
Abstract
Purpose:
Despite the improvements in the repair equipment techniques of rotator cuff, a gold standard method has not been defined yet and transosseous fixation through deltoid-splitting (mini-open) approach is still regarded as a good option. The primary purpose of this study is to present satisfactory clinical and functional outcomes with a novel transosseous device in full-thickness rotator cuff tear through deltoid-splitting.
Materials and Methods:
This retrospective study was performed on 70 consecutive patients who underwent surgery by a single surgeon from June 2014 to June 2016 for a full-thickness rotator cuff tear and was managed with a novel transosseous device. Total number of patients, mean age, percentage of male and female patients, mean duration of follow-up, percentage of involvement of the dominant extremity, affected shoulder, and tear size were recorded. Functional and clinical outcomes were assessed baseline and postoperatively at 3 and 6 months and final follow-up using Disabilities of the Arm, Shoulder and Hand (Q-DASH) and Constant-Murley scores.
Results:
A total of 70 (49 (70%) female, 21 (30%) male) patients whose mean age was 58.66 ± 9.19 (38–77) years were included. The mean surgery time was 35.33 ± 5.34 (28–55) min. The mean follow-up time was 28.31 ± 3.03 (24–36) months. According to the DeOrio and Cofield classification, 15 (21.43%) tears were small, 33 (47.14%) medium, 16 (22.86%) large, and 6 (8.57%) massive. By the final follow-up, the mean Constant-Murley score had significantly improved from 27.67 ± 7.46 (13–41) to 81.25 ± 3.77 (74–87; p = 0.0001) and the Q-DASH score had decreased from 82.34 ± 10.37 (65.91–100) to 10.28 ± 6.88 (0–23.45; p = 0.0001). There were no significant differences in the Constant-Murley or Q-DASH score at baseline–final follow-up between the small, medium, large, and massive tear groups (p > 0.05).
Conclusions:
Treatment of full-thickness rotator cuff tear using this novel transosseous device significantly improved functional and clinical scores. However, further long-term prospective randomized multicenter trials involving comparative studies are necessary to confirm these findings.
Introduction
Rotator cuff repair involves surgical treatment of the shoulder and is successful in terms of patient satisfaction and pain regardless of the surgical approach and repair method used. 1 –4 The primary goals of rotator cuff repair can be listed as follows: to achieve high initial fixation strength, to reduce gap formation, to restore a wide footprint, to preserve mechanical stability under cyclic loading, and to optimize tendon–bone biologic healing. 5,6 Several studies have shown that, regardless of the surgical approach used (e.g., open repair, mini-open repair with a deltoid-splitting, and arthroscopic repair), transosseous techniques are able to obtain a better functional reconstruction and pain free compared to other methods for rotator cuff repair. 3,7,8 Therefore, there are several instrument options to perform transosseous technique like the bone needle, ArthroTunneler™, drill guide + 3 Kirshner (K)-wires, and anterior cruciate ligament (ACL) guide. 9 –11 Herein, a novel implantable transosseous device (Sharc-FT®, NCS Lab Srl, Modena, Italy) is used for rotator cuff surgery.
The primary purpose of this study is to present satisfactory clinical and functional outcomes with a novel transosseous device in full-thickness rotator cuff tear through deltoid-splitting.
Materials and methods
This retrospective study included 77 consecutive patients who underwent surgery by a single surgeon (MA) from June 2014 to June 2016 for a full-thickness rotator cuff tear and were managed with a novel transosseous device with deltoid-splitting. The study was performed in accordance with the guidelines for Declaration of Helsinki: ethical princıples for medical research involving human subjects and approved by the Noninvasive-Clinical Ethical Committee of the Medical School of Duzce University, Duzce, Turkey in 2018 (no. 2018/40) and written informed consent was obtained from all patients.
Patients who had a symptomatic rotator cuff tear confirmed by preoperative magnetic resonance imaging (MRI), with clinical and functional results at the final follow-up after the operation, and who underwent MRI after surgery at final follow-up were included. Patients with a subscapularis tendon injury, biceps tendon pathology, glenohumeral osteoarthritis, humeral head fracture and osteonecrosis, osteomyelitis, active infection, previous shoulder surgery, or Bankart pathology were excluded.
According to these criteria, seven patients were excluded due to patients with biceps tendon pathology (n:4) and previous shoulder surgery (n:3). A total of 70 patients were included in this study.
Demographic data, including the total number of patients, mean age, percentage of male and female patients, mean duration of follow-up, percentage of involvement of the dominant extremity, affected shoulder, and tear size, were recorded. The size of the rotator cuff tear was assessed during deltoid-splitting surgery and categorized according to the classification of DeOrio and Cofield, which was defined in terms of the percentage of small tears (<1 cm in length), medium tears (1–3 cm), large tears (3–5 cm), and massive tears (>5 cm). 12
Surgical technique
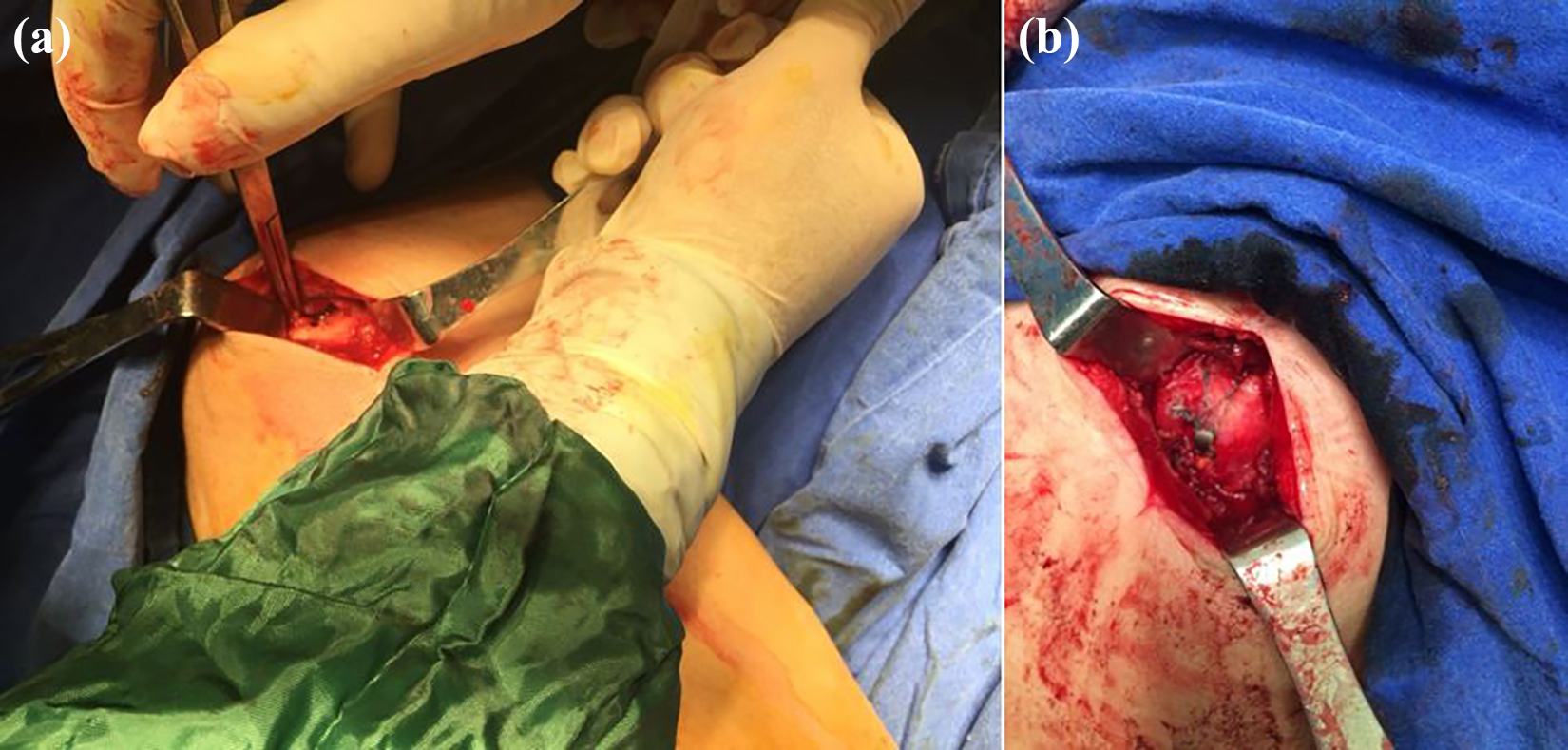
All surgeries were performed under general anesthesia in the beach chair position with a standard 3–4 cm lateral longitudinal incision beginning at the anterior border of the acromion (deltoid-splitting; Figure 1(a) and (b)). Subacromial decompression was performed in patients when necessary. After removing synovial tissues, present transosseous device system instrumentation (Figure 2) was applied as described by Pellegrini et al.. 13 First, the targeting needle was aligned with the longitudinal axis of the humerus to identify the correct lateral position of the Sharc-FT, and the punch instrument was used to place the entry hole at the lateral humeral cortex located 15–20 mm distally to the great tuberosity rim. Next, the distal end of the Taylor Stitcher was placed on the previously prepared hole and the right position of the super elastic transosseous needle was found. The super elastic transosseous needle was protruded 1 cm out over the footprint and captured the monofilament suture with a grasper before removing it from the bone. Depending on the tear size, different numbers of sutures and multiple holes near the footprint can be obtained. Next, the device was placed on the insertion tool using the retention suture, and high-resistance sutures were loaded onto the distal eyelet. The high-resistance suture limbs were tied to the corresponding monofilament suture shuttle and the sutures were pulled. The high-resistance sutures were pulled to allow the device to be positioned correctly at the prepared hole. All suture limbs were passed through the ruptured cuff and tied. Finally, the anterior limb of each high-resistance suture strand was tied with a retention suture and drawn through the proximal eyelet, and the anterior and posterior limbs were tied (Figure 3(a) and (b)). Figure 4 provides a summary of surgical technique for novel transosseous device (Sharc-FT).

(a) The skin marked for deltoid-splitting incision approximately 3 cm. (b) İntraoperatively, lateral longitudinal incision beginning at the anterior border of the acromion.

The implantable device (Sharc-FT) applied with punch, Taylor Stitcher with superelastic transosseous needle.
(a) A photograph with full-thickness rotator cuff rupture intraoperative period. (b) Full-thickness rotator cuff was repaired with novel transosseous device (Sharc-FT).

Flow diagram of surgical technique for novel transosseous device (Sharc-FT).
Rehabilitation protocol
All patients received postoperative therapy based on the same rehabilitation program after surgery. The affected arm was fixed with an abduction sling for 4 weeks at 45° abduction and neutral rotation for 4 weeks. Passive forward flexion, external rotation, and pendulum exercises were started only to the shoulder and elbow joints on postoperative day 3. At the end of week 4, the abduction sling was removed and active exercise was started (e.g., muscle strengthening program for the rotator and deltoid muscles).
Outcome measurements
Outcome measurement was performed by the surgeon (YT) who did not participate in the surgical procedures for the minimum bias. Functional and clinical outcomes of the affected shoulder were assessed baseline and postoperatively at 3 and 6 months and final follow-up using the Q-DASH and Constant-Murley scores. The Q-DASH is an abbreviated version of the original DASH outcome measure. In comparison to the original 30-item DASH outcome measure, the Q-DASH only contains 11 items. It is a questionnaire that measures an individual’s ability to complete tasks, absorb forces, and severity of symptoms. The Q-DASH tool uses a 5-point scale from which the patient can select an appropriate number corresponding to his/her severity and function level. Like the original version, the Q-DASH score ranges from 0 (no disability) to 100 (severest disability). Constant-Murley score is based on a scale of 100 points, with 35 points allocated for subjective variables (pain, activity of daily living, and functional use of the arm); 40 points, for objective measurements(range of motion); and maximum of 25 points, for the quantitative measurement of abduction. Abduction strength was measured with dynamometer with the shoulder in 90° of abduction.
Statistical analyses
Statistical analyses were performed using the Number Cruncher Statistical System 2007 Statistical Software (Kaysville, Utah, USA). Descriptive statistical methods (mean and standard deviation) and matched in-time comparisons of normally distributed variables were used. One-way analysis of variance (ANOVA) and Newman–Keuls multiple comparison test were used for subgroup comparisons. One-way ANOVA was used to compare groups, and the χ 2 test was used to compare qualitative data. The level of significance was set at p < 0.05.
Results
A total of 70 (49 (70%) female, 21 (30%) male) patients whose mean age was 58.66 ± 9.19 (38–77) years were included. The mean surgery time was 35.33 ± 5.34 (28–55) min. The right shoulder was operated on in 52 (74.29%) patients and the left shoulder was operated on in 18 (25.71%) patients. Surgery was performed on the dominant extremity in 52 patients and on the nondominant extremity in 18. The mean follow-up time was 28.31 ± 3.03 (24–36) months (small: 27.67 ± 2.19; medium: 28.12 ± 2.98; large: 29.31 ± 3.32; massive: 28.33 ± 4.32). According to the DeOrio and Cofield classification, 15 (21.43%) tears were small (<1 cm in length), 33 (47.14%) were medium (1–3 cm), 16 (22.86%) were large (3–5 cm), and 6 (8.57%) were massive (>5 cm). By the final follow-up, the mean Constant-Murley score had significantly improved from 27.67 ± 7.46 (13–41) to 81.25 ± 3.77 (74–87; p = 0.0001) and the Q-DASH score had decreased from 82.34 ± 10.37 (65.91–100) to 10.28 ± 6.88 (0–23.45; p = 0.0001). There were no significant differences in the mean Q-DASH or Constant-Murley score or in age or mean Constant-Murley or Q-DASH score at any time point (p > 0.05). There were no significant differences in the mean Constant-Murley or Q-DASH score between females and males, and no differences in the mean age, sex, surgery side, dominant operation side distribution, surgery time, or follow-up time (Table 1) or between the tear size groups (p > 0.05; Table 2 and Figure 5(a) and (b)). There were no reported complications both intraoperatively and during the postoperative time period such as stiffness, implant failure, infection, deltoid muscle problems, re-tears, fracture, or nerve injury.
Summary of patient demographics and clinical characteristics at baseline between small, medium, large, and massive tear groups.

SD: standard deviation.
aOne-way analysis of variance.
b χ 2 test.
Basline, 3rd months, 6th months, and final follow-up mean Constant-Murley–Q-DASH score between small, medium, large, and massive rotator cuff tear groups.

Q-DASH: Quick-The Disabilities of the Arm, Shoulder and Hand Score; SD: standard deviation.
aOne-way analysis of variance
b Matched one-way variance analysis, (mean ± SD).

Baseline, 3rd months, 6th months, and final follow-up mean Constant-Murley–Q-DASH score. Q-DASH: Disabilities of the Arm, Shoulder and Hand.
Discussion
Transosseous repair techniques are accepted as superior methods of rotator cuff repair regardless of the surgical approach (e.g. open repair, mini-open repair with a deltoid-splitting, and arthroscopic repair). 3,7,8 In addition, an open or deltoid-splitting (mini-open) repair with transosseous fixation is noted as a good choice currently. 14,15 The present study demonstrated that deltoid-splitting repair of a full-thickness rotator cuff tear with this novel transosseous device was associated with good clinical outcomes and good structural integrity, similar to the traditional transosseous technique. In addition, compared to other conventional transosseous techniques, the main advantages of this new device are that it provides wide footprint reconstruction, preserves lateral cortical rupture, and avoids impingement with the acromion. 6,13 Additionally, various transosseous repair devices have been published in the literature recently for the management of full-thickness rotator cuff tears like the bone needle, ArthroTunneler®, drill guide+ 3 K-wires, and ACL guide. 9 –11 However, all of these techniques are complicated and require several steps. In the current study, we used a novel transosseous device supplied with three additional and complementary tools: an inserter, a punch, and a multipurpose tool for fitting/removing the super elastic transosseous needle. 8,13 The punch instead allows a hole to be made where placing the transosseous device. In addition, the super elastic transosseous needle allows for the creation of one or more transosseous tunnels in the lateral entry hole in which the device is entered and one or more medial exit holes adjacent to the footprint field. All in all, this novel device enables one to perform transosseous repair with a dedicated instrument. 13 Different from other transosseous methods, this present transosseous device has a holed body intended to manage one to four (or more) inner sutures, and its shape was created to maximize the resistance to pull out effect and to prohibit suture–bone interaction. The head preserves superior stability to the system due to the external sutures that achieve a force equilibrium. Furthermore, the device behaves as a bridge, improving the way suture impact over bone. 6,8,13
Several studies have shown that the transosseous technique produces good to excellent clinical outcomes with superior biomechanical properties at the short- to long-term follow-up. 3,4,16,17 Park et al. evaluated the self-reinforcement effect after transosseous versus single-row rotator cuff repair. The authors compared 10 fresh-frozen human shoulders that underwent transosseous repair to 10 that underwent single-row cuff repair. They concluded that transosseous repair had a higher footprint contact force, area, pressure, and peak pressure at each load for both abduction angles and that this self-enforcing effect helped sustain structural integrity and may have improved healing biology. 18 Another study compared transosseous and double-row repairs in a cadaveric model and found that the transosseous-equivalent rotator cuff repair technique improved ultimate failure loads compared to the double-row technique and that gap formation was similar. 19 Transosseous-equivalent repair helps restore footprint dimensions and provides stronger repair than the double-row technique, which may optimize healing biology. 19 In a biomechanical study on the new transosseous system, Mantovani et al. reported that novel transosseous device (Sharc-FT) provides transosseous sutures with cortical fixation, creates a traction-compression lateral suture inside the footprint, greatly reduces the problems of poor bone resistance, decreases motion at the tendon–footprint interface, improves fatigue resistance, and makes the stress load distribution at the footprint homogeneous, therefore optimizing biological healing. 6 Another study on arthroscopic techniques using this device to describe the arthroscopic rotator cuff tear transosseous repair system reported encouraging outcomes, confirming its efficacy. The authors concluded that the patient satisfaction rate was high, no patients expressed concern about the implant, and the complication rate was very low. 13 In the present study, despite the relatively short follow-up time, our outcomes are concordant with previous reports, and no bone cutting phenomena, impingement with the acromion, or implant failure was noted with this new device. The mean clinical and functional outcomes 16.8 months after surgery showed significant improvements in the Q-DASH and Constant-Murley scores compared to the preoperative status (p < 0.05).
Recently, with the help of increased blood flow due to bone tunnels and microfractures on the footprint which stimulate bone marrow mesenchymal stem cells and growth factors, the biologic healing process of the repaired rotator cuff can be induced. 20 –24 Bilsel et al. used a rabbit model and concluded that a microfracture on the tuberosity of a repaired cuff stimulated tendon healing, with increased ultimate force to failure and with thicker collagen bundles and more fibrocartilage. 20 Taniguchi et al. 21 showed that bone marrow stimulated by multiple bone tunnels in the footprint increased the integrity of the repaired cuff, consistent with other studies. 22 –24 In the present work, there was no re-tear cuff detected by MRI, which was performed on all patients postoperatively at final follow-up. When we applied the novel transosseous device, the super elastic transosseous needle allowed for the creation of one or more holes depending on the tear size on the footprint. Therefore, we agree that one or more bone tunnels through the footprint can increase cuff integrity and biologic healing by increasing blood flow and stimulating bone marrow mesenchymal stem cells and growth factors.
There is only one clinical study in the English literature on novel transosseous device. Thirty-four patients who underwent arthroscopic surgery with this novel transosseous system to repair the supraspinatus and infraspinatus reported favorable structural results. In that study, the mean Constant-Murley score improved from 24.5 preoperatively to 86.9 at a mean follow-up duration of 18.6 months, and only two cases of adhesive capsulitis were recorded. 8 To the best of our knowledge, the present work is the first clinical application of this novel transosseous device on deltoid-splitting rotator cuff repairs. We evaluated 70 patients who underwent this novel transosseous suture repair of a full-thickness rotator cuff tear with the deltoid-splitting approach. The preoperative mean Constant-Murley score improved from 27.61 ± 7.44 (13–41) to 81.26 ± 3.76 (74–87) at the final follow-up (p = 0.0001), and the mean Q-DASH score decreased from 82.34 ± 10.37 (65.91–100) to 10.28 ± 6.88 (0–23.45; p = 0.0001).
According to Gerber et al., an ideal rotator cuff repair should ensure high initial fixation strength and minimize gap formation while healing. 5 Mantovani et al. compared the traditional transosseous technique with two high-resistance sutures and novel transosseous device. This study showed that novel transosseous device helps avoid direct impingement, mitigates contact pressure, and reduces the risk for local bone damage. They concluded that the traditional transosseous method by itself making use of high strength sutures leads to a significant increase in gap formation in a dynamic test than novel transosseous device. Also, the experimental evidence of study was that by avoiding a direct impingement, they significantly reduce the gap formation during the test of this present transosseous device. 6 In our experience with this device, we restored a wide footprint and minimized gap formation, and there were no symptoms of impingement in our patients after surgery at a mean follow-up of 28.31 ± 3.03 (24–36) months.
Rotator cuff surgery techniques continue to develop but the complications of repair have not been solved totally. 25 –29 Suture anchor fixation is frequently used although it causes complications such as arthritis, pullout, and osteolysis. 28,29 Also, there are other problems with the anchor usage in rotator cuff repair. For example, in the cases of re-tear, sometimes the revision surgery becomes difficult because the previous anchors are difficult to remove, thereby remaining limited area for new anchor placement. 10 Herein, one of the primary device (Sharc-FT) property refers to its placement in area with a good bone quality, located about 15/20 mm distally to the great tuberosity rim. This capability allow to obtain a significant decrease in the possibility of repairing failure due to suture bone cut effect. 8,13 In addition to all these, the cost of multiple anchors is high and anchor dislodgement, osteolysis of the greater tuberosity, and impingement of the anchor in abduction of the shoulder joint could occur. 26 On the other hand, the restrictive aspect of conventional transosseous repair is the risk of tearing the cortical part of the lateral border of the tunnel. 30,31 In our first clinical study on this new transosseous device with deltoid-splitting rotator cuff repair, there were no complications such as re-tear, rupture of the lateral cortex, or impingement affecting small, medium, large, or massive tears.
Most studies have shown that rotator cuff repair infection rates range from 0.27% to 1.9% using mini-open and open techniques 32,33 and from 0.04% to 0.23% using arthroscopic techniques. 34,35 In a recent level IV study, Asaid et al. retrospectively evaluated 764 patients who underwent mini-open repair; the incidence of infection was 1.2% at a mean follow-up duration of 11.62 years after surgery. 36 These data were not confirmed by our study in which there were no reported perioperative or postoperative infections.
Finally, there were a few limitations to our study. First, it was retrospective and examined relatively short-term outcomes after surgery. In addition, the number of patients was relatively small. Furthermore, despite the relatively low incidence of complications associated with rotator cuff repair in our study, a longer follow-up may lead to higher complication rates. In addition, there was no comparative group of patients repaired with a different technique, such as the traditional transosseous technique.
Conclusions
In spite of the improvements in the repair techniques of rotator cuff, a gold standard method has not been defined yet and transosseous fixation through a deltoid-splitting (mini-open) approach is still regarded as a good option. This developable device is one of the most anticipated techniques because of the possibility to recreate the footprint anatomy, avoid impingement with the acromion, and preserve the lateral cortical rupture; it is particularly useful for revision surgery. This is the first clinical study on deltoid-splitting rotator cuff repair with this novel transosseous device in which satisfactory clinical and functional outcomes were reported. However, further long-term prospective randomized trials involving comparative studies are necessary to confirm these findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.