
Abstract
Background:
Hydroxyapatite (HA)-coated stem has been introduced to decrease complications and eventually achieve quicker implant ingrowth and long-term stability. The aim of this study was to determine subsidence rate and incidence of perioperative periprosthetic fracture (PPF) of uncemented collarless Corail stem for displaced femoral neck fractures according to Dorr type.
Methods:
A retrospective review of plain radiographs and clinical data was carried out to identify consecutive patients who underwent uncemented hip hemiarthroplasty using collarless HA-coated Corail stem between March 2010 and August 2014. The risk of subsidence and PPF according to Dorr type was evaluated.
Results:
Dorr types A, B, and C were found in 66 (median age 74, 29.7%), 107 (median age 77, 48.2%), and 49 (median age 80, 22.1%) cases, respectively. Subsidence of stem occurred in eight (3.6%) cases. Dorr type had significant relationship (p < 0.05) with subsidence. Type C canals had higher rates of subsidence. PPFs occurred in 11 (5.0%) cases without showing significant difference among Dorr types not significant (n.s.). Female gender was not influential on subsidence (n.s.) and PPF (n.s.).
Conclusion:
Dorr type C had higher risk of subsidence when using uncemented collarless HA-coated stem. Dorr canal type had no bearing on risk of PPFs. Women did not have significantly higher risk of both subsidence and PPFs compared to men. A collarless fully HA-coated Corail stem had 3.6% of radiological subsidence and 5.0% of PPF risk.
Introduction
In 1961, Sir John Charnley pioneered the hip replacement operation. 1 Since that, Dr Dorr presented an article to assess bone quality of proximal femur, help selection of therapeutic option, and predict durability after arthroplasty in 1993. 2 The article classified proximal femur into A, B, and C types according to its bone quality and morphology (Figure 1). He proposed cortical index (CI) with higher CI indicating thicker bone. He also proposed a calcar to calcar isthmus ratio with higher ratio meaning more cylindrical proximal femur. Based on these concepts, Dorr C type is likely to cause higher incidence of subsidence and perioperative periprosthetic fracture (PPF).

Dorr classification of proximal femur.
Subsidence rates of femoral stems are variable. Cawley et al. have reported that only 2 patients among 36 patients were noted to have subsidence which measured less than 5 mm of the uncemented hydroxyapatite (HA)-coated stem for the treatment of femoral neck fractures in radiostereometric analysis. 3 However, Pentlow and Heal have reported mean 4.27 mm subsidence in the trauma patients in the same collarless Corail stem occurring in 6–12 months postoperatively. 4 It is known that subsidence of more than 5 mm indicates unsatisfactory long-term outcome such as stem breakage and loosening. 5
PPF risks are also variable ranging from 3.2% to 7.3%. 6 –8 Wider femoral canal types such as Dorr type B and C may be associated with more severe osteoporosis and higher risk of perioperative fracture. 9 On the other hand, one study has reported that patients with a perioperative fracture of the calcar have smaller and narrower femurs than those without a fracture. 10
HA coating for the fixation of a femoral stem has been introduced to achieve quicker biological fixation. Corail stem as a good example steadily used currently was developed in France in 1986. It is totally coated with 150 µm thickness HA. It has been reported that Corail stem has long-term survival rate. Corail stem has been reported to have fewer complications and an outcome to equal that of a cemented stem, suggesting that the use of this stem would result in a decreased rate of morbidity in trauma patients. 7
However, clinical data of this HA-coated stem for Asians are insufficient. Since Asian population appears to have narrower and different femur morphology compared to Whites 11 and Asian women have lower bone mineral density (BMD) compared to age-matched women of the White race, 12,13 risks of subsidence and PPFs in Asians may be different from those in Western people.
The purpose of this study was to investigate the subsidence rate and incidence of PPF of uncemented collarless Corail stem for displaced femoral neck fractures according to Dorr type in Korean population.
Material and methods
This research project has been reviewed and approved by the Institutional Review Board of the authors’ affiliated institutions.
Plain radiographs and clinical data of 222 consecutive patients who underwent uncemented elective hip bipolar hemiarthroplasty for displaced intracapsular femoral neck fractures between March 2010 and August 2014 were retrospectively reviewed. All operations were performed directly by the senior author. During the study period, Corail stem was used in most of the cases except three patients. Other stems were used for these three cases and excluded. All operations were done by posterolateral modified Gibson’s approach using Corail stems (DePuy, France, SAS) without cementation.
Operative technique
Preoperative templating was done to determined the femoral size and proximal femur geometry. The surgical procedures were generally the same. Patients were placed in the lateral decubitus position. The hip was exposed by the posterolateral approach and broached serially in one size increments until a press-fit was achieved. The rasp was inserted to the proximal femur in the same degree of version as the neck. Based on the preoperative templating, modular head with proper neck length was introduced. A trial was performed with the broach and final appropriate trial head was measured intraoperatively until a stable construct was achieved. A 28-mm inner head was used with a neck length from 1.5 mm (short) to 8.5 mm (long) and the appropriately sized bipolar shell as measured was assembled. After the hip was reduced, a drain was inserted and the wound was closed.
Inclusion criteria were as follows: (1) all age; (2) hip bipolar hemiarthroplasty performed between March 2010 and August 2014; (3) primary bipolar hemiarthroplasty performed for displaced intracapsular femoral neck fractures using modified Gibson’s posterolateral approach; (4) uncemented collarless Corail stem was used; (5) radiological and clinical data were available immediate postoperatively at 3 months, 1 year, and 2 years after surgery; and (6) postoperatively ambulatory patients. Exclusion criteria were as follows: (1) follow-up loss; (2) other combined complications such as periprosthetic joint infection; and (3) cases that other stems were used.
Radiologic parameters
These patients were followed up for a minimum of 2 years after surgery. Two independent investigators (clinical fellows in hip and pelvis division) assessed radiographs from preoperatively, immediate postoperatively, and at 3 months, 1 year and 2 years postoperatively to classify the proximal femur based on the Dorr type and subsidence. Since Dorr classification had no clear quantitative criteria, CI on anteroposterior radiographs to classify was used. 14 To evaluate the reproducibility of the Dorr classification, the Dorr type was calculated twice each by two observers. When classifying Dorr type on preoperative plain radiography, preoperative electronic radiographs were used. A reference line was drawn through the mid-lesser trochanter. A second line paralled to the reference line was drawn 100 mm below. At this level, the intramedullary canal diameter (X) as well as the femoral canal diameter (Z) were measured (Figure 2). The CI was calculated (Z − X/Z). Cutoff points were 0.58 between type A and B and 0.49 between type B and C on the anteroposterior radiograph. Subsidence using the Engh and Massin method 15 immediate postoperatively and at 1 year postoperatively was measured (Figure 3). Subsidence more than 2 mm was reported as significant since 2 mm change was the minimum required to show subsidence. Also the risk of PPF according to the Dorr type was evaluated.

Method of measuring Dorr classification using plain radiograph is shown. CI: cortical index.
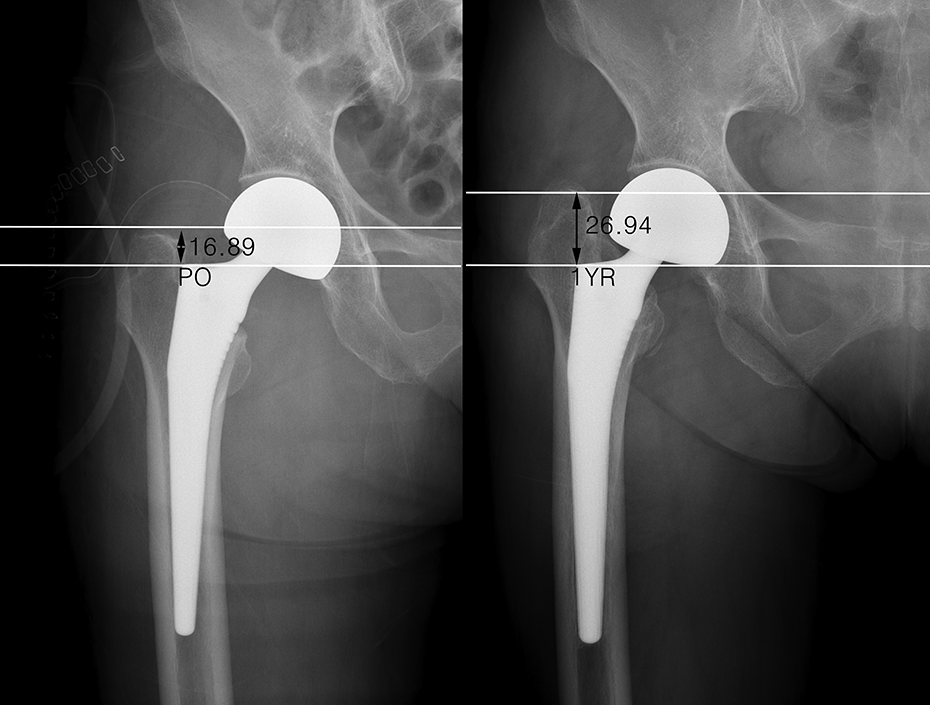
Measuring subsidence using the Engh and Massin method.
Statistical analysis
Statistical analysis was performed using SPSS 20.0 software (SPSS, Inc., Chicago, Illinois, USA). Shapiro–Wilk tests were used to assess normality of distribution. Reproducibility was assessed based on the intraclass correlation coefficient (ICC). Inter-rater reliability was also analyzed. All of the results were analysed using χ2 test.
Results
From March of 2010 to August of 2014, a total of 237 patients underwent bipolar hemiarthroplasty due to displaced femoral neck fractures. Of these patients, 12 were excluded due to follow-up loss or other complications (nine cases lost to 3 months follow-up and three cases of infection);3 were excluded since other stems were used. Finally, 222 patients were enrolled in this study.
There were 47 males and 175 females. The median age at the time of hip arthroplasty was 76 years (range, 60–102 years). There were 66 (29.7%) cases of Dorr type A, 107 (48.2%) cases of Dorr type B, and 49 (22.1%) cases of Dorr type C when the CI was used as the reference radiographic index for the classification (Table 1). The correlation coefficient of inter-examiner reproducibility was 0.982 (95% confidence interval: 0.973–0.988; p < 0.05). Regarding intra-examiner reproducibility, the ICCs were 0.971 and 0.978. Cases of subsidence of stem and PPF including calcar cracks and other periprosthetic fractures were investigated according to Dorr Type.
Demographics of patients according to dorr type.

M: male; F: female.
Eight cases (three cases of Dorr type B and five cases of Dorr type C) had a subsidence of more than 2 mm at 1 year follow-up (Table 2). Stem sizes in eight patients ranged from 11 to 15 (except size 13). There was a 3.6% risk of subsidence. χ2 Test indicated Dorr type had statistically significant relationship with risk of subsidence (p < 0.05; Table 1). In patients who subsided, there were one male and seven females. However, statistically significant difference was not found according to gender not significant (n.s.). Two patients (one case of Dorr type B and one case of Dorr type C) had no fracture and six patients (two cases of Dorr type B and four cases of Dorr type C) had subsidence secondary to missed calcar cracks or other periprosthetic fractures including three cases of lesser trochanter fracture (medial calcar fracture that extend below the lesser trochanter). These six fractures were noted only on postoperative radiographs. They were managed using a non-weight-bearing for 6 weeks with partial weight-bearing for another 6 weeks. For these patients, repeat radiographs were taken 2 weeks, 3 months, 1 year, and 2 years after surgery for further evaluation of subsidence. All the fractures had healed at 1 year follow-up and all of them demonstrated stem stabilization at 2 year follow-up. Of these eight subsidences, none of these patients were symptomatic and required a further revision.
Stem subsidence.

Collarless uncemented fully HA-coated Corail stem had about 5.0% risk of PPFs. Overall, 11 patients (three cases of Dorr type A, three cases of Dorr type B, and five case of Dorr type C) had perioperatively calcar or periprosthetic fractures, of which five case (three case of Dorr type A, one case of Dorr type B, and one case of Dorr type C) were recognised well intraoperatively and cablings were done. There was no change in postoperative rehabilitation or physical therapy for patients with cabling fixation. These fractures that had undergone cablings showed no subsidence during the follow-up. However, six patients (two cases of Dorr type B and four cases of Dorr type C) were missed. They were associated with subsidence. χ2 Test indicated Dorr type had no statistically significant relationship with risk of PPFs (Table 1; n.s.). In patients who had PPFs, there were three males and eight females. Also, no significant difference was observed according to gender.
Discussion
Among 222 cases, problem such as subsidence and PPFs occurred in 13 (5.9%) cases (Figure 4). Subsidence of stem occurred in eight (3.6%) cases. Subsidence was associated with Dorr B and C. Relatively wider Dorr canal types such as B and C were found to have statistically higher risk of subsidence, different from a recent report showing that Dorr type had no significant relationship with risk of subsidence. 16

Statistical analysis: Subsidence and PPFs using collarless HA-coated stem for displaced femoral neck fractures according to Dorr type. PPF: perioperative periprosthetic fracture; HA: hydroxyapatite.
Proximal femur morphology changes with age. 17 Wide canal and increased endosteal diameter are associated with significant reduction in canal index and characteristics of Dorr type C. Usually, subsidence and PPFs can occur either due to surgical error in an attempt to achieve an interference fit or due to high energy levels to obtain press-fit in a wider osteoporotic Dorr canal. 18 For this reason, Dorr C might be associated with older patients. Therefore, age may be the culprit as opposed to the Dorr grade.
PPFs occurred in 11 cases (5.0%) that were not statistically significant according to Dorr type (n.s.). With regard to the impact of gender, the share of women was high for subsidence and PPF. However, this difference was n.s. It is well-known that proximal femoral morphology and BMD differ between Asian and Western women. 11 –13 Compared to Caucasian women, Asian women have significantly lower BMD at the lumbar spine, total hip, and femur. On the other hand, there is no difference in bone quality or BMD between Asian and Western men regardless of age. 19,20 Several articles reveal the importance of BMD for treatment with uncemented collarless stem. 21,22 When inserting an uncemented femoral stem slightly larger than the prepared femoral canal, operation procedure can produce compression hoop stress. Lower bone density and different morphology can lead to different results. For these reasons, the risk of subsidence and PPF in Asian women might be higher than that in Asian men. Although female gender did not show statistically significant relations with the risk of subsidence and PPFs, there were more women. Other retrospective studies performed in Western United Kingdom have also shown no statistically significant difference in subsidence or perioperative fracture between males and females. 16,23
Uncemented stems rely on biological osteointegration of bone to the surface of the prosthesis. For this reason, femoral stem tends to be slightly larger than bone canal to obtain press-fit. In 2017, a meta-analysis was published, including five randomised controlled trials (RCTs) comparing cemented and uncemented hemiarthroplasty. 24 In this article, there was no statistically significant difference in any other outcome between these two methods of fixation except that there were different outcomes about implant-related complications in the uncemented stem. Prosthesis-related complications such as periprosthetic fractures and reoperations were significantly higher in the uncemented group of femoral neck fractures. 25 Also uncemented stem has higher micromotion than cemented stem in the human cadaver study. 26 Although cemented stem achieves stability through a solid bond between stem, cement, and bone within the cement mantle, uncemented prosthesis may improve bonding through coating bioactive materials. 27 Since HA coating may also encourage osseous bonding due to its osteoconductive properties, HA-coated stem could be an option with excellent outcomes, particularly in the osteoporotic elderly women even though. 28
Collared stem did not be used. The roll of collar in cementless arthroplasty has been a topic of debate. The use of collar is unlikely to cause differences in biomechanics of bone–implant interaction on in vivo and in vitro studies. 29,30 However, further analysis is needed before generalizing these findings.
This study presents clinical data of the Asian population. However, our sample size was large than any previous study. In addition, textbook example of posterolateral-modified Gibson’s technique was used. Follow-up period was enough for evaluation of subsidence since most subsidence and fractures occur within the first year. 31
However, this study is limited by the use of retrospective data and did not give the robustness of data offered by prospective data collection. Stem subsidence may depend on the compatibility of the stem shape and the geometry of the proximal femur. Furthermore, many of perioperative fractures may depend on the technical skill of the surgeons. Preoperative planning and surgery by one surgeon with same surgical technique could minimize bias. Also, because cemented stem did not be used, collared with collarless stems could not be compared either. A larger prospective randomized study is needed in the future to obtain higher level of evidence.
Conclusion
Wider Dorr canal types were found to have higher risk of subsidence when we used collarless HA-coated stem. However, Dorr canal type had no bearing on the risk of PPFs. Women did not have significantly higher risk of both subsidence and PPFs compared to men. A collarless fully HA-coated Corail stem had only a 3.6% risk of radiological subsidence and 5.0% risk of PPF.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.