
Abstract
Purpose:
The objective was to evaluate the clinical and patient-related short- to medium-term performance of the OPTY-LINE nail device for high tibial osteotomy (HTO), comparing a case series of the said device to the established Tomofix fixed-plate device.
Patients and Methods:
Males with symptomatic medial compartmental osteoarthritis and no serious (co-morbid) knee pathology were followed up, five Tomofix and six OPTY-LINE patients. Patients underwent computed tomography assessment and completed Knee Injury and Osteoarthritis Outcome score (KOOS) and osteotomy surgery patient satisfaction questionnaires, 3 and 6 months post-surgery. A radiologist impression score and a quantitative digital bone density analysis were performed by two independent radiologists. Mann–Whitney U test was applied for inferential statistical tests.
Results:
At 6 months post-surgery, for Tomofix, the median radiologists’ healing impression score was ‘progressive healing’ versus ‘union virtually complete’ for the OPTY-LINE nail; bone healing quotient was 1.30 (standard deviation (SD) 1.74) versus 1.78 (SD 1.58), p = 0.18. The post-operative absolute surgical accuracy was a mean 12 (7.5) for Tomofix versus 4.1 (2.3) for OPTY-LINE, p = 0.052. At baseline, however, Tomofix patients had more knee symptoms, as determined by KOOS symptom sub-score, when compared to the OPTY-LINE cohort (p = 0.009).
Conclusion:
This initial, non-randomized, comparative evaluation of the OPTY-LINE device for HTO has produced similar outcomes to patients treated with the established Tomofix device. In particular, the rate of post-surgical bone regeneration and surgical accuracy achieved with the OPTY-LINE device are encouraging. Large-scale randomized controlled studies with longer follow-up are indicated to further evaluate the clinical and patient-related outcome performance for OPTY-LINE.
Keywords
Introduction
Angle stable plates are the current implants of choice in open-wedge high tibial osteotomy (HTO) offering increased stability and earlier post-operative weight-bearing than their predecessors. 1,2 Some authors have described full-weight bearing as early as 2 weeks post-surgery without negative impact. 3 Tomofix patients tend to resume normal activities of living soon after surgery with work-related physical activities introduced at 3–4 months and sports after approximately 6–12 months. 4,5 One reservation for allowing patients to fully weight bear early on is the perceived risk of loss of correction of the angle, although in practice this effect appears to be a rare occurrence. 1,6,7 Histologically, there is variability in the degree of healing and indeed maturation of bone regeneration achieved in the open wedge. With current fixed-plate devices, even 18 months post-procedure, a minor subset of patients will not have significant signs of regeneration in the gap. 8
Gradual HTO wedge opening and stabilization can be achieved with the recently CE-marked OPTY-LINE system (NuVasive Specialized Orthopedics, San Diego, California, USA). The OPTY-LINE device is an extendable nail which is inserted into the proximal tibial intramedullary canal after the osteotomy is created in the conventional manner. Figure 1(a) shows a schematic drawing of the full-length OPTY-LINE device, including where it is fixed to the tibia. Following surgery the nail is slowly extended over a period of time until the distraction gap and thereby the bone correction angle is satisfactory, as measured by X-ray imaging. Figure 1(b) demonstrates schematically how the proximal mediolateral screw changes its angle in relation to the longitudinal axis of the nail as the distraction produces opening of the wedge via the anteroposterior (AP) screw. The null hypothesis is that there would be no difference in outcome for rate of bone healing and surgical accuracy in cases using the new OPTY-LINE design in comparison with cases using the established gold standard Tomofix plate. Timely healing of the osteotomy gap is of clinical importance since, in the majority of cases, it allows the patient to resume activities such as sports even if the supporting device is removed. 4,9 Surgical accuracy is extremely important for successful outcome in HTO. 10 Inaccuracy leads to poorer outcomes with higher revision rates or conversion to arthroplasty. The main objectives of this comparative study are therefore to introduce the surgical methodology for the new OPTY-LINE device and appraise its relative performance to the Tomofix device with particular focus on the post-operative bone healing process and surgical accuracy.

OPTY-LINE device for high tibial osteotomy. (a) Schematic drawing of the complete device, depicting the locations of the four screws for fixation and the housing tube containing magnet, gears and threaded pin which is distracted in stages post-operatively. Image courtesy of Nuvasive Specialized Orthopedics. (b) Schematic drawings of the status of the high tibia and knee joint immediately post-surgery (left) and 6 weeks later (right) following distraction of the rod within the OPTY-LINE device. Image courtesy of Nuvasive Specialized Orthopedics. ML: medial–lateral; AP: anterio-posterior.
Patients and methods
Study design and subjects
The study is a prospective, open label, two-armed, single-centre therapeutic study. The study is registered with ClinicalTrials.gov, identifier NCT02717845. Two cohorts of patients were enrolled into the study without randomization. The participants either underwent HTO with the OPTY-LINE system or the Tomofix plate (DePuy Systhes, West Chester, Pennsylvania, USA). Patients were identified prospectively from surgical and clinical lists. Only males were enrolled into the study to make the study more controlled and for two relevant reasons: to minimize fetal risk with increased ionizing radiation and to avoid confounding due to the known difference in bone density between males and females. 11
A total of 12 patients were recruited into the study, and it concerned seven OPTY-LINE patients and five Tomofix patients. One of the OPTY-LINE subjects expired during follow-up, prior to the study follow-up visits, probably due to non-surgery or medical device-related reasons and therefore six OPTY-LINE patients remained for analysis. Table 1 presents an analysis of distribution of demographics – and baseline degree of osteoarthritis – and comparison between the two cohorts.
Demographics and baseline characteristics of study subjects.
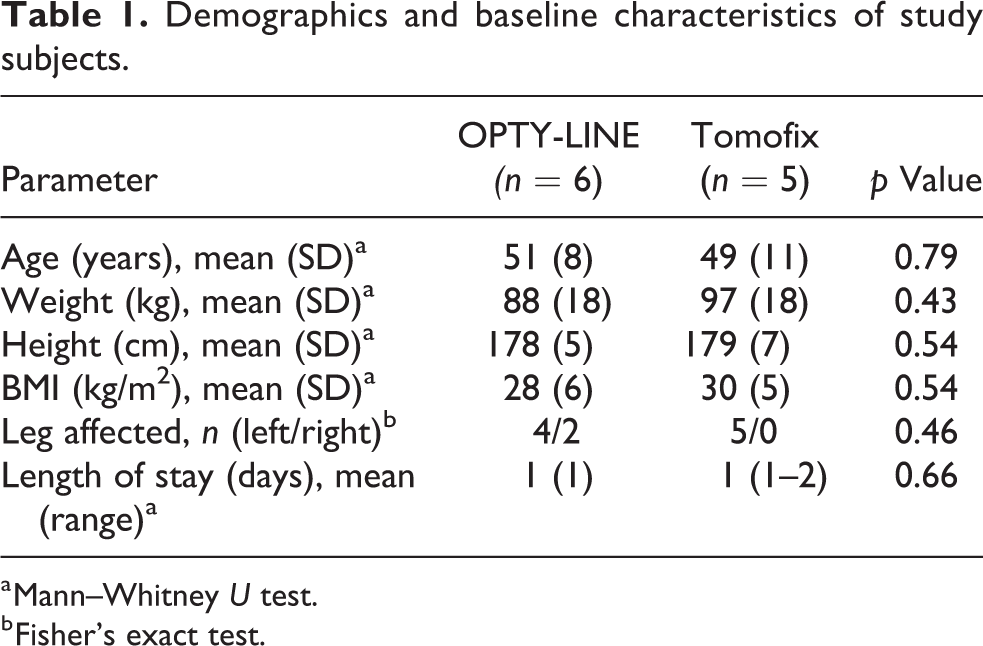
a Mann–Whitney U test.
b Fisher’s exact test.
Eligibility criteria
Inclusion criteria were treatment with medial open-wedge proximal tibial osteotomy, either with Tomofix device or with OPTY-LINE device for symptomatic medial compartmental osteoarthritis, provision of written informed consent, males, and mental capacity. Exclusion criteria were under age (<18 years), patients lacking mental capacity, females, and current use of nicotine products, including smoking and patients who cannot understand English and therefore cannot be consented. Furthermore, the following pre-existing clinical exclusion criteria were applied for potentially eligible patients: varus deformity greater than 10°, flexion contracture greater than 15°, knee flexion under 90°, medial/lateral tibial subluxation over 1 cm, medial bone loss of over 3 mm if demonstrated on radiographs, inflammatory arthritis (including use of methotrexate), arthritis in the lateral compartment, patella baja, weight over 115 kg, severe patella femoral symptoms, unaddressed ligamentous instability, fixed flexion contracture, known or suspected osteoporosis or osteopenia based on medical history and radiographic image, and requirement for other major surgical procedures at the time of the HTO surgery.
Surgical procedures and rehabilitation
Tomofix plate
Open-wedge HTO was conducted according to the method outlined in osteotomies around the knee indications-planning-surgical techniques using plate fixators and Elson et al. 12,13 According to the standard local practice, the osteotomy gap was not filled with a bone graft or other filler device.
OPTY-LINE nail
The OPTY-LINE device surgical procedure was performed as follows: with the knee bent at 90–110° with a bolster, medial para patellar approach to the tibial entry point was made. The entry point is at the anterior cortex of the tibia slightly medially in line with the tibial medullary canal. The position was verified with image intensification. Guide wire was inserted and confirmed with orthogonal views to be inside the medullary canal. Reaming was performed to 160 × 12.5 mm2, and a trial nail was then inserted. The proximal end of the nail should sit flush with the tibial plateau. Following nail insertion, the AP screw is drilled. After removal of the trial nail the HTO was performed per Elson et al. 12 Subsequently the OPTY-LINE nail was inserted and locked proximally and distally. After wound closure, the magnet inside the nail was then identified and marked on the skin aided by the image intensifier. Post-operative correction is based on preoperative planning and serial radiographs. Daily correction for each patient was typically 0.5 mm, divided into two sessions, starting 5–7 days after the operation. Weekly follow up – up to 6 weeks – with long leg alignment radiograph views were performed to optimize the corrections.
All patients
Post-operatively, patients returned to full mobility through the following steps: toe touch in first 2 weeks, partial weight bearing after 2–4 weeks, full weight bearing after 4–6 weeks (use of single crutch) and full weight bearing without aids from 6 weeks onwards. To minimize the risk of deep vein thrombosis developing, all patients were treated with a calf pump and administered clexane while in hospital and prescribed rivaroxaban for 2 weeks once discharged home.
Correction planning and post-operative surgical accuracy assessments
The approach to planning the intended knee joint correction did not differ between the two medical devices. Preoperative planning and post-operative assessments were conducted according to the method described by Elson et al. 12 For accuracy calculations, the weight-bearing axis transecting the tibia (% Mikulicz point) was used. The absolute figures for surgical accuracy were calculated in relation to post-operatively achieved Milkulicz line minus the preoperatively planned Mikulicz line. Therefore, a value of zero can be considered a perfect correction. 14,15
Study schedule
Apart from correction visits for OPTY-LINE patients, all study subjects were seen at baseline (within 1 month prior to surgery), and 3 and 6 months following their HTO procedure for collation of the patient and clinical outcome measures. At baseline, subject demographics were recorded. During each study visit, the following patient-reported outcome measures were collected: visual analogue pain scale (standard 10 cm line), Knee Injury and Osteoarthritis Outcome score (KOOS) knee health questionnaire 16 and an osteotomy patient satisfaction questionnaire (see Online Supplemental Appendix 1). The latter questionnaire is based on three earlier published questionnaires adopted for this study. 17 –19
CT imaging details
The primary outcome was the radiologist’s assessment of healing, as determined from computed tomography (CT) imaging according to a 5-point Likert-type scale devised by Brosset et al. 20 This was performed by two radiologists, FF (rater 1) and JE (rater 2), each of whom have over 10 years’ experience as a consultant radiologist. The radiologist impression scoring system, and what each score equates to, is outlined in Table 2.
Radiologists’ impression scores and quantitative assessment of bone healing.
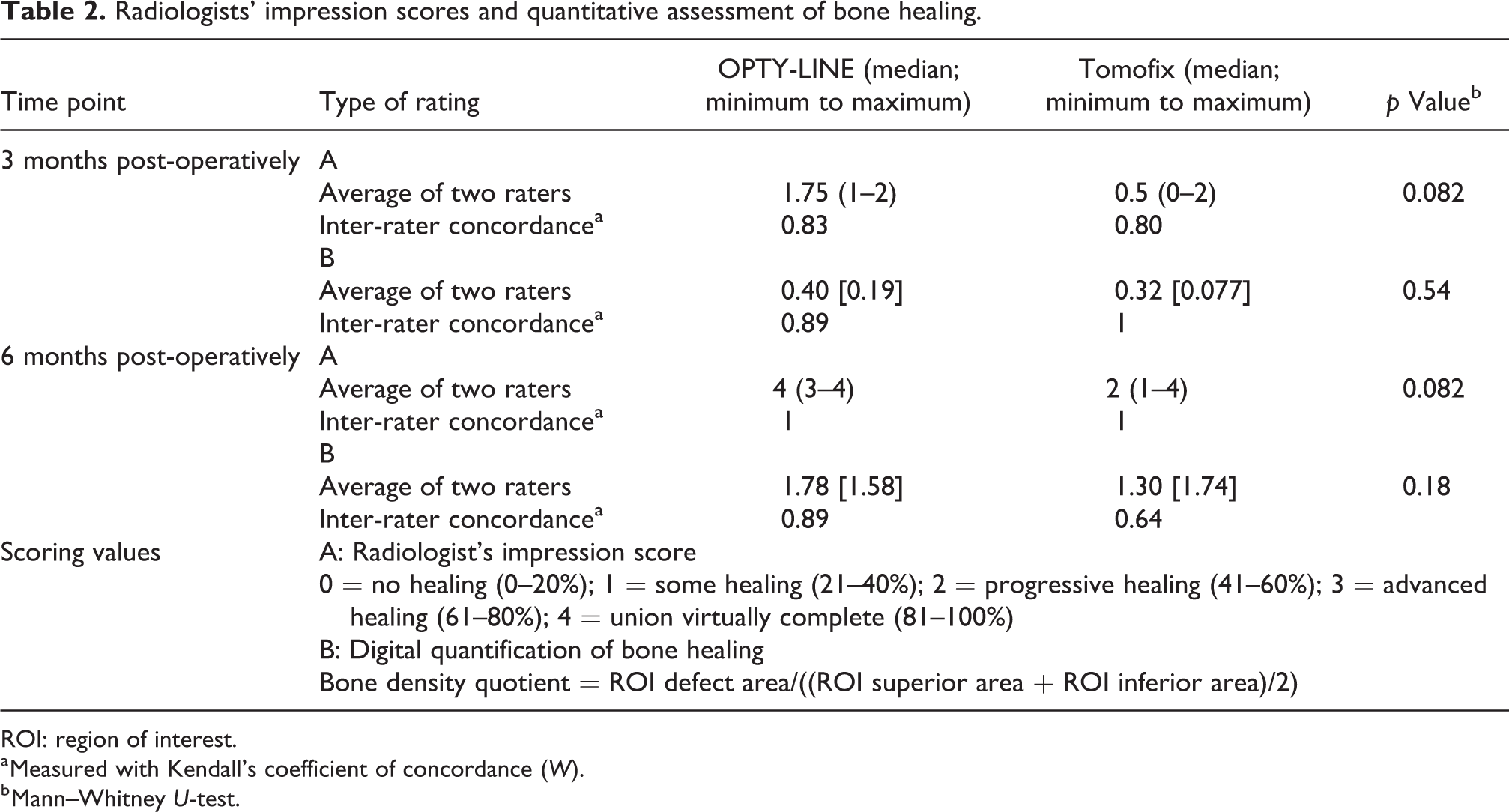
ROI: region of interest.
a Measured with Kendall’s coefficient of concordance (W).
b Mann–Whitney U-test.
The CT apparatus used in this study was a Siemens somatom sensation (64 slice) scanner. To minimize unnecessary exposure to ionizing radiation, the image acquisition will start 3 cm above the proximal osteotomy line and ending 3 cm below the inferior aspect of the gap. A standardized CT protocol with full detector coverage of 64 slices, a slice thickness of 0.6 mm, peak voltage of 120 kV, product of tube current and exposure time of 140 mAs effective and a pitch of 0.9 with a rotation time of 1 s was used. Images were then reconstructed with very sharp kernel of B70s in 2 mm slices with a reconstruction increment of 2 mm. In addition to the aforementioned radiologist impression score, other parameters related to bone healing following HTO were recorded. The osteotomy margin is the angle between the superior osteotomy margin and the articular surface of the medial tibia plateau. In addition, the margin surface appearance was also recorded (smooth vs. irregular). The osteotomy gap is the maximum gap within the osteotomy location, measured at the cortex on a coronal field of view. Callus characteristics were also defined for each subject; callus appearance can be divided into irritation callus and fixation callus respectively. 21 The presence of endosteal and periosteal bone healing was also recorded. In addition to a qualitative bone healing scoring, bone healing was also quantified by applying regions of interest (ROIs), measuring approximately 7 mm2 in size. This quantitative measurement was performed within the osteotomy gap on coronal reconstruction images on the picture archiving and communication system (PACS). The location of the ROI was as follows: for the defect area, the ROI was positioned in the centre of the osteotomy gap between the superior and the inferior margins a few millimetres beside the medial cortex of the proximal tibia, and for inferior/superior areas, it was placed around 10 mm from the respective osteotomy margins. The purpose of measuring the ROI above and below the level of the osteotomy gap was to deliver references of normal bone marrow density of tibia of the same individual. Bone density of the callus formation was assessed independently by the two abovementioned radiologists, with each using the same coronal midpoint slide.
Statistical analysis
Study data were entered in Microsoft Excel, and analyses were conducted using SPSS v20. The a priori power calculation was performed using GPower 3.1 freeware. Since this concerns a first pilot study on the application of the OPTY-LINE nail, no formal power calculation was performed to determine a required sample size a priori. For comparison of quantitative assessment of bone formation between Tomofix and OPTY-LINE cohorts, Mann–Whitney U test was also applied. Concordance between the two radiologists’ scores was assessed with Kendall’s coefficient of concordance. Any statistical difference between the baseline demographics of the two cohorts for demographics was assessed with two-sided Mann–Whitney test for ordinal and continuous data, and Fisher’s exact test for binary data. KOOS patient-reported outcome data and magnitude of error of accuracy was assessed by the application of a two-sided Mann–Whitney U test. Lost to follow-up was not taken into account, as subjects were to remain under clinical supervision by the Orthopaedic department during the study period.
Results
Table 2 displays the data for the Likert scale radiologist’s impression score and also for the quantitative analysis using pixel density on images in PACS. The average bone healing status for OPTY-LINE at 6 months is ‘union virtually complete’, whereas for Tomofix it is ‘progressive healing’. These results are mirrored to a large extent with digital quantification analysis at 6 months. The characteristics of the regeneration in the lesion align with the radiologist impression score. At 6 months, four of the six OPTY-LINE cases show the presence of fixation callus, whereas this type of more developed callus is only seen in one of the five Tomofix cases. In all other cases, irritation callus is the predominant feature. Figure 2 shows representative CT imaging for one Tomofix and one OPTY-LINE patient at 3 and 6 months post-operative, respectively. CT imaging also revealed four of the six type I and one of the six type II hinge fractures in the OPTY-LINE cohort, whereas in the Tomofix cohort three of the five patients had a type I and two of the five had a type II hinge fracture.

Representative coronal imaging of osteotomy lesions at 3 and 6 months post-surgery. With both Tomofix and OPTY-LINE devices, there is an increase in callus formation is observed when the two post-surgical time points of 3 and 6 months are compared (a vs. b and c vs. d), respectively. At 3 and 6 months the healing for Tomofix cases compared to OPTY-LINE is less pronounced at particularly the medial edge of the osteotomy gap (a vs. c and b vs. d, respectively). (a) OPTY-LINE at 3 months, (b) OPTY-LINE at 6 months, (c) Tomofix at 3 months, and (d) Tomofix at 6 months.
The surgical accuracy achieved for each patient, and comparison analysis between the two cohorts, is summarized in Table 3. The OPTY-LINE device achieved a median improvement of more than 10 points – equating to achieving a minimal perceptible clinical improvement (MPCI) 16 – for each of the KOOS sub-scales, which are pain, symptoms (activities of daily living (ADL), sport & recreation (S&R), and quality of life (QoL). KOOS score improvements were also observed in the Tomofix cohort, with S&R and QoL reaching MPCI levels. An initial descriptive patient-reported satisfaction appraisal of each respective treatment shows little to no difference in how they perceive the outcome of the surgery (see Online Supplemental Appendix 1 for full graph summarizing outcomes at 3 and 6 months post-surgery). At 6 months, both OPTY-LINE and Tomofix score a median of ‘satisfied’ for general and pain-related patient satisfaction, whereas for daily activities and S&R they both score ‘neutral’. The data to some extent mirror the KOOS data. For none of the five sub-scales of the KOOS questionnaire there was a significant difference in change between baseline and 6 months post-operatively when OPTY-LINE and Tomofix cohort results were compared. The respective changes in KOOS sub-scale scores over 6 months were 17 versus 8 for pain (p value 0.54, Mann–Whitney U test), 14 versus 3 for symptoms (0.54), 18 versus 6 for ADL (0.082), 38 versus 24 for S&R (0.18) and 22 versus 15 for QoL (0.79). The full data set for KOOS scores is available in Online Supplemental Appendix 2.
Analysis of achieved versus intended Mikulicz at 3 and 6 months follow-up.

a A value of 0 equates to accuracy of 100% (achieved Mikulicz – intended Mikulicz (Elson, 2017)).
b Mann–Whitney U test.
When compared, of note is the difference in terms of the KOOS score at baseline for OPTY-LINE versus Tomofix (p value, Mann–Whitney U test): pain 68 versus 44 (0.052), symptoms 58 versus 41 (0.009), ADL 71 versus 47 (0.052), S&R 22 versus 6 (0.13) and 32 versus 20 (0.33).
Discussion
This is the first proof-of-concept report on the use and short- to medium-term performance of the OPTY-LINE nail in HTO, in a non-randomized case series comparing its clinical, radiological and patient-reported performance versus the established Tomofix plate device. Initial impressions are that the performance of OPTY-LINE is non-inferior equivalent to that of Tomofix, though the sample size used does not allow for concrete conclusions to be drawn. Through radiological assessment, the rate of bone regeneration in the osteotomy gap and healing at 6 months in OPTY-LINE shows promise. Although the application of the OPTY-LINE device in patients with osteoarthritis is novel, the applied technology is well-established. It has its roots in the PRECICE intramedullary limb lengthening system; a magnetic rod and a motorized external remote controller with rotational magnetic field are used to gradually extend the limb. 22 The PRECICE system has been shown to be highly accurate in terms of achieving a desired lengthening. 22,23
The gradual elongation with OPTY-LINE also allows fine-tuning of the MiKulicz correction axis point, whereas with Tomofix the surgeon is dependent purely on preoperative imaging and calculations to try and achieve an as accurate as possible correction. Data from our comparative case series evaluation hint that this may be worth exploring further in a larger, ideally randomized controlled, trial. In our cohorts, where three of the five Tomofix cases have an absolute surgical accuracy of <10, in the case of OPTY-LINE all cases are within 10. The range of corrections seen in the Tomofix cohort is not uncommon for HTOs conducted with said device. 15 At 3 months post-surgery both cohorts contain undercorrected and overcorrected cases. On the other hand, at 6 months, there are signs – in five of six cases – that the corrections for OPTY-LINE are not sustained and that there may have been a degree of compression of the osteotomy gap. More cases need to be carried out to ascertain if this is an accidental observation or whether this is a characteristic of the OPTY-LINE device which needs to be taken into account when planning surgery. Loss of correction has previously been shown to be a rarity in HTOs carried out using Tomofix, with only up to 2% of cases showing such signs. 24,25
Regardless of the medical device system applied, for open-wedged HTO it is imperative that the open wedge is healed and repopulated by new bone, to restore strength and allow full recovery following HTO. Regeneration will take place naturally, although some surgeons apply aids to promote bone healing, such as allografts or synthetic bone substitutes. Research into filling of the wedge has shown that there is no significant advantage to using the filler – both in terms of stability and in terms of bone healing time of the wedge. 16,26 Therefore, in this present study, for the Tomofix, cohort filler was not applied; with OPTY-LINE, since initially only the cut is made and a wedge is created in the weeks post-surgery, filler is not indicated. The option of introducing, for example, a bone graft into a Tomofix osteotomy gap does imply that any future studies that focus on bone regeneration could consider comparing OPTY-LINE against both Tomofix with and without filler. As mentioned in the introduction, osteotomy patients often wish to return to being physically active, including participation in sports. However, surgeons often find it very difficult to decide when their patient can indeed return to unrestricted sports. This is partially because it is often very difficult to quantify the bone healing process precisely on radiographs. Experiments on osteotomy cases and in other mammals have shown that CT imaging is the best option for appraising healing since radiography overestimates the degree of healing. 27,28 The radiologist impression scores and quantitative bone healing quotient scores using CT imaging were highly comparable at 3 and 6 months for each medical device, though lower concordance was found at 6 months, where the standard deviation was much larger for bone healing quotients. This can be explained by the fact that the radiologist impression score is based on an evaluation of the whole lesion, whereas for the digital quantification only one sub-region was captured. Due to the nature of healing, there may be ‘hotspots’ of healing with callus foci distorting the actual average degree of the new bone formed. Although each patient’s natural bone density was taken into account, this artefact could not be avoided because the selected region was in a consistent position within the gap to avoid selection bias. On the other hand, human interpretation of bone regeneration may introduce bias due to the subjective (human assessment) nature of the assessment. There are some signs of this at 3 months, with slightly poor concordance observed for this time point. Inter-rater concordance was higher for the 6-months samples. Therefore, in each of the bone regeneration appraisal techniques used, radiologist impression score and bone healing quotient has a flaw. The combined application of the two approaches is warranted because they corroborate each other. With the assessment techniques in mind, the osteotomy gap in patients fitted with the OPTY-LINE device healed at least as well as those fitted with Tomofix. On average, virtually complete regeneration at 6 months is achieved with OPTY-LINE with the cohort in this study; in the case of Tomofix, the healing time stretched beyond 6 months post-surgery for this case series. Due to the non-randomized nature of this study, and, for example, the fact that Tomofix patients had poorer knee function at baseline, one can only conclude that these are encouraging results for the OPTY-LINE device, rather than firm evidence that bone regeneration is superior over Tomofix. Previous research has shown that even at 1 year post-surgery, consolidation of the wedge created with a Tomofix fixed plate is complete in just under 90% of cases. 28 Of note is where OPTY-LINE regeneration is observed in the lesion; callus formation is seen in both the lateral and the medial compartments (see Figure 2(a) and (b)). On the other hand, in line with what has previously been reported, the Tomofix osteotomy gap is repopulated from the lateral side (Figure 2(c) and (d)), beginning at the hinge point where the distance between the existing bone is the least. 28,29 There is a body of evidence supporting the notion that smaller osteotomy gaps heal faster than large gaps. 30,31 Due to the gradual enlargement of the osteotomy gap, OPTY-LINE lesions can take advantage of this phenomenon. Furthermore, internal fixation with a degree of flexibility encourages bone healing and maturation, resulting in more callus formation. 32 This may possibly explain why healing in the OPTY-LINE cases is showing signs of promise. Schröter and colleagues previously showed that unstable hinge fractures and smoking may delay bone healing. 32 All the subjects in this study were non-smokers, and therefore, this does not pose an issue in terms of potential confounding. As expected, using CT in preference to radiography, a diagnosis of at least a type I fracture was made almost universally, and three type II fractures were also observed; distribution of the fractures was not skewed to one cohort in particular. The occurrence of the fractures add to the caution that needs to be taken in extracting firm conclusions on any difference in performance between the OPTY-LINE nail and Tomofix plate.
Despite this being a prospective, clinically and demographically matched comparison of OPTY-LINE and Tomofix, medical device allocation was not random. None of the staff, including the reporting radiologists, where blinded to the intervention. Furthermore, there was no controlling for KOOS score at baseline, particularly pain before surgery, and in the resulting analysis, it transpired that there was a significant difference in the said scores between the two cohorts at baseline. This covariate may introduce a degree of bias in terms of patient-related outcome measures post-operatively and possibly even closure of the osteotomy gap if there are biomechanical reasons underpinning the poor KOOS scores. In contrast, OPTY-LINE patients were marginally older on average. Potential bias and the small sample size limit the conclusions that can be drawn on the relative effects each device can have on patients’ pain, QoL, and ability to engage in ADL and sports. A future definitive trial will need to address these potential shortcomings, through the introduction of randomization and stratification for KOOS score. Nonetheless, it appears that OPTY-LINE patients are as ‘satisfied’ as Tomofix patients with the procedure at 6 months post-operation. The trend seen at 3 months for patient satisfaction, with a possibly a poorer performance for OPTY-LINE, may reflect the nature of the new device. OPTY-LINE patients need to undergo the daily elongation procedure for up to 6 weeks after surgery, whereas Tomofix patients have effectively completed their correction once off the operating table. Since a lot of patients do not return to playing sports after more than 6 months following HTO, 4,5,9 the potential impact of OPTY-LINE on return to physical activity was not assessed in detail in this proof of concept study due to the limited follow-up period. Nonetheless, both OPTY-LINE and Tomofix patients achieved an MPCI at 6 months in terms of KOOS sports sub-score. The ‘neutral’ score in terms of patient satisfaction for both devices indicates that it is possibly too early to gauge opinion on this specific topic at 6 months post-surgery.
Conclusions
The OPTY-LINE medical device is a new modality for high tibial open-wedge osteotomy in which post-operative distraction of the osteotomy cut creates a wedge that can be fine-tuned in terms of gap and thereby correction angle. The initial performance results in this proof of concept study indicate that the device facilitates bone regeneration, surgical accuracy and patient satisfaction to at least a level achieved with the more established Tomofix device for HTO. More definitive trials that involve a longer post-operative follow-up period are indicated to evaluate the performance of OPTY-LINE.
Footnotes
Acknowledgements
The authors thank Ms Hannah Crowther, Research Practitioner, North Cumbria University Hospitals NHS Trust; Dr Pregash Ellappardja, Orthopaedic Training Fellow, North Cumbria University Hospitals NHS Trust; and Dr Aiman Khunda, Orthopaedic Training Fellow, North Cumbria University Hospitals NHS Trust, for their help.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MD has received honoraria from Nuvasive for conference presentations. The other authors have no conflict of interest to declare.
Ethical approval
Ethics approval was obtained from the UK’s National Research Ethics Service, North-West Lancaster Committee (reference 16/NW/0017).
Informed consent
Written informed consent was obtained from all participants in accordance with the Declaration of Helsinki (Good Clinical Practice), as part of the study protocol.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was sponsored and funded by Nuvasive Specialized Orthopedics, Inc., San Diego, California, USA.