
Abstract
Background:
Direct anterior approach (DAA) is known to diminish a dislocation risk and widely used for total hip arthroplasty (THA). On the other hand, anterior dislocation due to increasing stem anteversion and cup anteversion is an important complication.
Methods:
A retrospective analysis of 140 (male/female: 10/130) consecutive patients with 149 hips who had undergone primary THA in the period between 2011 and 2015 was conducted. Factors including age, gender, body mass index (BMI), and primary diagnosis were examined. Radiographic parameters including the Dorr proximal femoral types, cortical thickness index (CTI), canal flare index (CFI), and canal to calcar index were measured. To investigate relationships of combined anteversion (CA) with other factors, a stepwise regression analysis was performed.
Results:
The mean age, BMI, and the follow-up period were 69.5 ± 10.3 years old, 23.4 ± 3.4 kg/m2, and 48.2 ± 13.6 months, respectively. The proximal femurs of the 149 hips were categorized as Dorr type A (n = 33), type B (n = 110), and type C (n = 6). The mean CTI, CFI, and canal to calcar index were 0.56 ± 0.08, 4.15 ± 0.83, and 0.46 ± 0.09, respectively. The mean stem varus angle, radiographic inclination, and radiographic anteversion of the cup were 0.19 ± 1.63, 40.9 ± 6.0°, and 12.7 ± 3.5°, respectively. Stem anteversion measured by computed tomography (CT) axial image was 17.7 ± 12.0°. The mean radiographic inclination, radiographic anteversion (CTRA), and anatomical anteversion analyzed by Kyocera 3-D template were 40.8 ± 7.2°, 19.8 ± 6.6°, and 28.8 ± 10.0°, respectively. Mean CA defined as the sum of stem anteversion and CTRA was 37.5 ± 14.5°. To investigate relationships of CA with other factors, a stepwise regression analysis was performed and resulted in a model with age (p < 0.001). In the same way, stem anteversion and CTRA were analyzed; only for the stem anteversion, the stepwise selection process resulted in a model with age (p < 0.001) and the Dorr types (p = 0.047).
Conclusion:
The risk of excessive femoral anteversion increases for relatively younger age and for types of femoral morphology according to the Dorr classification, moreover with an increase of CA in DAA-THA with cementless tapered-wedge stem.
Keywords
Introduction
The direct anterior approach (DAA) for total hip arthroplasty (THA) (DAA-THA) is a surgical approach that preserves the hip abductors, the posterior capsule, and the short external rotators. 1 It is known that DAA-THA diminishes a dislocation risk and the need for precautions for the postoperative hip is reduced. 2 However, some researchers are concerned that DAA-THA may introduce new problems related to a reduced visual field during surgery, such as neurovascular injury, poor implant fixation, 3 and implant malposition. 4 A usual dislocation occurred following DAA-THA is an anterior dislocation unless the acetabular or femoral components are significantly retroverted on implantation. 5 There have been little literature published regarding factors increasing stem anteversion and cup anteversion with DAA-THA. The purpose of this study is to research the contributing factors that increase the combined anteversion (CA) in DAA-THA.
Methods
Patients and surgery
A retrospective analysis of 140 consecutive patients with 149 hips who had undergone primary THA in the period between October 2011 and June 2015 followed by postoperative computed tomography (CT) under their approval was performed. Patients with severe acetabular deformity or severe flexion contractures were excluded and those surgeries were performed with a posterolateral approach (PLA) during the time period of this study. There were 18 male patients with 19 hips and 122 females with 130 hips (Table 1). The mean age at the time of operation was 69.5 ± 10.3 years (range 51–89 years), and the body mass index (BMI) was 23.4 ± 3.4 kg/m2 (range 17.9–34.3 kg/m2). The mean follow-up period was 48.2 ± 13.6 months (range 30–74 months). The diagnoses upon surgery were osteoarthritis (OA) for 128 hips, idiopathic femoral necrosis for 10 hips, femoral neck fracture (Garden stage IV) for 8 hips (we used THA for patients younger than 70 years with Garden stage III and stage IV), nonunion after surgery for femoral neck fracture for 2 hips, and femoral neck fracture Garden stage III with developmental dysplasia of hip joint (DDH) for 1 hip (Table 2). All the stems used were cementless tapered-wedge types, and Accolade II® stem (Stryker Orthopaedics, Mahwah, New Jersey, USA) and the Taperloc Complete Microplasty Hip Stem® (Zimmer Biomet, Warsaw, Indiana, USA) were used for 132 hips and for 17 hips, respectively. All the cups except for two cases had cementless designs, and Trident Acetabular System® (Stryker), G7 OsseoTi Acetabular System® (Biomet), and X3 RimFit® (Stryker) were used for 130 hips, for 17 hips, and for 2 hips, respectively. All surgeries were performed with DAA by the total number of six operators, as previously described. 1,5 Our target was to maintain the cup inclination in the range of 40 ± 10°, the cup anteversion in 15 ± 10°, 6 and stem anteversion to be 15°.
Summary statistics of demographic data.

SD: standard deviation.
Summary statistics of diagnosis and gender (n = 149).
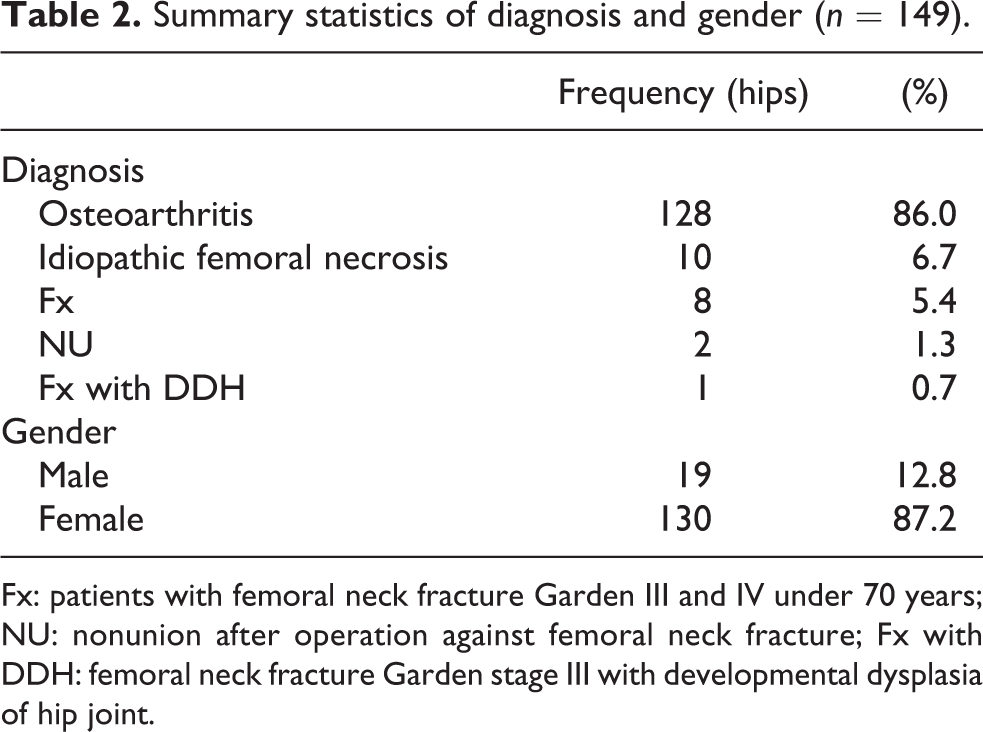
Fx: patients with femoral neck fracture Garden III and IV under 70 years; NU: nonunion after operation against femoral neck fracture; Fx with DDH: femoral neck fracture Garden stage III with developmental dysplasia of hip joint.
Postoperative measurement
Based on the X-ray analysis for the pelvis in the supine position obtained before the surgery, the Dorr types, the cortical thickness index (CTI), the canal flare index (CFI), and the canal to calcar ratio (CCR) were determined (Table 3). According to the Dorr description of the types of proximal femoral morphology, 7 type A exhibits thick cortices that begin at the distal end of the lesser trochanter and thicken quickly, producing a funnel shape and a narrow diaphyseal canal. Type B exhibits bone loss with medial and posterior cortices. The proximal portion of the posterior cortex is thin or absent, which results in an increased intramedullary canal width. Type C exhibits considerable loss of thickness in the cortices, resulting in a very wide intramedullary canal and a fuzzy appearance to the bone cortices. The CTI was defined as the ratio of the femoral shaft width minus the medullar width to the femoral shaft width at 100 mm below the tip of the lesser trochanter. 8 The CFI is a parameter for morphologically classifying the proximal femur. It was defined as the ratio of the intracortical width of the femur at a point 20-mm proximal to the lesser trochanter and at the canal isthmus. For consistent measurements, we identified the canal isthmus at 10 cm below the mid lesser trochanter. 7 The CCR was measured as described by Dorr et al. 8 A horizontal line at the mid-lesser trochanter was established on the AP hip radiograph. The intramedullary femoral canal width was measured as the distance between the medial and lateral markers at the 10-cm level. The CCR was calculated as the fraction of the isthmus canal width divided by the calcar canal dimension. Femoral stem varus angle was an angle between the stem and the femoral shaft on the X-ray image of the pelvis in the supine position obtained just after the surgery. Stem anteversion was calculated as the Nakashima’s method 9 (Figure 1). The radiographic inclination measured by plain radiographs (XPRI) is the angle between a line joining the ischial tuberosities and the long axis of the acetabulum 6 (Figure 2). The radiographic anteversion measured by X-ray (XPRA) was measured with the Lewinnek’s method 6 (Figure 3). Radiographic inclination (CTRI) and radiographic anteversion (CTRA) were calculated by the Kyocera 3D-template (Kyocera Medical, Osaka, Japan) and a THA planning software. We loaded postoperative CT images into the software and measured the angle of the cup inclination and anteversion. The CA (the sum of stem anteversion and cup anteversion) was calculated by stem anteversion and CTRA. CT scan and X-ray images were reviewed by a single observer (an orthopedic surgeon). This research has been approved by the institutional review board of the authors’ affiliated institution.
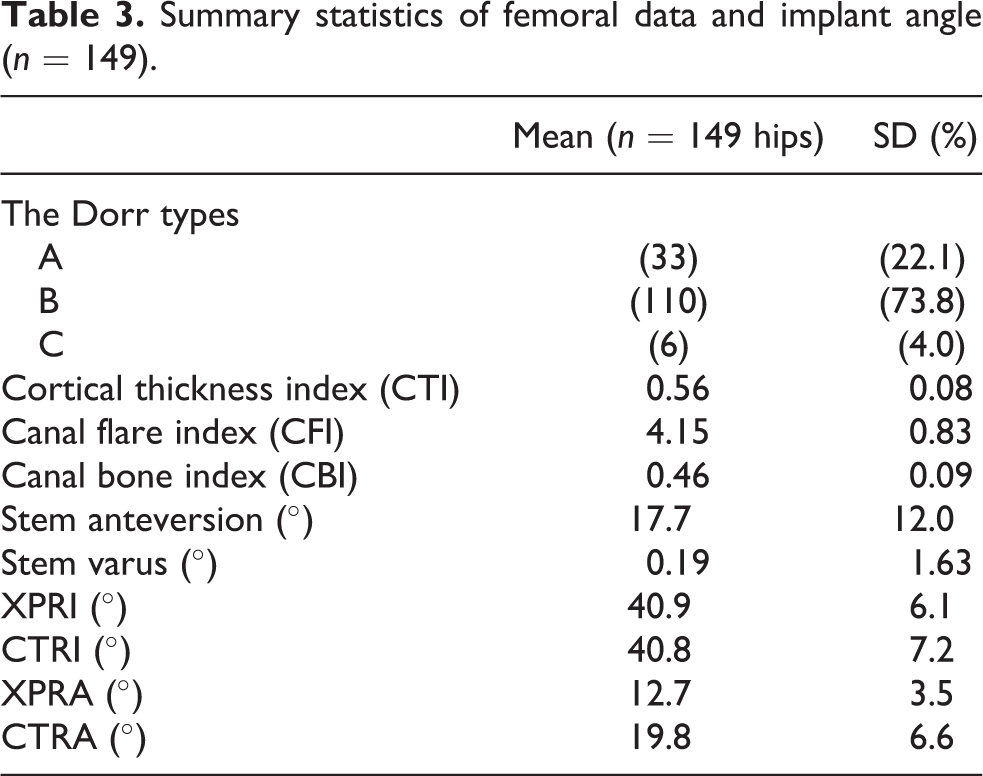
Summary statistics of femoral data and implant angle (n = 149).

Femoral stem anteversion was calculated as the angle between a line from the head of the femoral prosthesis to the center of the proximal femoral diaphysis and a line connecting the medial and lateral femoral condyles, indicated by asterisk.
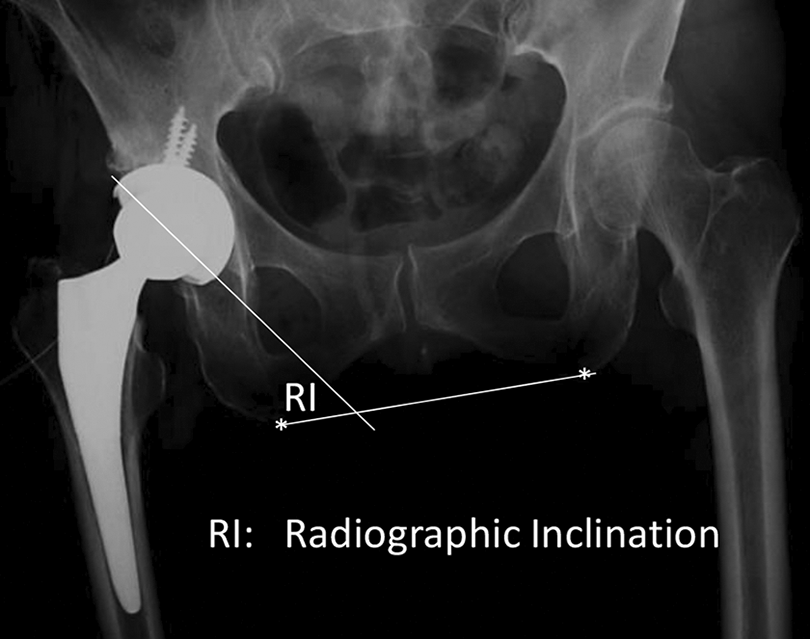
XPRI is the angle between a line joining the ischial tuberosities, indicated by asterisk, and the long axis of the acetabulum, shown as an ellipse. XPRI: radiographic inclination measured by plain radiographs.

In Lewinnek’s method, d is the short axis of an ellipse drawn perpendicular to the long axis of the implant; D is the long axis that is maximal diameter. XPRA = sin−1(d/D). XPRA: radiographic anteversion measured by plain radiographs.
Statistical analysis
Although consecutive patients in a fixed period were enrolled in this study, the sample number was not based on the testing hypothesis as this study was retrospective. No formal statistical comparisons for the measurements were planned or conducted, so the type I error was not controlled for multiplicity. To investigate relationships among CA, cup anteversion, stem anteversion, and other factors, a stepwise regression analysis was performed. As a selection criterion, a probability of F was between ≤0.100 and ≥0.200. Factors including age, gender, BMI, primary diagnosis, the Dorr types, CTI, CFI, and CCR were examined. Statistical analysis was performed using SPSS for Windows version 22 (IBM, Armonk, New York, USA). Each of the data was expressed as a mean ± standard deviation unless otherwise indicated. In all cases, p < 0.05 was considered significant.
Results
Analysis on the radiographs regarding the morphological type of the proximal femur among the 149 hips showed that there were 33 (22.1%) Dorr type A femurs, 110 (73.8%) type B, and 6 (4.0%) type C. The mean CTI, CFI, and CCR were 0.56 ± 0.08 (range 0.34–0.71), 4.15 ± 0.83 (range 2.50–7.14), and 0.46 ± 0.09 (range 0.26–0.75), respectively. The mean stem varus angle and stem anteversion were 0.19 ± 1.63 (range −8 to 9.6) and 17.7 ± 12.0° (range −13° to 46°), respectively (Table 2). The mean CTRI and CTRA were 40.8 ± 7.2° (range 21.8–63.7°) and 19.8 ± 6.6° (range −4.8° to 34.8°), respectively. The mean CA was 37.5 ± 14.5° (range −3.1° to 75.2°). For 92 cases of the 149 cases (61.7%), the CA was in the range of 25–50°, 10 whereas the implantation was done for 102 cases of the 149 (68.4%) cases in the Lewinnek safe zone 6 using CTRA and CTRI. To investigate relationships of CA with other factors, a stepwise regression analysis was performed. The stepwise selection process resulted in a model with age (p < 0.001; Table 4). In the same way, each of the factors increasing the stem anteversion and CTRA was analyzed. As a result, only for the stem anteversion, the stepwise selection process resulted in a model with age (p < 0.001) and the Dorr types (p = 0.047; Table 5).
Regression analysis for CA (stepwise method).

SE: standard error.
Regression analysis for stem anteversion (stepwise method).
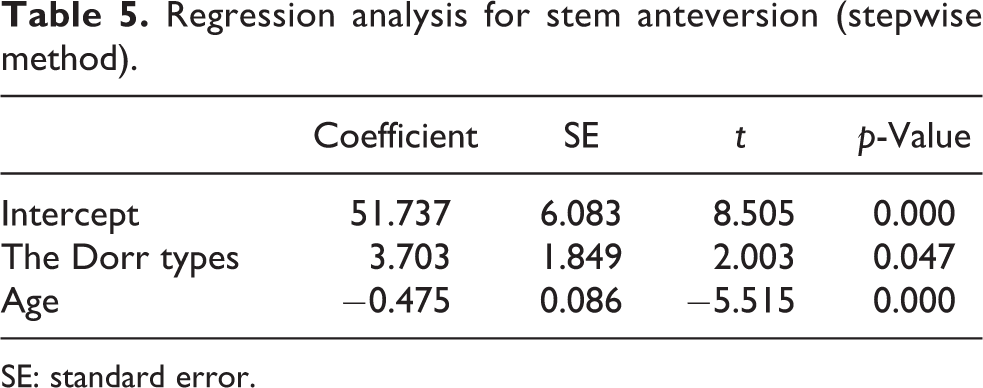
SE: standard error.
There was a case of intraoperative greater trochanter fracture during the releasing femur for elevation with a retractor, which was followed by a month’s delay to achieve full weight-bearing in physiotherapy. There were no postoperative complications such as calcar fracture, infection, and dislocation.
Discussion
DAA has attracted a great deal of interest because the preservation of muscle attachments to bone may improve hip stability. 1 Anterior approach was associated with lower rates of infection, dislocation, and reoperation. 3 Another advantage of DAA is that it makes the use of fluoroscopy during implant fixation easier. However, we cannot confirm stem anteversion by fluoroscopy.
Following primary THA, complications may occur as a result of incorrect positioning of the femoral stem, the acetabular cup, or both. It is known that acetabular malposition may lead to increased rates of dislocation, impingement, edge-loading, polyethylene wear, pelvic osteolysis, and prosthesis failure. Acetabular component positioning has been described as the most important factor in dictating risk of dislocation following THA. 11 It was reported that the incidence of THA dislocation is 1.5% when the acetabulum component is placed within a “safe zone” of 15 ± 10° anteversion and that of 40 ± 10° abduction, while the incidence is 6.1% when it is not placed within the ranges. 6 On the other hand, the “safe zone” for the movement avoiding the impingement and dislocation in THA predicted by the proposed parametric 3-D finite element model is 15–25° anteversion and 40–60° abduction. 12
There is purported improvement in component positioning and hip stability with the use of DAA-THA. Although fluoroscopic assistance seems to decrease complications such as femoral fracture by varus or flexed implantation of the stem, surgeons changing from PLA to DAA for THA should consider potential excessive cup anteversion and varus or flexed implantation of the stem in their early experience with DAA. 3 A common error in DAA-THA is to inadvertently insert the cup in too much anteversion. There is a tendency to hold the cup inserter too vertical, which imparts excessive anteversion to the component relative to the native pelvis. 5 Anteriorly unstable hips compared with stable hips had higher tilt-adjusted operative anteversion of the cup (40 ± 6° vs. 26 ± 10°; p < 0.001) and combined tilt-adjusted anteversion of the cup (64 ± 10° vs. 54 ± 19°; p = 0.028). 13
It is known that the native femoral anteversion cannot be used to predict the rotation of the femoral implant, so the operator cannot rely on a preoperative measurement even by CT scan in a straight, tapered cementless stem. 14 On the other hand, the postoperative femoral anteversion was not significantly different from the preoperative femoral anteversion in THA performed via an anterolateral approach with Orthopädische Chirurgie München using a straight stem and tapered-wedge stem. 15 Preoperative femoral anteversion has been reported to be a factor related to postoperative anteversion change. 16 Natural femoral anteversion of Japanese patients operated with THA (111 hips; OA: 105 hips, DDH: 76 hips) has been reported to be 23.9° ± 10.7°. 9 Natural femoral anteversion of Asians (Japanese: 22.1°, Thais: 22.7°) is known to be significantly larger than that of Caucasian (14.5°; p = 0.001). 17 It is difficult to verify stem anteversion even if intraoperative fluoroscopy was used. Postoperative stem anteversion is mainly influenced by the natural anteroposterior and mediolateral bow of the femoral canal, thickness of the posterior cortex, and width of the medullary canal. 18,19 The femoral component follows the flexion and twist of the proximal femoral channel to a so-called “best fitting” position. 14 Considering the result from this study, the operator has little control about the anteversion of the femoral stem in younger patients when using a tapered-wedge cementless stem. It is proposed to be started with the preparation of the femur followed by adjusting the position of the cup according to the increased femoral anteversion in younger patients.
CFI and CTI have been reported to decrease with age. 20,21 In our study, younger age was related to decreasing CCR. Higher CFI increases the risk of clinically detectable postoperative leg length discrepancy in single-wedge femoral stems with cementless metaphyseal fixation. 22 One of the concerns with high CFI femora is also the risk of femoral component undersizing due to potting of the stem distally in the narrow canal, particularly with tapered-wedge stems. 23 CTI and CFI were evaluated as morphological factors, and there was a related factor found for stem alignment in the sagittal and coronal planes between the size-matched stem group and the smaller stem group. 24 The CCR is a reflection of the geometric relationship of two points of the proximal femoral canal, which is also used as a morphological factor. A small ratio represents a funnel shape and a larger ratio, approaching 1.0, is a more cylindrical or stovepipe shape. Although there has been no guideline published that would advocate the routine clinical use of femoral CT, the Dorr types, CFI, CTI, CCR, and P20/D20 25 prior to THA, these should remain less complicated, faster, affordable, and less invasive techniques of femoral shape evaluation in the clinical setting. Worse Dorr proximal femoral types correlated with lower cortical thickness indices, 8,26 are found predominantly in older women with lower body weight. The Dorr types are simpler and easier to measure than CFI, CTI, and CCR.
The intraobserver and interobserver variability is a potential source of measurement errors in radiographic analyses. 27 To exclude the impact of this confounding factor, all radiographic measurements in the present study were performed by a single observer. A previous study reported that the intraclass correlation coefficient for absolute agreement between two independent observers was 92.1% for CFI. 27 It is reported that intrarater reliability in the determination of Dorr classification was 92%. 26
This study shows that patient age and the Dorr types are important parameters for increasing stem anteversion in planning short tapered-wedge stem with cementless metaphyseal fixation. The strengths of our study include the fact that to the best of our knowledge this is the first published study analyzing the factor for increasing acetabular cup anteversion and stem anteversion in DAA-THA using fluoroscopy. We were also able to evaluate the cup placement based on the Lewinnek safe zone and confirm there were no postoperative complications such as calcar fracture, infection, and dislocation. On the other hand, this study has several limitations. First, the natural femoral neck anteversion was not evaluated because this was a retrospective study where preoperative CT data were obtained from all the patients. Second, all the patients were Japanese, and the data may be unrepresentative of other ethnicities, as referred at natural anteversion of the femur. 9,17 Third, stem anteversion could be changed intentionally with the CA theory when the cup anteversion was increased or decreased. Despite these limitations, there have been no studies that have identified the factors related to stem anteversion in DAA-THA. We believe that this study can be potentially useful for younger age on stem anteversion and that it may be achieved by analyzing preoperating morphology of the femur.
Conclusion
The risk of excessive femoral anteversion increases for relatively younger age and for types of femoral morphology according to the Dorr classification, moreover with an increase of CA in DAA-THA with cementless tapered-wedge stem.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.