
Abstract
Objective
This study was performed to investigate the clinical features, risk factors, and outcomes of bone and joint tuberculosis in patients undergoing dialysis.
Methods
We systematically reviewed the medical records of 17 patients with bone and joint tuberculosis undergoing dialysis who were admitted to our hospital from January 2009 to January 2019.
Results
Seventeen patients with bone and joint tuberculosis undergoing dialysis were identified in this retrospective study, and 13 patients were undergoing hemodialysis. The mean age of the 17 patients was 61.3 years (range, 32–82 years), and 10 (58.9%) patients were male. Most of the patients had a low CD4+ cell count and low hemoglobin and albumin levels. Surgery was performed in 6 patients (35.3%), and 13 of the 17 patients (76.4%) were cured. Three patients had bone or spine sequelae, mainly because of a delayed diagnosis, and one patient died of heart failure.
Conclusion
These findings indicate that older age, a low CD4+ cell count, and low hemoglobin and albumin levels are possible risk factors for bone and spine tuberculosis in patients undergoing dialysis. If diagnosed early, most patients should have a good outcome after anti-tubercular therapy with or without surgery.
Introduction
Tuberculosis (TB) is a significant public health problem and a leading cause of infectious morbidity and mortality worldwide.1,2 Numerous hospital-based cohorts and regional registry studies have shown that the risk of TB in patients undergoing hemodialysis and peritoneal dialysis is 3- to 25-fold higher than that in the general population.3,4 In many reports, the bones and joints are identified as the third most frequent sites of extrapulmonary TB.5,6 Bone and joint TB is associated with chronic pain, deformity, and disability; therefore, early diagnosis and treatment is desirable.7–9 However, few studies have focused on bone and joint TB in patients undergoing dialysis, especially peritoneal dialysis. We herein describe 17 patients undergoing dialysis who were treated for bone and joint TB in our hospital during the past 10 years.
Patients and methods
Patients
In this retrospective study, we reviewed the medical records of patients undergoing dialysis who developed bone and joint TB and were treated at Huzhou Central Hospital from January 2009 to January 2019. A diagnosis of bone and joint TB was made based on clinical symptoms affecting the bones or joints and microbiologic or histopathologic evidence of TB at the affected site.
Data collection
The patients’ medical records were further reviewed to obtain demographic, medical, and laboratory data. These data included sex, age, dialysis duration, and presenting symptoms; comorbidities, including diabetes, hypertension, heart disease, and malignancy; immunosuppressive therapy, intravenous iron treatment within the past year, and history of TB; laboratory data, such as the white blood cell count, C-reactive protein level, albumin level, erythrocyte sedimentation rate, and Kt/V urea-dialysis; treatments, including anti-tuberculous and surgical interventions; and post-management outcomes (after 6–9 months of anti-tuberculous therapy). The outcomes were defined as cure, sequelae, or death according to a previous study in Denmark. 10 Variables are presented as mean ± standard deviation or proportion.
Ethics and informed consent
This study was approved by the local ethics committee of Huzhou Central Hospital (ethics approval number 2019021). Verbal informed consent was obtained from each patient or his or her parent/caregiver.
Results
Seventeen patients undergoing dialysis who developed bone and joint TB were identified in this retrospective study. The patients’ demographic and clinical characteristics are summarized in Table 1. The mean age of the patients was 61.3 years, and 10 patients were male. Most of the patients were undergoing hemodialysis. The mean duration of dialysis at the time of TB diagnosis was 3.9 years. All but one of the patients had hypertension; most had other comorbidities. The mean hemoglobin level was lower than the reference range, and 10 patients had a history of intravenous iron treatment within the past year. Most of the patients had a low albumin level. Nine patients had a low CD4+ cell count, and in six patients it was <300/mm3.
Demographic and general clinical characteristics of patients undergoing dialysis with bone and joint TB.

Data are shown as mean ± standard deviation, median (range), or n (%).
IV, intravenous; TB, tuberculosis; IgG, immunoglobulin G; PTH, parathyroid hormone.
As shown in Table 2, all patients presented with local pain, and 10 patients had a fever. The lumbar spine was the most susceptible site, followed by the thoracic spine. Two patients also had concomitant pulmonary TB. TB was confirmed by histopathology in 10 patients; 6 underwent operative focal cleaning and 4 underwent CT-guided bone biopsy. Another seven patients underwent drainage of abscesses or synovial fluid, and their polymerase chain reaction or culture results were positive for TB. The average duration from initial symptoms to diagnosis was 30.3 days. Seven patients had a bone or joint deformity, and imaging examinations showed a spinal or articular cold abscess in five patients. Eleven patients underwent nonsurgical treatment consisting of drainage or anti-tuberculous drugs. Bone or spine TB was cured in 13 patients, and 3 patients developed bone or spine sequelae (paraplegia in 1, limb numbness in 1, and articular dyskinesia in 1). One patient died 2 months after anti-tuberculous therapy, mainly because of heart failure. No serious drug-related adverse effects requiring drug discontinuation occurred in this study.
Bone or joint presentation in patients undergoing dialysis with bone and joint TB.
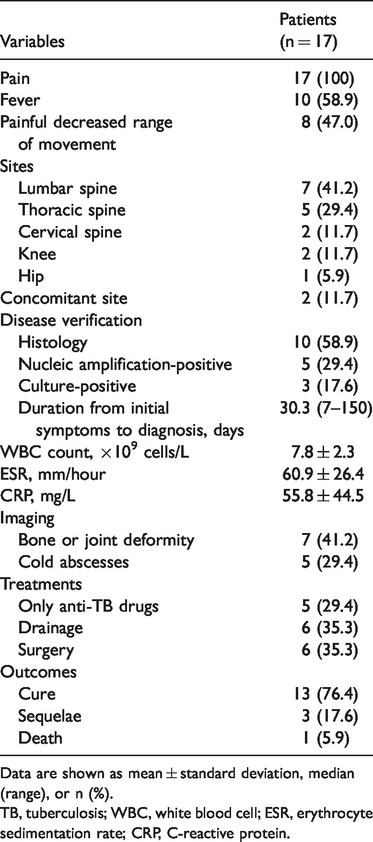
Data are shown as mean ± standard deviation, median (range), or n (%).
TB, tuberculosis; WBC, white blood cell; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein.
Discussion
Infections remain a significant cause of morbidity and mortality in patients undergoing dialysis.11,12 China is one of seven countries worldwide with a high number of TB cases. 2 During the past 10 years, we identified 17 cases of bone and spine TB in patients undergoing dialysis, mainly hemodialysis. Considering that the number of patients undergoing hemodialysis is two- to three-fold higher than the number of patients undergoing peritoneal dialysis in our hospital, the incidence of bone and spine TB may actually be similar in the two groups.
The clinical characteristics and laboratory findings in our patients were similar to those previously described by other research groups.13,14 The spine was the most susceptible site, and local pain and fever were the most common presenting symptoms. The patients had a long duration from initial symptoms to diagnosis, especially those with TB affecting the thoracic spine. This long delay may be attributed to the fact that spinal TB is a chronic process and that patients and physicians are often unaware of the clinical characteristics of this condition. 15 Imaging methods play an important role in the diagnosis of bone and spine TB, and magnetic resonance imaging remains the method of choice, especially for spinal TB. 16 In most of the patients in our study, the radiological and histopathological findings suggested underlying TB. However, bone and joint TB remains a diagnostic challenge. Close multidisciplinary collaboration among orthopedic surgeons and pathology and laboratory services can help to improve the diagnostic accuracy. 17
Patients undergoing dialysis are more likely to develop TB than the general population, mainly because of the impaired cellular immunity associated with renal impairment.18,19 In six of nine patients in our study with a low CD4+ cell count, the cell count was <300/mm3, indicating a state of impaired cell-mediated immunity in these patients. In addition, the patients in our study were older, and many had diabetes and low albumin and hemoglobin levels, which also leave patients susceptible to TB infectious complications.20,21 Moreover, a previous study showed that patients with chronic kidney disease who developed pulmonary TB were significantly more likely to have received intravenous iron therapy, and iron is a co-factor supporting mycobacterial growth. 22 In our study, more than half of the patients had received intravenous iron treatment within the past year, which may also be a risk factor for the development of bone and spine TB.
In most of our patients, the only treatment performed was drainage or administration of anti-tuberculous drugs. In our treatment strategy, operations for spine TB are performed in the presence of neurological signs of spinal compression shown by magnetic resonance imaging or when spinal decompression and stabilization are required. 23 In patients with joint TB, infection affecting the hip or shoulder often requires open surgical drainage, but more accessible joints such as the knee can sometimes be managed by serial aspiration. 24 Three patients in our study had bone or spine sequelae that were mainly due to the long duration from initial symptoms to diagnosis. Only one patient with heart failure died, indicating that bone or spine TB itself might not increase mortality.
In summary, we retrospectively reviewed 17 patients undergoing dialysis who developed bone and joint TB. The lumbar spine was the most susceptible site. Older age, low albumin and hemoglobin levels, and a low CD4+ cell count may be risk factors for bone and joint TB in patients undergoing dialysis. Surgery was only performed in one-third of our patients, and three-quarters of patients were cured.