. A hematology analyzer was not available and a total platelet dose for each PRP was roughly estimated at 1.2 billion platelets in the 1ml of LR-PRP and 800 million platelets in the 1 mL of LP-PRP. This was calculated using the known concentration factors of the Arthrex Angel system and an average female platelet concentration of 225 000 platelets/μL.
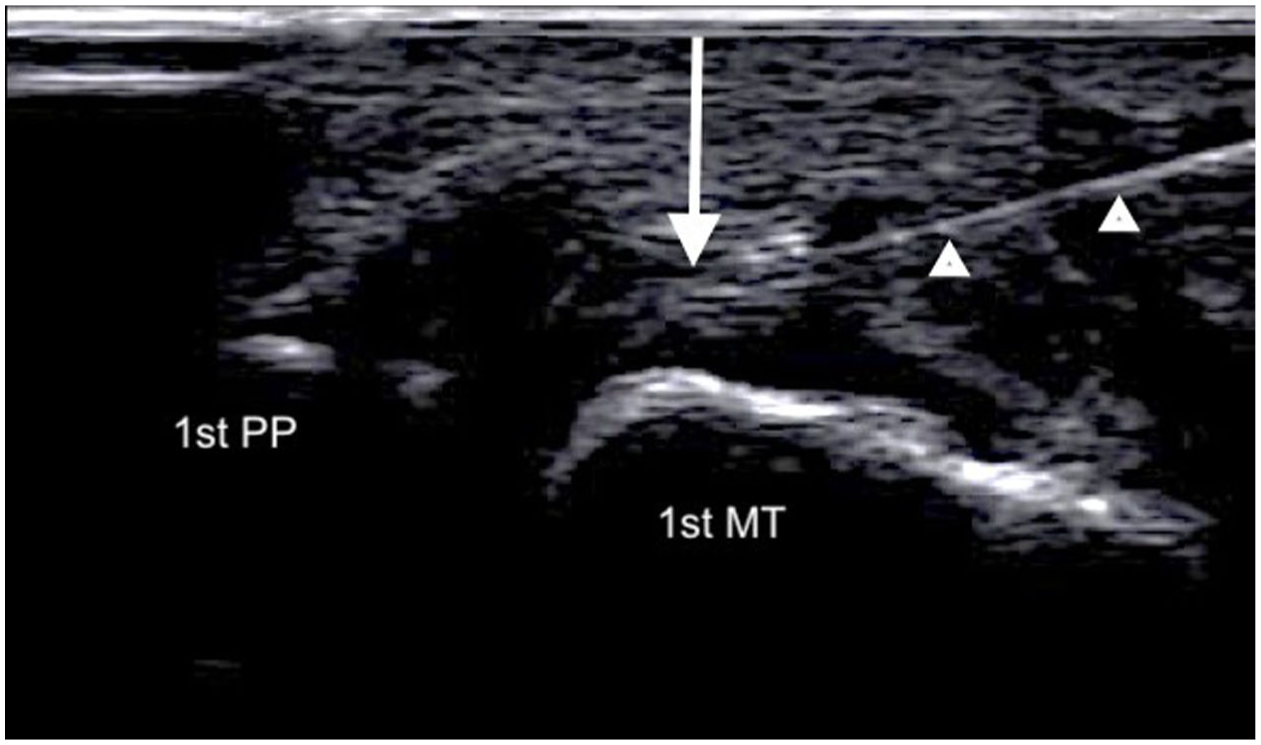
Ultrasound image of the first MTP joint in the axial plane (longitudinal axis to the first MTP joint) showing the ultrasound-guided PRP injection into the MCL of the first MTP using an in-plane proximal-to-distal approach. Arrow: MCL, arrow heads: needle.
Following the PRP injections, the patient was placed in an orthopaedic boot with continued use of the graphite plate and toe spacer. Two weeks following the procedure, she began physical therapy, and tapered out of the orthopaedic boot at 4 weeks. Dynamic US at 4 and 10 weeks post-procedure, performed by the same physician and with the same US machine, showed medial joint widening of 3.3 and 3.4 mm (Figure 4), respectively, with valgus stress. She returned to full dance at 12 weeks post-PRP injection with mild stiffness and was symptom-free at 18 weeks. At 22 months post-PRP, she remains symptom-free and continues to dance without limitations. Her medial MTP joint space was still 3.0 mm when tested with dynamic US valgus stress (Figure 5), again by the same physician and with the same US machine. A scatter plot was created to illustrate the dynamic US measurements of medial joint space widening at multiple time points over the 22-month follow-up period (Figure 6).
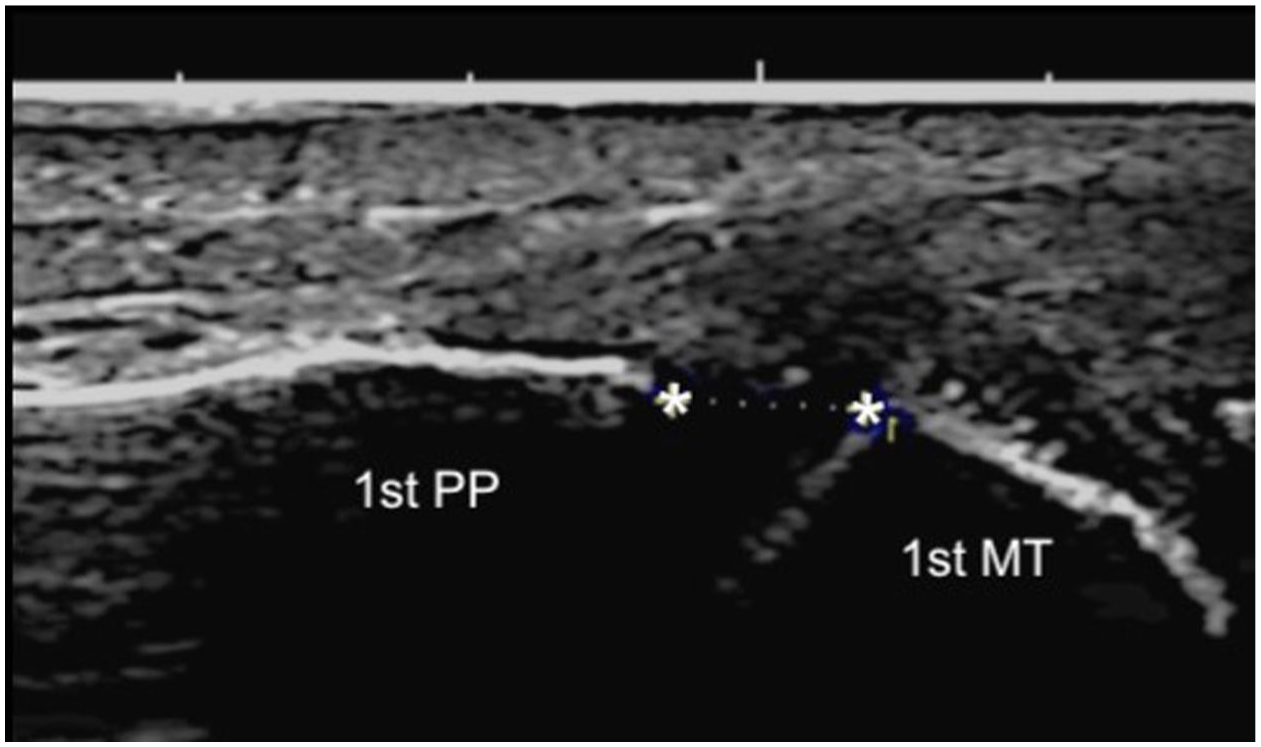
Dynamic ultrasound image of the first MTP joint in the axial plane (longitudinal axis to the first MTP joint) with valgus stress at 10 weeks post-PRP injection into the MCL, showing a medial joint widening of 3.3 mm. PP: proximal phalanx, MT: metatarsal, stars: joint space.
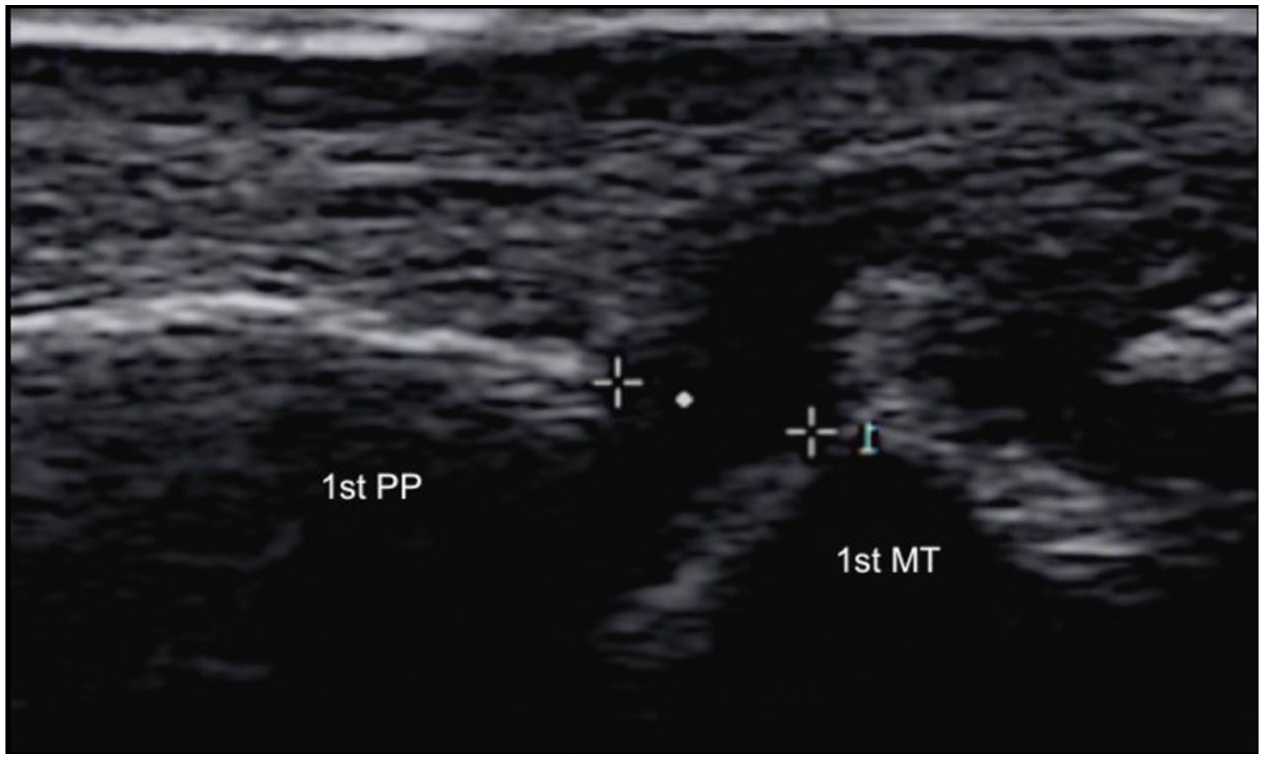
Dynamic ultrasound image of the first MTP joint in the axial plane (longitudinal axis to the first MTP joint) with valgus stress at 22 months post-PRP injection into the MCL, showing a medial joint widening of 3.0 mm. PP: proximal phalanx, MT: metatarsal, targets: joint space.
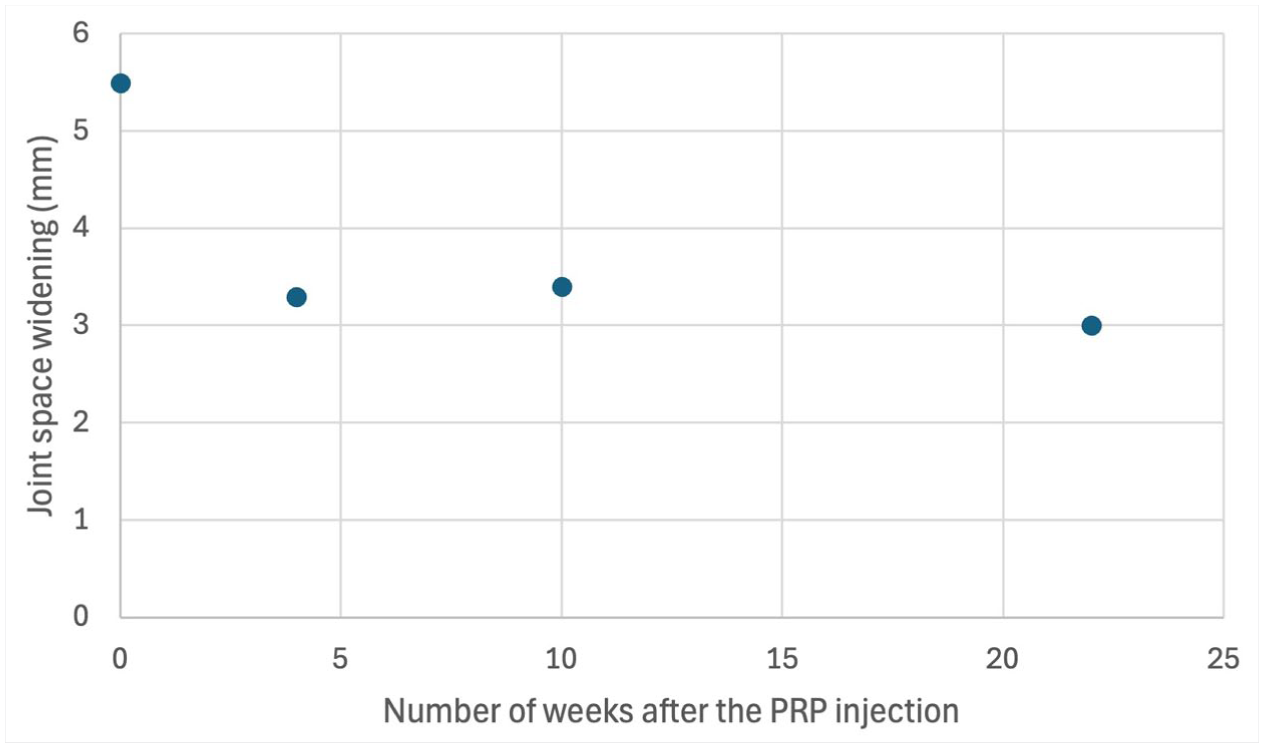
Scatter plot illustrating the dynamic ultrasound measurements of the medial first MTP joint space widening while applying valgus stress at multiple time points over the 22-month follow-up period.
Following return to pointe shoes, it was made apparent the shape of the previous shoe no longer fit her foot. They were modified with a widened toe box and lengthened vamp (top part of shoe that covers toes and the dorsal foot).
Discussion
In this professional classical ballet dancer, US-guided injection of LR-PRP into the MCL and LP-PRP into the joint of the first MTP joint followed by foot immobilization with an orthopaedic boot, a graphite plate, a toe spacer, and physical therapy provided complete relief, full return to professional dance, and spared her from surgery.
It is crucial to have a high index of suspicion for MCL injury in athletes presenting with first MTP joint pain. Early diagnosis and treatment is vital to prevent worsening ligament damage, progression to complete tear and progression to severe hallux valgus.2,4,6,7 When identified early, conservative treatment in the form of prevention of dorsiflexion, and toe spacer has shown to prevent progression to hallux valgus.1-4 This case demonstrates promise for PRP in improving pain and decreasing laxity from an MCL partial tear of the great toe.
While no studies have yet evaluated PRP for MCL injuries of the first MTP, evidence for PRP in other ligament partial tears creates optimism. Specifically, PRP treatment for partial tears of the UCL of the elbow demonstrated improvement in joint stability, higher return to play than those treated conservatively, and faster recovery than if treated with surgery. 9 A partial tear of the UCL following PRP injection is commonly assessed by measuring ulnohumeral joint space widening with US during a valgus stress, serving as an indirect sign of ligament healing.9,11 This same principle was applied in this study, where a decrease in the first MTP medial joint space widening was measured under US during a valgus stress to indirectly assess the MCL integrity before and after PRP injection. The results of this case report align with those of previous studies that treated partial tears of the UCL of the elbow and the MCL of the knee with PRP, which seemed to yield favorable outcomes.9,12,13 However, the current evidence base for PRP in UCL and knee MCL injuries remains limited. Systematic reviews highlight that much of the supporting data comes from small case series without randomization or control groups, and often includes confounding treatments.12,14,15 As no high-level studies currently exist for first MTP MCL injuries, extrapolation from other ligamentous injuries should be interpreted with caution.
There is conflicting evidence regarding the effect of PRP on the cellular and molecular aspects of ligamentous injuries, according to systematic reviews, possibly related to the heterogeneity in PRP preparation.16,17 Theoretically, platelets orchestrate the healing cascade required for ligament restoration. Platelet-rich plasma concentrates growth factors such as platelet-derived growth factor-AB, transforming growth factor beta, and vascular endothelial growth factor to augment and accelerate the healing cascade. 10 These growth factors stimulate cell proliferation; promote angiogenesis, immune cell recruitment; and coordinate the transition from a weaker type III collagen to a stronger type I collagen. 10 In addition, certain leukocytes found in the LR-PRP such as neutrophils, monocytes and macrophages, and associated cytokines such as tumor necrosis factor-alpha and interleukin-1, also contribute to angiogenesis and inflammation modulation, which are instrumental in the tissue repair process.18,19 LR-PRP may cause more short-term pain than LP-PRP after being injected into a ligament due to its pro-inflammatory cytokines like interleukin 1-beta and transforming growth factor-alpha, but it may promote soft tissue healing more than LP-PRP according to the aforementioned mechanisms.19-21 The role of leukocytes in ligament healing remains controversial, with some studies supporting their pro-regenerative potential and others linking them to excessive inflammation.
The optimal PRP formulation for ligament partial tears remains unknown, and comparative studies—especially in small joints like the first MTP—are lacking. Systematic reviews assessing the outcome of PRP for partial tears of larger ligaments, mainly the UCL at the elbow, have found promising short-term and long-term clinical outcomes, both with the LR-PRP and the LP-PRP.15,22 The lack of consensus is further complicated by the wide variation in how PRP is classified and prepared, prompting recent expert guidelines to emphasize the need for standardized protocols to ensure meaningful comparison across studies.23,24
The main limitation of this article is that it is a case report, which provides low-level evidence. In addition, the simultaneous use of multiple therapies—including intra-ligamentous and intra-articular PRP injections, foot immobilization with an orthopaedic boot, a graphite plate, a toe spacer, and physical therapy—limits our ability to specifically assess the effect of PRP on the first MTP MCL partial tear. Furthermore, it remains unknown which preparation of PRP better optimizes the healing process of a first MTP MCL partial tear. Regarding the assessment of MCL partial tear treatment outcomes with dynamic US, the inter-operator variability also represents a limitation of this study, which could be minimized in future studies by using the same osseus landmarks at every US assessment and using a dynamometer to apply the same force when performing the valgus stress.
Future studies, including prospective cohorts and randomized trials comparing LR-PRP, LP-PRP, and surgery for partial ligament injuries in small joints and using standardized dynamometers and validated questionnaires, are needed to guide optimal clinical decision-making and establish standardized protocols for PRP use.
Conclusion
In this recalcitrant case of a first MTP MCL partial tear in a professional classical ballet dancer, the patient successfully returned to dance 12 weeks after receiving a US-guided PRP injection to the MCL and joint, with complete resolution of symptoms and ligamentous laxity.
Footnotes
Acknowledgements
Not applicable
Data Availability
The data from this case report will be available upon request.
Declaration of Conflicting Interests
Michael Khadavi is a consultant for Arthrex. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This is a case report, which does not require IRB approval according to our university.
Informed Consent
The patient described in this case report gave consent to publish the clinical data and the MRI/ultrasound images.
Trial Registration
This is a case report, which does not need to be registered as a clinical trial according to our university.