
Abstract
Introduction:
Acromioclavicular joint injuries are common shoulder girdle injuries most commonly resulting from a direct blow to the acromion with the arm adducted. Type-I or type-II acromioclavicular joint injuries can be managed with sling immobilization, early shoulder motion, and physiotherapy. The management of type-III injuries remains controversial and is individualized. Type IV and V injuries should be treated surgically. A myriad of surgical techniques for the management of acromioclavicular joint injuries have been reported.
Methods:
We present a comparative study of 76 patients treated with two most common modalities of treatment for AC joint disruption and that is Hook plate stabilisation (n=52) or arthroscopically assisted tight rope stabilisation (n=24). The primary objective was to establish whether hook plate stabilization was superior compared to arthroscopic tight rope fixation in reducing pain and increasing function in the short-term and long-term for patients with AC joint disruptions III-IV. We also wanted to assess how quickly patients returned to their work/job. It was a prospective study, we included all the patients operated between 2008 and 2015 for AC joint disruption by the two shoulder surgeons of our department. All patients followed a strict physiotherapy protocol and were assessed at 6 weeks, 3 months and 12 months. We used the Harm and cost criteria of assessment and the patient specific functional outcome scores.
Results:
Both modalities of treatment have high patient satisfaction rate, return to work is faster in tight rope group but after a year both group of patients returned to their premorbid state. Removal of hook plate is not mandatory and lysis of acromion is rare (1% in our series).
Conclusion:
Despite the fact that both methods yielded similar results and have statistically similar number of complications, the type of postoperative complications was different between groups. The plate group had more postoperative pain and worse function but both aspects improved after plate removal. The rope group had more complex complications including deep infection and recurrence of deformity and fracture. These differences should be taken into consideration when consenting the patient regarding possible treatment.
Introduction
Acromioclavicular (AC) joint injuries are common shoulder girdle injuries mostly resulting from a direct blow to the acromion with the arm adducted. Type I or type II AC joint injuries can be managed with sling immobilization, early shoulder motion and physiotherapy. Based on these approach, it has been reported that for type I injuries the mean period of immobilization was 19.5 days, and functional outcomes using the mean constant shoulder rating score was 94 points, indicating an excellent functional outcome. 1
The management of type III injuries remains controversial and is individualized. Although some studies suggest a return to previous level of functional activity with nonsurgical treatment, surgical treatment and coracoclavicular ligament reconstruction have been associated with a favourable outcome, 2,3 with a place in the management of patients with high functional demands especially athletes participating in overhead sports.
Three randomized prospective trials 2,4,5 and few nonrandomized studies 6 –8,22 have directly compared nonsurgical versus surgical intervention outcomes in the management of type III AC separations. None of the studies show surgical management is better except arguably in some cases of high-performing athletes.
Surgical management is indicated for high-grade (≥ type IV) AC joint injuries to achieve anatomic reduction in the AC joint, reconstruction of the coracoclavicular ligaments and repair of the deltotrapezial fascia.
Surgical reconstruction led to satisfactory clinical outcomes, 9,10 with regard to pain relief and return to functional activities, but biomechanical strength of these constructs that are necessary to avoid loss of reduction and creep with cyclic loading are yet to be evaluated.
A myriad of surgical techniques have been reported for the management of AC joint injuries. With recent advancements in instrumentation and arthroscopic techniques, there has been an increased use of arthroscopically assisted or all-arthroscopic reconstruction of the coracoclavicular ligament with graft or synthetic material. There is very little to choose between these different modalities of treatment. The open hook plate method and arthroscopic tight rope fixation with augmentation are considered to be preferable to other techniques because they are used most commonly, with predictable outcomes and which has also got reasonable support in the literature. 10 –12 Besides all these, the learning curve is not very steep especially in the hook plate fixation.
Methods
Design and setting
A prospective study, comparing the efficacy of the hook plate stabilization technique (hook group, n = 52) with arthroscopic tight rope fixation procedure (rope group, n = 24). The study was conducted over a period of 9 years from 2008 to 2015, at one hospital site located in the West Midlands at an NHS Foundation Trust. Eligible participants were adults aged between 18 and 65 years, who had reported direct trauma to their shoulder.
Patients were randomly allocated to either one of the surgeons by the accident and emergency department. Patients were booked into shoulder trauma clinics, depending on availability. This resulted in unequal number between groups. Simple randomization was preferred in order to reduce selection bias and ease study planning. AC disruption was diagnosed from X-ray and categorized using the Rockwood classification type II, type III, type IV in either the emergency or the orthopaedic departments. Follow-up periods were 6 weeks, 3 months and 1 year post-operatively. During this period, patients would have already started a physiotherapy protocol (Table 1). Remaining follow-ups were at 3 monthly intervals up to a maximum of 48 months post-surgery, for a final review.
Physiotherapy protocol.
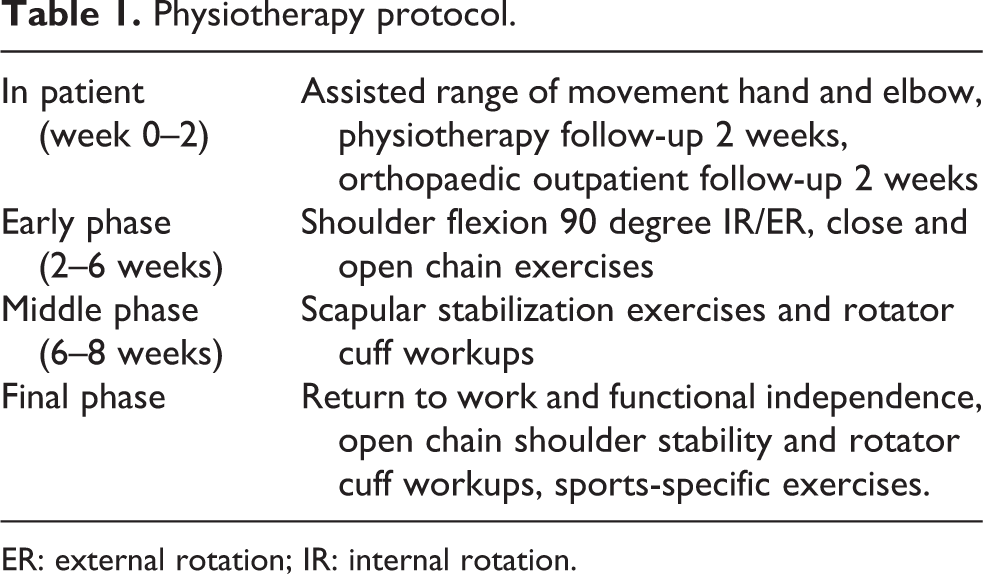
ER: external rotation; IR: internal rotation.
Outcome measures
Post-surgical measures included measures on function, harm and cost and also patient-specific functional score (function).
Harm
Levels of harm were categorized based on the Common Terminology Criteria for Adverse Events: mild, moderate or severe 28 . Harm was expressed as the number (and percentage) of participants who had reported harm associated with an intervention.
Cost
Surgical utilization cost and follow-up cost were expressed as the mean number of orthopaedic and physiotherapy appointments needed per group and calculated in terms of mean monetary value of unit costs for time.
Statistical methods
Harm was expressed as a number (and percentage) of participants who reported harm with an intervention. All tests were conducted using a significance level of 5%, and results were analysed with caution since no adjustment was made for multiple testing. Percentages were compared using the z score test for two population proportions. All statistical analyses were completed using SPSS (IMB SPSS Statistics Ver. 20).
Results
This study identified a total of 76 patients who had AC disruption II–IV and had undergone surgery. Fifty-two patients underwent hook plate stabilization and 24 were treated with tight rope technique. According to baseline demographic data, participants in the two groups had similar characteristics.
Average time to surgery was 34 days (3–90 days). There was no difference in the average waiting time in two groups.
Demographic characteristics of randomized participants, at baseline (n = 76).

n: number of participants; AC: acromioclavicular.
Harm
During the course of the intervention period, neither intervention led directly to any severe harm. Both the groups showed a similarity in moderate harm (z score, p = 0.1298), 20 (37%) patients in the hook group required revision surgery to remove the plate compared to only 5 (17%) in the rope group, who required further intervention. Removal of the hook plate is part of a staged procedure which is performed at an average of 6.8 (3–14) months.
Complications were more common in the rope group (13 patients, 52%) compared to the hook group (17 patients, 33%), but they were statistically similar (z score, p = 0.07). From the hook plate group, 15 patients who had mobility issues following the hook procedure showed further improvement following plate removal. Two patients underwent surgical revision because of loss of fixation but the plate did not have enough cortical purchase medially and hence were considered technical failures.
Two patients from the rope group had hardware sensitivity and six patients had recurrent deformity. Two patients who had recurrence required revision to a hook plate, one due to fracture and one due to deep infection.
Two patients from the hook group and one from the tight rope developed erosion of the acromion, and this condition was similar between groups (p = 0.944). Minor harm including superficial infection in 8% of the hook group and 4% of the rope group was reported, and this was similar between groups (z score, p = 0.234)
Function
Pain and range of movement were significantly affected in seven patients, Three hook plate and four tight rope, at the time of last review. No statistical difference between groups was identified (z score, p = 0.126). Of the 76 patients, 10 had a poor outcome at the time of their last review due to either reduction in function or the overall satisfaction with the process and outcome. With regard to management, 4 patients from the tight rope and 6 patients from the hook plate fixation were not satisfied, and satisfaction was similar between groups (z score, p = 0.038).
Cost
Cost was assessed by the need for second procedure and total time of work, time required to return to activities . The dominant hand was affected in 34 patients of the hook group, with time off from work totalling to 8.9 (1–23) weeks, of the 37 that were in employment. In 30 cases, 6.2 (1–18) weeks at the first operation and 3.3 (1–6.7) weeks at the second procedure. Of these patients, 10 were overhead manual labourers who required 5–6.7 weeks to return to work, and the rest were able to return to less active jobs within 1–4 weeks. All office workers (n = 9) were able to return to work within 2 weeks.
The dominant hand was affected in 14 patients of the rope group, with time off from work totalling to 6.2 (1–15) weeks, of the 22 that were in employment, though 7 required to undergo unplanned surgery, necessitating 3.4 (1–6) weeks away from work; 2 for revision to hook plate, 2 for removal of hardware causing sensitivity and 3 for superficial skin infection. Of the 76 patients, 63 (35%) were discharged from the clinic after an average of 20 months, with no ongoing issues.
Discussion
The surgical management of high-grade AC joint injuries seems to be the most favourable modality of treatment for shoulder surgeons of current time, which is approved by the validated data obtained from many studies. This holds good particularly for the cases with type III to VI AC joint injuries. Our study also conforms with other studies (8). 11,13 The successful outcome with surgical management of AC joint injuries depends on anatomic and accurate reduction in the AC joint to correct displacement and translation. Some studies suggest a direct repair (in patients with acute injury) or reconstruction (in patients with chronic injury) of the coracoclavicular ligament results in better outcome, this was the case in our study where patients were treated with tight rope fixation . A recent study by Natera et al. also suggests that there are no significant differences between acute and chronic repair of AC joint dislocations if all other aspects of treatment are similar. 14
In our study, the outcome from both modalities of treatment, that is, tight rope or hook plate fixation, does not show statistically significant differences. 15 Helfen et al. reviewed 921 studies, which included 32 review papers, and reported similar results. 16 This was similar to the comparative study by Yoon et al. 17 Another review by Arirachakaran et al. 18 identified 41 studies reporting results from both methods but not directly comparing them. They report lower complication rates but worse function scores and higher postoperative pain in the patients treated with hook plate. In our study, there were no statistically significant differences in the number of complications between groups but the type of postoperative complication was different between groups. This was similar to the review paper by Arirachakaran et al., 18 where the hook plate group had more postoperative pain and worse function but both the aspects improved after plate removal. The rope group had more complex complications including deep infection and recurrence of deformity and fracture. Another recent comparative study showed similar results regarding the increased incidence of recurrence following rope fixation and more erosions after hook fixation. 17 These differences should be taken into consideration when consenting the patient regarding possible treatment. Plate removal is another issue that needs to be discussed, as it adds a second procedure. Post-operative pain is an indication to remove the plate, that is, if it is painful, then plate removal can be performed before 3 months, and if it is not painful but the function is impaired, then removal can be delayed beyond 3 months. 18 If there is no pain or function impairment, then the hook plate can be left in situ. In our series of 52 patients, the plate was removed in 20 patients and left it in situ in the rest, with only 1 (3%) developing signs of erosion of the acromion.
Supplementation or protection of the coracoclavicular ligament repair or reconstruction with synthetic material (suture or tape) or a rigid implant to maintain AC joint stability during the acute phases of healing improves outcome as shown in many studies, 19,20,27 as was the case in our study as well. Repair of the deltoid and trapezial fascia and distal clavicular resection in patients with chronic AC injuries with radiographic or clinical evidence of AC osteoarthritis improves the outcome as reported in some studies; however, this was not done regularly hence difficult to compare. Few patients who underwent the repair and resection had favourable outcome.
Simple randomization was preferred to reduce bias and ease the planning of the study. Randomization was based on random assignment to surgeon by the booking team. Then, choice of treatment was the result of surgeon preference and skills. This resulted in unequal number of patients treated between the two groups. Power analysis with effect size of 0.71 calculated a 1 − β error probability of 0.81 (G*Power 3.0.10).
Conclusion
In summary, there is currently a lack of studies with a high level of evidence evaluating nonsurgical and surgical management of type III AC joint injuries. The three prospective randomized studies are over 20 years old and involve surgical fixation methods that are not currently utilized. We conclude that surgical fixation allows quicker return to work and early pain relief. Patients with tight rope group returned to work quickly by 3.2 days on average (p = 0.004), but no significant differences were observed between the two groups. This is similar to a recent study by Yoon et al. 17
Numerous surgical techniques have been described in the treatment of type III to type V AC joint injuries, but no one technique has been shown to be clinically superior to another (9), 20,13 which was the conclusion in this study as well. The patient satisfaction rate was high in both groups and they are not statistically significant. We think patient satisfaction was quite high in the hook plate group not because their functional outcome was superior but because the expectations of those in hook plate group were met well. Not all patients wanted plate removal. this study does not answer as to how it will affect the osteolysis of acromion, but no adverse effects were noted up to the point of last follow-up.
Despite the fact that both methods yielded similar results, as it has been reported in the recent literature, 17 –21 and have statistically similar number of complications, the type of postoperative complications was different between groups. As noted before, the plate group had more postoperative pain and worse function but both aspects improved after plate removal. The rope group had more complex complications including deep infection and recurrence of deformity and fracture. These differences should be taken into consideration when consenting the patient regarding possible treatment.
Footnotes
Author’s Note
All authors have made substantial contributions to the conception and design of the study or acquisition of data analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; the final approval of the version to be submitted. The authors did not have any writing assistance, did not have any source of payment or funding for this paper, and did not have any study sponsors; and this manuscript, including related data and tables, has not been published previously and is not under consideration for publication elsewhere.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.