
Abstract
Background:
Gunshot injury of the hip joint was reported to constitute 2–17% of all extremity firearm injuries. However, there are few studies in the literature related to gunshot injuries of the hip joint. The aim of the current study was to present the results of 10 cases treated with arthroplasty following a gunshot injury to the hip joint together with the recommended treatment algorithm.
Methods:
Patients with a previous medical history of hip joint region gunshot injury who underwent total hip arthroplasty were retrospectively evaluated. Those with incomplete medical records or who were lost to follow-up were excluded. Patients were classified according to the severity of the previous gunshot injury to the hip joint region. Harris hip score (HHS) and Short Form-12 quality of life score were the main outcome measurements. Postoperative complications encountered during follow-up were recorded.
Results:
The mean age of the patients at the time of surgery was 29.9 years. The mean preoperative HHS was 25.2 points and it was 65.8 at the final follow-up. Patients with bullet fragments in the hip joint, classified as group 1, had better HHS, whereas those with contaminated hip joint with intestinal flora, classified as group 3, had worst HHS.
Conclusion:
Hip arthroplasty after hip joint gunshot injury is a good treatment choice in young patients to reduce pain and regain functions. However, very high infection rates can be seen in patients with accompanying intestinal injury.
Introduction
In recent years, there has been an increase in gunshot injuries, which present great problems for orthopaedic surgeons. 1 It is important that orthopaedic surgeons are aware of these injuries and the appropriate treatments. In the literature, gunshot injury of the hip joint was reported to constitute 2–17% of all extremity firearm injuries. 2 However, there are few studies in the literature related to gunshot injuries of the hip joint, and some of these publications are decades old. 3,4
Great care must be taken in the treatment of gunshot injuries in this region because of the proximity of intra- and extra-pelvic anatomic structures. Follow-up of the treatment for gunshot injuries in the hip joint is difficult because of the high-mortality rate and the development of morbidity. In addition to the high costs of treatment, this difficulty creates concomitant nerve damage and contamination of the hip joint following visceral organ damage. 5 The risks of lead intoxication and fibrotic scar tissue developing as a result of soft tissue damage also make treatment more difficult. 6
In the scarce literature, the treatment algorithm recommended following gunshot injury to the joint is limited to arthroplasty. 7 The current study is one of the reports in the literature on this subject including the most extensive and youngest group of patients. The hypothesis of this study was that possible complications could be predicted by classification according to the severity of the injury in patients undergoing total hip arthroplasty following a gunshot injury to the hip region. Therefore, the aim of the study was to present the results of 10 cases treated with arthroplasty following a gunshot injury to the hip joint together with the recommended treatment algorithm.
Patients and method
Approval for this retrospective study was granted by the Institutional Ethics Review Board. Informed consent was obtained from each patient. The patients included were those with a previous medical history of hip joint region gunshot injury who underwent total hip arthroplasty at a single centre. Those with incomplete medical records or who were lost to follow-up were excluded. For each patient, a record was made of age, gender, body mass index (BMI) and previous medical history. Previous interventions performed at the same centre of first admission after gunshot injury of the hip joint were also recorded for all patients.
Surgical technique
Patients with traumatic osteoarthritis and/or incongruent and damaged hip joint due to gunshot injury and with no sign of infection were treated with primary total hip arthroplasty. All patients were operated on at a single centre by the same senior surgeon (OP) through the posterolateral approach. Intra-articular bullet fragments were extracted during surgery, and femoral shortening osteotomy was performed in patients with trochanter major superior displacement. Cement-less femoral and acetabular components were used for the total hip arthroplasty procedure (M/L Taper Hip Prothesis and Wagner SL Revision Hip System, Zimmer Biomet, Warsaw, Indiana, USA). No grafts or augmentations were used for any of the patients.
Prophylaxis of cefazolin was administered to all patients and was continued for 3 days postoperatively. Low-molecular-weight heparin was administered for 4 weeks. All patients were mobilized on postoperative day 1 and full weight-bearing was permitted. All the patients were discharged at mean 3–5 days postoperatively.
All patients were called for follow-up visits in the postoperative 2nd week, 6th week, 3rd month, 6th month, 12th month and annually thereafter. Pelvis anteroposterior and lateral radiographs were taken at each follow-up examination. In patients with intra-articular bullet fragments, attention was paid to lead toxicity. Postoperative complications encountered during follow-up were recorded. Minimum postoperative follow-up time was set as 2 years.
Throughout the follow-up period, the patients were evaluated in respect to complications that are frequently seen such as aseptic loosening in the hip prosthesis, infection (deep periprosthetic or superficial wound infection), deep vein thrombosis, pulmonary embolism, limb length discrepancy, dislocation and hematoma. The patient clinical scores were evaluated using the Harris hip score (HHS) and Short Form-12 (SF-12) quality of life, in both its physical and mental components, preoperatively and at the final follow-up examination. HHS < 70 points was considered poor function, while HHS of 70–79 was evaluated as fair, 80–89 as good and >90 as excellent.
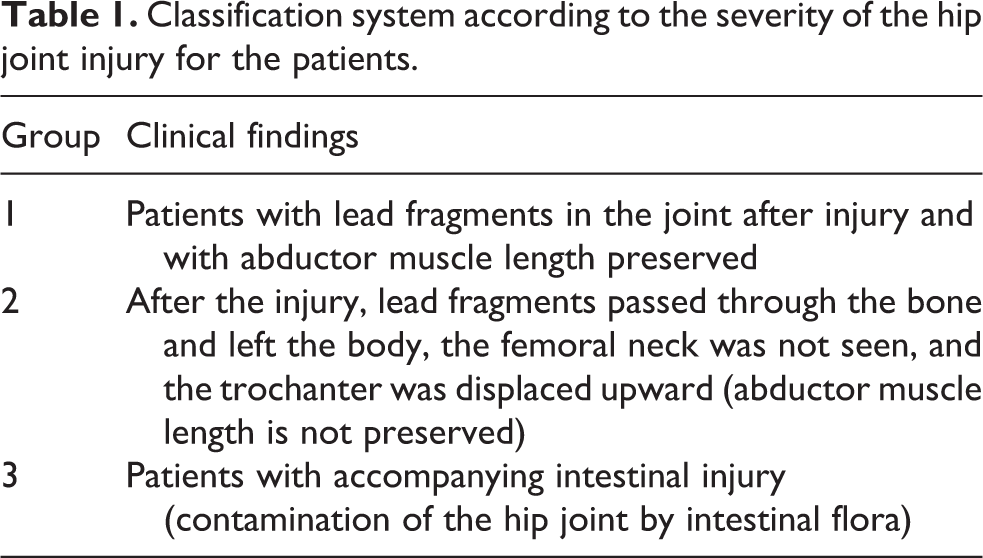
Patients were classified according to the severity of the previous gunshot injury to the hip joint region. An abductor mechanism injury was classified as a more severe injury compared to group I injuries which consisted of intra-articular bullet fragments without disruption of the abductor mechanism. The disruption of the abductor mechanism was due to the displaced trochanteric fracture. Patients in this group had limping because of abductor weakness. Patients with contaminated hip joint injuries were classified as group III. In group III injuries, the abdominal injury was extended to the ipsilateral pelvic wall and contaminated the hip joint. The classification of the patients according to the severity of the hip joint injury is shown in Table 1.
Classification system according to the severity of the hip joint injury for the patients.
Results
The demographic data of the patients, previous interventions for hip joint injury before total hip arthroplasty, classification of the gunshot injury, HHS and SF-12 scores are presented in Table 2. The average time from injury to surgery was 4.9 ± 1.4 months (range 3–8 months). The mean age of the patients at the time of surgery was 29.9 ± 10.0 years (range 18–45 years). The mean BMI of the patients was 24.7 ± 3.1 kg/m2 (range 18.9–29 kg/m2). The mean preoperative HHS was 25.2 ± 8.7 points (range 13–37 points) and it was 65.8 ± 16.5 points (range 38–87 points) at the final follow-up examination. The mean preoperative physical component of SF-12 was 26.0 ± 1.9 points (range 23.3–30.2 points) and it was 38.7 ± 2.3 points (range 35.3–43.0 points) at the final follow-up examination. The mean preoperative mental component of SF-12 was 32.8 ± 3.9 points (range 25.0–37.4 points) and it was 36.5 ± 2.4 points (range 32.2–40.5 points) at the final follow-up examination. The HHS and SF-12 scores of the patients according to the groups are shown in Table 3.
Patient demographics, classification of the gunshot injury, HHS and SF-12 scores.

BMI: body mass index; HHS: Harris hip score; SF-12: short form 12.
HHS and SF-12 scores of the patients according to the groups.

n: number; HHS: Harris hip score; SF-12: short form 12.
It was observed that rapid traumatic osteoarthritis was more likely to develop in patients with intra-articular bullet fragments and synovitis observed in the hip joints during surgery (Figure 1). No evidence of lead toxicity was detected in any of the patients during postoperative 2-year follow-up. Femoral shortening osteotomy was performed in patients with trochanter major superior displacement (group II; Figure 2). None of the patients had any signs of preoperative infection. However, postoperative infection developed in all two patients with accompanying intestinal injury (group III; Figure 3). One of these patients was treated with debridement, whereas the other patient could not be treated with debridement and the patient refused any additional treatment.

(a) A 23-year-old male patient with a bullet fragment in the hip joint after gunshot injury who was classified as group 1. (b) Five months after the injury and initial surgical wound debridement, patient underwent cement-less total hip arthroplasty (M/L Taper Hip Prothesis, Zimmer Biomet).

(a) A 27-year-old male patient with a previous history of failed internal fixation and shortened abductor length after gunshot injury, who was classified as group 2. (b) Five months after the injury, patient underwent femoral shortening osteotomy and cement-less total hip arthroplasty (Wagner SL Revision Hip System, Zimmer Biomet).

(a) A 23-year-old male patient with a previous history of colostomy and contaminated hip joint after gunshot injury, who was classified as group 3. (b) Five months after the injury, patient underwent cement-less total hip arthroplasty (Wagner SL Revision Hip System, Zimmer Biomet).
Discussion
Gunshot injuries to the hip joint region constitute 2% of all extremity gunshot injuries. After a hip joint gunshot injury, open reduction and internal fixation are recommended for fracture treatment. 8 In the acute period, arthrodesis or arthroplasty is not recommended. In the period after injury, arthroplasty is a treatment choice for arthrosis or unsuccessful internal fixation. 8 In the current study, hip arthroplasty was performed on 10 young adult patients in the chronic period after hip joint gunshot injury. The most important finding of this study was that patients with less severe injuries had a higher HHS at the final follow-up, and patients with severe and contaminated injuries and those with disrupted abductor mechanism had worse outcomes and higher complication rates. Additionally, we observed that after the arthroplasty procedure patients’ clinical score and quality of life score increased compared to their preoperative condition despite the severity of the injury.
Arthroplasty or arthrodesis for patients with a hip joint gunshot injury should be planned under elective conditions because of the risk of infection. 9,10 In the current study, total hip joint arthroplasty was applied at mean 4.9 months after the injury. None of the patients in this case series with mobility limitations due to a gunshot wound accepted the option of arthrodesis. In the current study, the postoperative mean HHS was 65.8 (poor). Although this is poor as a functional result, when it is considered that the mean preoperative score was 25, there was relative patient satisfaction observed. When the patients were examined separately in the groups, patients in group I obtained a better HHS functional outcome.
Similar to the current study, a previous study stated that hip arthroplasty was an effective method for cases with post-traumatic arthritis developing after gunshot injury. There are few cases in the literature of hip arthroplasty after gunshot injury, 2,11 but of these, the current study comprises the youngest age group. In a series of nine cases with gunshot injury-induced secondary arthritis, Naziri et al. reported the mean age to be 59 years. 2 The authors reported significant increases in HHS, visual analogue scale and Short Form-36 (SF-36) score, and therefore recommended total hip arthroplasty after hip joint gunshot injury. 2
In our department, the posterior approach is preferred for total hip prosthesis. Therefore, the total hip arthroplasty was applied to all the patients in this series with a posterior approach. In patients with post-traumatic arthritis developing after gunshot wounds, it was emphasized that surgery is more difficult than primary total hip arthroplasty due to metallic fragments, soft tissue damage and adhesion. 2 These same problems were encountered in the current cases. However, the posterior approach provides a good view of the joint. Moreover, no dislocation was observed during follow-up.
After gunshot injury, in addition to bone pathologies, severe soft tissue damage may be accompanied by neurovascular damage. 12,13 Infection, cartilage damage, synovitis, foreign body reactions and lead poisoning may also be observed along the track of the bullet through the soft tissue. 11,14 Before beginning surgical treatment, all of these should be considered. No lead intoxication was observed in any of the current study patients. During the arthroplasty surgery, debridement of the tissue around the joint was performed, and all the bullet fragments were removed as far as possible. Intraoperative debridement and irrigation also allow for detailed examination of the joint and related injuries. Removing the bullet from within the joint is important to protect against septic arthritis, lead toxicity and cartilage damage. 3,15
In group I patients with abductor muscle length preserved, rapidly progressing arthrosis and mechanical obstruction were seen preoperatively because of bullet fragments in the joint after the injury. The best postoperative functional results were seen in this group. For good functional results after total hip prosthesis, the restoration of the abductor lever arm length is important. 16
In group II patients, the adductor arm was short and contracted so it was necessary to perform femoral shortening in these patients. Shortening of the femur is important to be able to minimize the risk of damaging neurovascular structures due to excessive limb lengthening. Furthermore, reduction of the femoral head into the true acetabulum remains challenging without shortening the femur. 17
No findings of infection were determined in any of the patients preoperatively. However, postoperative infection was observed in group III patients because of contamination of the hip joint by intestinal contents. It was previously reported that the hip joint can sometimes be contaminated by bowel contents following gunshot injury. 15 For transabdominal gunshot injuries including the hip joint, algorithms were published recommending emergency irrigation and debridement with empirical antibiotic treatment including gram-positive, gram-negative and enteric organisms. 18 Several studies have shown that there can be devastating sequelae following hip gunshot injury. The reason for this is that widespread bone and cartilage destruction require more than one operation. In addition, as the trauma severity and degree of contamination increase, so the long-term hip functions and HHS are seen to decrease. 15 Poor functional results were seen in the group III patients. Similar to the current study results, Becker et al. reported that four of five patients with transabdominal and hip gunshot injury developed infection. The mean HHS of patients with infection in that study was 48.5 and for the non-infected patient it was evaluated as 86 points. 19
Although this type of injury is uncommon, intestinal injuries opening on to the hip joint have a high risk of infection. 19 An aggressive treatment method is mandatory when an abdominal injury includes the hip joint. 19 In addition, there is no definitive evidence in the literature related to when arthroplasty can be applied after the injury. In the current study, the arthroplasty treatment was applied to patients with no preoperative findings of infection at least 3 months after the injury. Despite this, infection was encountered in two patients in group III. Based on the authors’ experience, in patients where there is contamination of the hip joint with bowel contents, it can be recommended that following debridement and the application of a spacer with antibiotics, total hip prosthesis is applied at the second stage. However, there is a need for further studies to demonstrate the efficacy of this recommendation. In the literature, poor functional results were reported in cases of acetabulum fracture and when the pelvis was contaminated with bowel contents because of a gunshot injury. 18
The severity of the injury and degree of contamination in patients with a hip gunshot injury vary from patient to patient. 15 In the current study, the severity of the injury was observed to increase from group I to group III. In the literature related to these kinds of injuries, there are patient series that presented the results of acute treatment. 20 The current study can be considered of value as the first to present the results and recommend a treatment algorithm for arthroplasty following a hip gunshot injury, which is a difficult injury to treat.
We note some limitations for the current study. Firstly, the study population was small. In addition, more extensive evaluations of quality of life measurements and patient satisfaction were not applied. However, this study is the first in the literature evaluating the outcomes of total hip arthroplasty after hip joint gunshot injury with the largest patient population. Retrospective design of the study is another limitation of the current study. Nevertheless, we evaluated prospectively collected patient data and the retrospective design of the study also prevents patient selection bias. Additionally, we created three groups according to the severity of the hip joint gunshot injury and this information may guide orthopaedic surgeons in the management of total hip arthroplasty after hip joint gunshot injury. We had no patient neurovascular deficit preoperatively; maybe patients with neurovascular deficit may constitute a more severe group as group IV. For a more comprehensive classification and better understanding of the prognosis of total hip arthroplasty after hip joint gunshot injuries, further studies with large patient populations are needed about arthroplasty after gunshot injuries of the hip joint.
Conclusions
Gunshot injuries of the hip joint can be challenging and have devastating long-term problems. Hip arthroplasty after a hip joint gunshot injury is a good treatment choice in young patients to reduce pain and regain function. However, very high infection rates can be seen in patients with accompanying intestinal injury. This group of patients must be treated with caution in terms of infection. The outcomes of the treatment recommended in the current study should be considered according to the severity of the injury and the degree of contamination. There is a need for future multi-centre studies of large patient populations which are based on classification according to severity of gunshot injury in the hip joint.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.