
Abstract
Background:
Spinal tuberculosis (TB) is a leading cause of damage to the spine and associated neural structures.
Purpose:
This study aims to identify the risk factors for neurological deterioration in spinal TB patients to promptly care for the patients before paralysis develops.
Methods:
The demographics, clinical characteristics, laboratory results, and radiographic findings of spinal TB patients were collected between 1993 and 2016. The data were analyzed using logistic regression methods. The predictive factors for neurological deficit were identified.
Results:
There were 125 spinal TB patients (70 men and 55 women). The average age ± standard deviation was 55.7 ± 2.0 and 52.3 ± 2.4=years, respectively. According to the univariate analysis, the significant risk factors associated with neurological deterioration were signal cord changes, notable Cobb angle (>30°), radiating pain, and epidural abscess. The multivariate analysis revealed that only signal cord change and notable Cobb angle significantly influenced neurological status.
Conclusion:
The predictive factors for neurological deterioration in spinal TB patients are signal cord change and notable Cobb angle. Surgery should be considered in patients who present with these factors before the development of neurological deterioration.
Introduction
The World Health Organization (WHO) estimates that there are more than 10 million new cases of tuberculosis (TB) each year. 1 Among all tuberculous infections, the incidence of spinal TB is 1%, 2 and spinal TB represents one-half of extrapulmonary TB cases. 3,4 Spinal TB is also the most common and serious form of musculoskeletal TB; it can cause pain, vertebral destruction, and neurological deficit. 3 Due to motor deficits, patients have poor daily living activity. Laboratory investigations, radiographs, and magnetic resonance imaging (MRI) inform spinal pathoanatomy and help in making a diagnosis. 5 –9 Spinal TB frequently affects thoracic and lumbar spine, leading to the destruction of the spine and can cause neurological compression. 10 Management of spinal TB can be classified into those with neurological complication and those without neurological complication. Anti-TB medication is the mainstay of treatment for both groups. However, for a patient with neurological complication, the addition of surgical treatment provides better results. 11 The results will be the best if the patients at risk for neurological deterioration are identified and treated promptly. The literature, however, have limited information about the risk factors for predicting neurological deterioration in adult spinal TB patients. 12 It is believed till date that the neurological deficit may be associated with the patient’s age 12 and signal cord changes on MRI T2-weighted image. 6 The purpose of our study was to determine the predictive factors for neurological deficit in spinal TB patients.
Materials and methods
Study design and population
The study protocol was reviewed and approved by the Institute’s Ethics Committee for Human Research based on the Declaration of Helsinki and the ICH Good Clinical Practice Guidelines (HE571094).
Medical records of 125 spinal TB patients seen consecutively at our institute between 1993 and 2016 were retrospectively reviewed. For nonoperated patients, the diagnosis of spinal TB was based on the therapeutic diagnosis (the clinical responses to anti-TB medication). For operated patients, the diagnosis was based on pathological specimens, tissue cultures, or polymerase chain reaction (PCR) for TB. The TB spine patient with active disease and/or early onset of neurological deficit were included. The patients who had a late-onset neurological deficit in a healed TB 10 were excluded from the study. The data collection included patient characteristics, clinical features, neurological status, laboratory results, radiographic findings, and MRI findings.
Outcome measurement
Data on possible risk factors were also collected, including: (a) clinical characteristics (i.e. age, sex, local spine tenderness, radiating pain, body temperature, urinary incontinence, and neurological deficit); (b) erect radiographic results and MRI findings (i.e. Cobb angle, 13 vertebral collapse, endplate destruction, signal cord change, posterior element involvement, epidural abscess, disc space involvement, and level of spine involvement); and (c) laboratory investigations (i.e. erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)). All factors were recorded as present or absent, except for: (i) age (which was recorded as years); (ii) kyphosis or lordosis (which was classified as <30° or >30° using the Cobb method 14 –19 (the angle between the upper border of the upper normal vertebra and the lower border of the lower normal vertebra); (iii) ESR (which was recorded as <40 mm/h or >40 mm/h); and (iv) collapse (which was recorded as <50% or >50% anterior vertebral body height loss).
Statistical methods
To achieve 80% power, 20 a total number of 110 patients were needed to have a 95% chance of detecting a 0.6 odds ratio (OR) of having a neurological deficit, based on a 30% incidence of neurological deficit in patients with TB spine. 2
Descriptive statistics included mean, standard deviation (SD), and 95% confidence interval (CI). The baseline demographic data were compared between the neurological deficit and control groups. The continuous variables and categorical data were compared using the independent t-test and nonparametric tests, respectively. Univariate and multivariate logistic regression analyses were used to determine the risk factors for neurological deficit. Variables from the univariate analyses—indicating an association with neurological deficit (i.e. p value <0.2) 21 —and in the literature were included in the multivariate regression analyses. Backward logistic regression was used for model building. The overall significance level of the study was set at 0.05. All data were analyzed using IBM SPSS Statistics (version 20, IBM Corporation, Armonk, New York, USA), and post hoc power analysis of the study was calculated using G*Power (version 3.0.10). 22
Results
A total of 125 spinal TB patients including 70 men (mean age 55.7 ± 2.0) and 55 women (mean age 52.3 ± 2.4) were enrolled. Most of the spinal TB involved the thoracic (68.8%), followed by the lumbar (23.2%) and the cervical spines (8.0%). There were 77 cases of neurological deficit (Table 1) including the quadriplegia for three cases, paraplegia for five cases, complete motor deficit of lower limbs with preserve some pinprick sensation for 25 cases, paraparesis with motor power less than grade 3 for 32 cases, and paraparesis with motor power grade 3 or 4 for 12 cases. All patients with neurological deficit were operated. In patients without neurological deficit, seven cases were operated on due to psoas abscess and 10 cases were operated for their tissue biopsies.
Demographic data of the spinal TB patients at initial visit.a
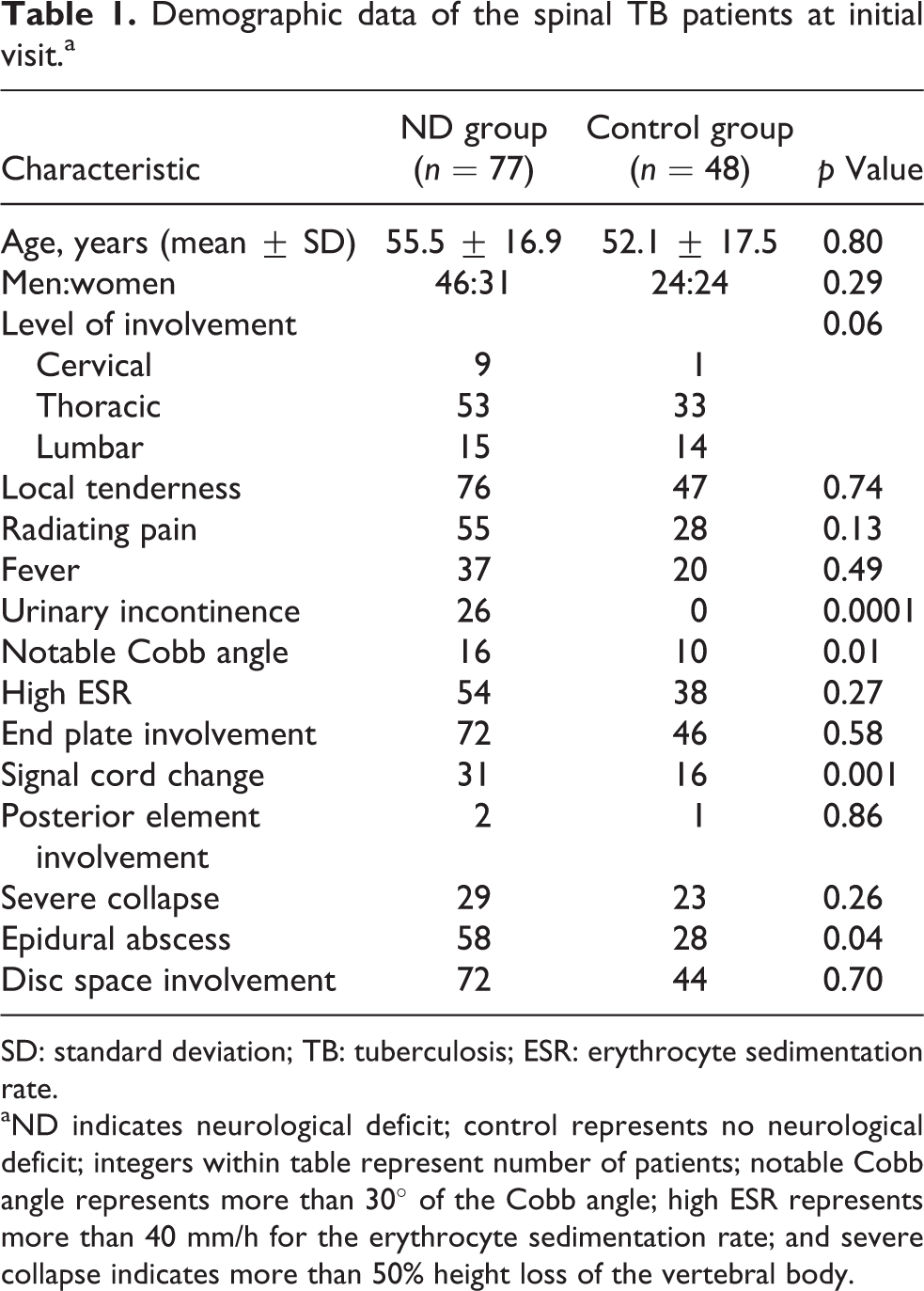
SD: standard deviation; TB: tuberculosis; ESR: erythrocyte sedimentation rate.
aND indicates neurological deficit; control represents no neurological deficit; integers within table represent number of patients; notable Cobb angle represents more than 30° of the Cobb angle; high ESR represents more than 40 mm/h for the erythrocyte sedimentation rate; and severe collapse indicates more than 50% height loss of the vertebral body.
According to the univariate regression analyses, the significant risk factors (p value <0.2) were signal cord change (Figure 1), notable Cobb angle (>30°) (Figure 1), epidural abscess, and radiating pain (Table 2). For comparison, previous studies included age and severe collapse as risk factors for the neurological deficit in spinal TB patients. We included all of these factors in the multivariate regression analyses, but after backward stepwise logistic regression analyses (Table 3), only signal cord change and notable Cobb angle were significant risk factors. The adjusted OR was 3.31 (p = 0.003) and 2.62 (p = 0.04), respectively. The Nagelkerke R 2 from backward stepwise logistic regression ranged between 0.21 and 0.32, and post hoc power analysis of the study was 0.97.

A 25-year-old man with spinal tuberculosis presented with 58° of kyphosis (a) and hyperintense signal cord change (together with anterior and posterior spine destruction) at the area of kyphotic deformity on T2-weighted image (b). The antituberculosis medication was started, but he had progressive paraplegia within a few weeks after the initial visit. Then, the spinal cord decompression and spinal instrumentation were operated promptly. After surgery for 4 months, the patient was able to walk independently with almost grade 5 motor power of his lower limbs.
Univariate analyses.a

CI: confidence interval; ESR: erythrocyte sedimentation rate.
aNotable Cobb angle represents more than 30° of the Cobb angle; high ESR represents more than 40 mm/h erythrocyte sedimentation rate; and severe collapse indicates more than 50% height loss of the vertebral body.
b p < 0.2: significant risk factors from univariate analyses.
Multivariate analyses of possible risk factors.a
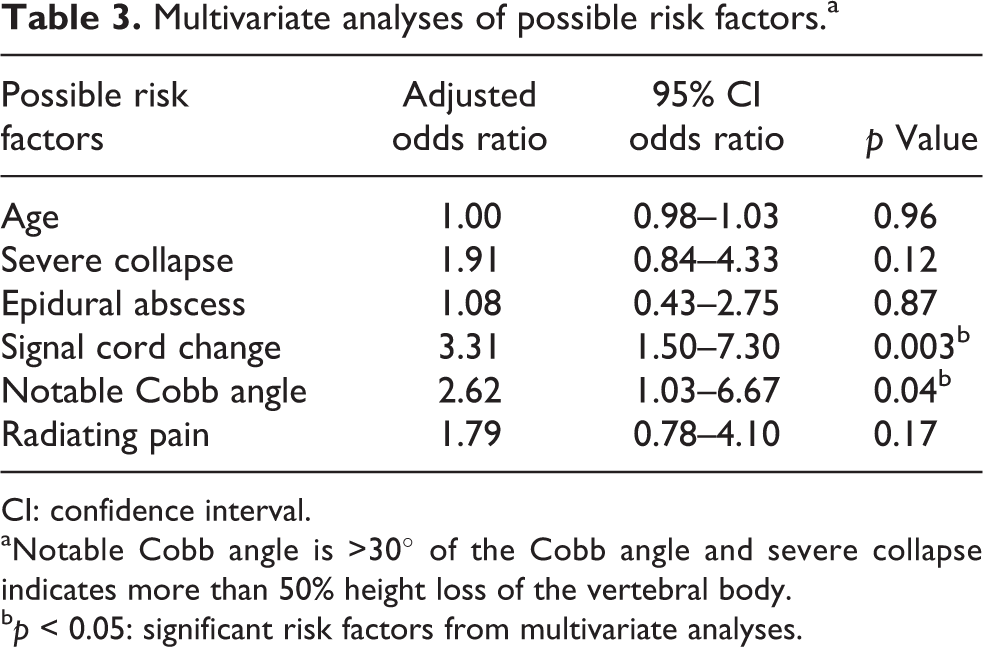
CI: confidence interval.
aNotable Cobb angle is >30° of the Cobb angle and severe collapse indicates more than 50% height loss of the vertebral body.
b p < 0.05: significant risk factors from multivariate analyses.
Discussion
The clinical features of TB spine vary; they can be either systemic or local diseases but are often nonspecific. The clinical features in our TB spine patients were similar to those described in previous studies, with backache (58%), fever (22%), and weight loss (19%) being the most commonly presenting symptoms. 23 We also diagnosed TB spine using the typical features of spinal TB seen on MRI including the lesion that originated from vertebral endplate, anterior vertebral body involvement, subligamentous spreading, preserved disc space, preserved pedicle, and/or multiple vertebral body lesions. An MRI was performed in the early period after the patient’s admission or after neurological deterioration.
Most of the spinal TB involved the thoracic (68.8%), followed by the lumbar (23.2%) and the cervical spines (8.0%). Considering only for thoracic spinal TB, the univariate analysis showed that the respective crude OR of signal cord change, notable Cobb angle, epidural abscess, and radiating pain were 3.78, 3.67, 2.47, and 1.32 (all p value <0.2). Again, the multivariate analysis showed that the adjusted OR for signal cord change was 3.68, p value = 0.005 and for notable Cobb angle was 2.57, p value = 0.048. These were very close to the crude OR and adjusted OR of all levels of the spinal TB (Tables 2 and 3). From this analysis of covariance, the level of spine involvement is not the factor affecting the results of the study. The data including all levels of the spine were used to keep larger sample size, power of the study, and generalizability.
All 77 neurological deficit patients received surgical decompression. However, the mean time before the operation was 3.8 days (ranged between 1 day and 9 days) depending on the referral time of each patient to tertiary referral hospital. Transportation time and finance still remain problems in developing countries. If the TB spine patients at risk for neurological deficit can be identified early, then the patients can be managed to prevent their neurological deterioration.
The frequency of neurological involvement has been found to vary across studies, from 23% to 76% of patients. 4,24 –26 For laboratory investigations, the elevated ESR and CRP are recommended more than leukocytosis, which has proved less useful. 27 Radiographic changes associated with TB spine include mainly the destruction of the vertebral end plates and vertebral body destruction, while some cases may have disc space narrowing in the late phase of the disease. These findings may not be visible on plain radiographs for up to 8 weeks. 3,28 –30 An MRI provides earlier and better information about the spinal canal and spinal cord lesions. The typical MRI features of TB spine are that the involved vertebral body and vertebral end plate are severely damaged, with evidence of osteomyelitis, and the epidural space is affected by the extension of the paravertebral abscess or epidural abscess. 3,31 Neural compression from spinal TB is gradual, so neural compression seen on MRI is not strictly associated with clinical neurological deficit. 32 One study reported that age, level of spinal infection, vertebral body collapse, and abscess were associated with neurological deficit. 12 Signal cord change on T2-weighted image is not correlated with synchronous neurological deficit, 6 whereas another study reported that signal cord change on T2-weight image is associated with neurological deficit. 32 Recently, Kumar 33 pointed out that neurological status, back pain, back muscle spasm, diminished disc space, paradiscal vertebral endplate destruction, vertebral collapse, and Cobb angle were the factors associated with TB spine. We, therefore, integrated these mentioned clinical, laboratory, radiographic, and MRI findings as the possible risk factors for neurological deficit.
From the univariate OR, the risk factors for neurological deficit were the signal change of the spinal cord, notable Cobb angle, radiating pain, and epidural abscess. For the multivariate logistic regression analysis, we also included the literature-accepted risk factors of age and severe collapse.
From the adjusted OR, the notable Cobb angle and the signal cord change were the only statistically significant risk factors. These are the predictive factors identified from radiographic and MRI findings; these should be investigated in patients suspected of having spinal TB.
Compared to previous studies, Tan et al. 7 found the ESR was the predictive factor for neurological deficit. In contrast to our study, the ESR was not found to be the predictive factor for neurological deficit. Our finding has corresponded well with the review article of Guerado and Cerván 27 that the high ESR together with high-level CRP were useful laboratory findings for TB spine diagnosis (but not the risk factor for neurological deficit). Contrarily, Javed et al. 34 found that the laboratory results of ESR and CRP had large SD and should not be considered as part of final criteria in TB spine diagnosis. Similar to the current study, ESR and CRP were not found to be the predictive factors for neurological deficit. Age is reported as the factor associated with the neurological deficit. 12 Recently, Marais et al. 35 compared patient who had TB spondylitis and those who had no bony involvement. They found that TB spondylitis patients had a significantly older age than the others. Neurological deficit was seen in similar proportion between these two groups. In line with our study, age was not found to be a significant predictive factor for the neurological deficit.
The limitation of the current study was the method of TB spine diagnosis as only the operated patients were diagnosed by tissue pathology, tissue culture, or tissue PCR, while the nonoperated patients had only a therapeutic diagnosis. Most of the limitation for tissue biopsy were patient’s rejection for this invasive procedure. The others were the time for the bacteriological culture which usually takes 4–6 weeks incubation period and against advice due to the risk of surgical complication. Once diagnosed the spinal TB, all patients were treated with the usual doses of anti-TB drugs composing the isoniazid, rifampicin, ethambutol, and pyrazinamide. Depending on the referral time to the hospital and the time to start the anti-TB drugs, some patients still developed neurological deterioration. For the control group of 48 individuals who were treated conservatively, the disease was healed as well after 12–18 months of anti-TB drugs. The diagnosis of spinal TB in this group was based on the endemic area of TB, clinical of night pain, constitutional symptoms, elevated ESR, elevated CRP, Roentgenographic findings compatible with spinal TB, and response to anti-TB drugs. 36,37 For the operated patients, like the recent review, most of the operations in neurological deficit patients were anterior decompression, grafting, and posterior fixation, while tissue biopsy and abscess drainage were the most common operations in patients without neurological deficit. 38 In the current study, we excluded urinary incontinence from the multivariate logistic regression model building because bladder incontinence can be categorized as a type of neurological deficit and it is not a risk factor predictive of neurological deficit.
The clinical application of this study is that spinal TB patients who present with normal neurological status with signal cord change have 3.31 times greater risk of developing neurological deficit than patients with no signal cord change. Similarly, the risk for neurological deficit was 2.62 times greater for patients with a notable Cobb angle than those <30° Cobb. Patients with radiating pain (p value <0.2 from the univariate analysis 21 in Table 2) are 1.8 times more likely to develop neurological deficit than those who do not. So, in patients diagnosed with TB spondylitis with radiating pain, radiography and MRI are recommended. The recent study described that the severe kyphosis was associated with retropulsed bony and disc sequestration, 39 while the signal cord change was the inflammatory spinal cord edema. Similar to the current study, if the patient has a notable Cobb angle together with signal cord change in MRI findings, a neurological deficit is likely, and the patient should be closely followed up or surgical treatment considered. If the surgery was chosen, we recommend both the decompressive and the corrective surgeries.
Based on the multivariate logistic regression model building, the predicted probability of developing neurological deficit can be calculated (Figure 2). For example, TB spine patient with signal cord change and notable Cobb angle has 80% of the probability of developing neurological deficit

The formula to predict the probability of developing neurological deficit in spinal tuberculosis.
For the TB of lumbar spine below the spinal cord level, the main predictive factor is the Cobb angle. If the patient has a notable Cobb angle, then this patient has 54% of the probability of developing neurological (nerve root) deficit
Conclusions
The predictive factors for neurological deficit in spinal TB are the signal change of the spinal cord on MRI finding and a notable Cobb angle. Neurological deficit is likely to occur in spinal TB patients who have both risk factors. Therefore, surgery should be considered for these patients. In patients who have both the notable Cobb angle and the signal cord change, decompressive and corrective surgery is recommended.
Footnotes
Acknowledgements
We would like to acknowledge Bryan Roderick Hamman for assistance with the English-language presentation of the manuscript under the aegis of the Publication Clinic, Research Affairs, Khon Kaen University, Thailand.
Author contributions
All authors designed the protocol. Kriwut Leurmprasert and Nattamon Wongba collected the data. Surachai Sae-Jung supervised the study and analyzed the data. All authors participated in the manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.