
Abstract
Objective:
The objective of this study was to examine the clinical and magnetic resonance imaging (MRI) outcomes of extensive tenosynovectomy on patients with diffuse flexor hallucis longus tenosynovitis combined with effusion (DFHLT-E).
Methods:
Consecutive patients undergoing extensive tenosynovectomy for DFHLT-E in the same foot and ankle center from January 2013 to December 2016 were selected; a total of 14 patients were included in the final analysis. Patients with a minimum 1-year follow-up were evaluated with physical examination, MRI, American Orthopaedic Foot and Ankle Society (AOFAS) clinical midfoot scale, and visual analog scale (VAS) pain scores.
Results:
The 14 patients were followed up for an average of 15.0 ± 2.3 months (12–18 months). There were no recurrences in all clinical examinations at the final follow-up. The AOFAS score was improved from 61.57 ± 10.70 before surgery to 90.28 ± 9.41 at the final follow-up. The difference was statistically significant (p = 0.001). The VAS score was improved from 4.00 ± 0.82 before surgery to 0.43 ± 0.53 at the final follow-up (p < 0.001). MRI examination revealed two patients with small residual and limited effusion with no clinical symptoms. Superficial pin infection was observed in one patient, and two patients had transient neurostimulation.
Conclusions:
Extensive tenosynovectomy is an effective alternative for the treatment of DFHLT-E with less complications or recurrence.
Introduction
Flexor hallucis longus (FHL) tenosynovitis (FHLT) with effusion (FHLT-E) is a disease caused by excessive secretion of synovial fluid from the inflamed tendon sheath. It occurs in people who have a history of foot and toe strain, such as actresses engaged in ballet performances, while relatively rare in the general population. 1 –3 It is different from FHLT tenosynovitis, which is usually a local lesion and the most common site of it is within the fibrous–osseous tunnel posterior to the medial malleolus. 3 Its clinical manifestations are diverse, and some cases manifest inaccurate ankle discomfort and pain. Michelson and Dunn 1 reported 81 patients with diffuse pain in the middle and posterior foot, most of whom were misdiagnosed as “plantar fasciitis” and then underwent erroneous treatment; some cases manifest local symptoms; Lui 4 once reported a group of patients with nail prick injury-caused FHLT and the first metatarsophalangeal synovitis, which manifested swelling and pain at the distal end of the first metatarsophalangeal joint; some cases have no clinical symptoms. Lohman et al. 5 used magnetic resonance imaging (MRI) and observed asymptomatic sheath effusion of FHL after long-distance running in healthy people.
Because swelling and pain may appear at the lesions of FHL or tendon sheath of any area, and the signs are often lack of specificity, so sometimes, lesions of the FHL or tendon sheath at the ankle level can be expressed as swelling and pain in the big toe, which is easily misdiagnosed and mistreated, and the recurrence rate is high. Such cases are rarely reported. 1,6 In recent years, we performed extensive tenosynovectomy through open surgery to treat such cases. The treatment effects are observed and summarized in this article.
Materials and methods
Patients
Between January 2013 and December 2016, a total of 14 consecutive patients with flexor hallucis longus tenosynovitis combined with effusion (DFHLT-E) around the tendon were retrospectively evaluated. All patients had failed conservative treatment, including medication and restriction of foot activity for at least 3 months, with no effective relief of clinical symptoms, such as foot swelling and pain. All the patients were performed extensive tenosynovectomy. DFHLT-E is defined as pain and tenderness in ankle(s), mass(es), or sinus tract in the foot sole or hallux, which may become bigger or effuse when being squeezed. There were 4 men and 10 women with a mean age of 57.1 years (37–76). Six patients had right-sided and eight had left-sided involvement. The mean follow-up was 15.0 (12–18) months, and no patient was lost during the follow-up. The mean preoperative American Orthopaedic Foot and Ankle Society (AOFAS) clinical midfoot scale 7 and visual analog scale (VAS) pain scores were 61.57 ± 10.70 (range 52–80) and 4.0 ± 0.82 (range 3–5), respectively.
Preoperative MRI confirmed the presence of DFHLT-E. According to the zonation of FHL by Lui, 8 zone 1 is located between the tendon–muscle belly junctional zone and sustentaculum tali, zone 2 is located between the sustentaculum tali and the Henry nodule of foot sole, and zone 3 is located at the distal end of the Henry nodule until the end point of the phalanx of FHL. All the 14 patients had effusion in zone 3 connecting with the toe mass or sinus tract. Among the patients, three patients had hydrops simply in zone 3, six patients had hydrops in zones 2 and 3, and four patients had hydrops in zones 2 and 3.
Pain was not consistent with MRI performance. The most common site of pain was the plantar midfoot (zone 2, 10 of 14 patients). Others presented with pain located at either the sesamoid complex in the plantar (zone 3, 5 of 14 patients) or the posteromedial ankle (zone 1, 4 of 14 patients). In five patients, pain was present in two locations.
Five patients were misdiagnosed as “local cyst of the big toe” and two patients were misdiagnosed as “local infection” previously. Nine patients had undergone focal debridement one to six times, three patients had undergone focal puncture of lesions one to four times; possible related foot and ankle disease included severe ankle sprain in three patients, flat foot in two patients, os trigonum in three patients, and talipes cavus in one patient. Possible systemic diseases included rheumatoid arthritis in one patient and diabetes in two patients. The preoperative basic information and possible related occupation of all patients are presented in Table 1.
Basic preoperative data of the 14 patients.

M: male; F: female; MRI: magnetic resonance imaging.
All the patients signed informed consent and were treated with the approval of the hospital ethics committee.
Operation procedure
Routine laboratory tests were performed before surgery to rule out surgical contraindications. All the surgeries were performed by the first author of this article, who also simultaneously guided another attending physician with 10 years of work experience. After epidural anesthesia, each patient was placed in a supine position with a tourniquet on the proximal thigh. The surgical incisions were designed based on the range of tenosynovitis and effusion found by MRI (1.5 T). According to the zoning rules by Lui, 8 10 patients had the incision being located in zone 3 (the nonweight-bearing area of the medial side of the arch), two patients had the incision being located in zone 3 extending to the proximal side until zone 2, and two patients had the incision being located in zones 1 and 2 (the posterior side of the fistula) because their MRI results showed that the effusion was mainly located between the planta of sustentaculum tali and the backside of talus.
In zone 3 (the nonweight-bearing area of the medial side of the arch), the incision passed through plantar fat layer, plantar fascia layer (penetrating deeply from the medial edge), and flexor digitorum brevis layer, freed and retracted the medial plantar nerve and distal lateral foot sole nerve to fully reveal the pachyntic tendinous sheath of FHL until the proximal side of the hallux sesamoid bone at the distal side and the Henry nodule area at the proximal side. If necessary, the incision can be extended proximally to reveal the tendinous sheath of FHL in zone 2. The incision in zones 1 and 2 was located on the posterior side of the fistula, which carefully cut open the skin and subcutaneous fat layer, after the vascular nerve bundle on the posterior side of FHL was revealed and retracted for protection, the incision can be extended backward to reveal the lesion on the posterior side of FHL and extended proximally to reveal the internodal groove on the posterior side of the talus.
DFHL hypertrophy and filling was obvious in all the patients, and clear jelly-like or thin synovial fluid can overflow from the distal side of the hallux sinus or the big toe mass exhibited a significant increase when the lesion was squeezed. The tendon sheath in the surgical field was completely removed for pathological examination. The FHL was observed carefully, and the synovial tissue attached to the tendon and the surface of the tendon were removed until the tendon became bright. Small curette was used to scrape the nonrevealed tendon sheath between the distal part of the sesamoid and the skin sinus (the load-bearing area that the incision should avoid), followed by saline rinsing. The patient with longitudinal fissure was trimmed and sutured, and the patient with a preoperative significant decrease of flexor muscle strength was intraoperatively explored and confirmed that the FHL was loose and then sutured to restore the tension. There was no necessity for treatment of the skin sinus that was already present before surgery. Absorbable thread was used to suture the plantar fascia and subcutaneous layers, followed by closing the incision and placing the drainage strip. The tendinous sheath removed during surgery was sent for pathological examination. Two typical cases are shown in Figures 1 to 3.

Patient 1, female, 76-year-old, with the main complaint as repeated mass rupture and forming a sinus on the plantar side of the right toe. She was performed local lesion removal once and puncture-drainage twice. (a) Preoperative posture image, (b) the surgical incision was designed in the nonweight-bearing area of the medial side of the arch along the projection of the FHL (the distal half of zone 2 and the proximal half of zone 3), (c) the epidermis around the FHL sinus has been peeled off, which reveals a thin capsule that bulges from the deep part that envelops the clear synovial fluid, (d) the FHL tendon sheath in the field has been completely removed, which reveals obvious diffuse filling, (e) the tendon sheath in the field has been completely removed and the FHL is explored, (f) one small curette is used to remove the tendon sheath in the weight-bearing area of the first metatarsal region, and this incision should avoid the involvement of the weight-bearing area. (g) and (h) Review in month 18 reveals that the original hallux sinus recovers well and the muscle strength of FHL is normal. (i) the tendon sheath tissue removed during surgery for pathological examination reveals hyperplasia of the fibrous connective tissue of the cyst wall and mucus degeneration in the outer space of the fibrous capsule, which are consistent with the signs of tenosynovitis (HE ×100). FHL: flexor hallucis longus.

MRI images (1.5 T) before surgery and 1 year after surgery. Preoperative MRI T2WI antilipid sequence: (a) the axial view, (b) the sagittal view, and (c) the coronal view of the foot show effusion in the tendon sheath of FHL, and high-signal fluid surrounded by FHL in the low signal range of the mid-forefoot range, the distal side of which is connected to the toe lesion. Postoperative 1-year MRI T2WI antilipid sequence: (d) the axial view, (e) the sagittal view, and (f) the coronal view of the foot show no obvious effusion around the FHL. FHL: flexor hallucis longus; MRI: magnetic resonance imaging.

Patient 6, female, 65-year-old, with more concealing clinical manifestation. The main complaint is repeated mass on the dorsal side of the left toe. The patient had a history of three-time left toe lesion clearance and puncture drainage once. (a) Physical examination reveals diffuse mass on the dorsal side of the big toe. (b) and (c) The dorsal metacarpal fossa is confirmed intraoperatively to be connected to the deep part of FHL tendon sheath through the lacunar space. (d) The deep part of the cavity is closed by ligation. (e) The incision in zone 2 shows diffuse hypertrophic FHL tendon sheath, which is completely removed. (f) and (g) Review in month 18 reveals no recurrence of the mass on the dorsal metacarpal toe and the FHL muscle strength is normal. (h) The pathological examination results of the removed tendon sheath tissue reveals hyperplasia of fibrous connective tissue (HE ×100). FHL: flexor hallucis longus.
Postoperatively, elastic bandage compression was used to reduce bleeding, control swelling, and prevent deep vein thrombosis. The drainage strip was removed 24 h later, and the maximum-range passive flexion and extension of FHL started 1 week after surgery, active activity was encouraged 2 weeks after surgery, weight-bearing walking of the foot gradually began 3 weeks later, and weight-bearing walking stick-free activity started in 6 weeks.
Clinical and radiological analysis
The surgeons in charge of the surgery reviewed the patients in months 1, 3, 6, and 12. At the time of follow-up, each patient’s foot swelling, pain, or numbness was recorded, together with the incision scar, plantar sensation, toe activity range, and muscle strength. The patients were also guided the weight and toe strength training. The AOFAS clinical midfoot scale was used to evaluate the function of the foot at the final follow-up, and the VAS score was used for pain assessment.
MRI (1.5 T) was performed at the 12-month follow-up to observe the shape of FHL and whether the surrounding effusion recurred.
Statistical analysis
The data were statistically analyzed using SPSS 19.0 (SPSS, Chicago, Illinois, USA). The AOFAS midfoot scores and VAS scores before and after surgery were analyzed by the paired t-test, with p < 0.05 being considered as statistical significance.
Results
General information
All the 14 patients were followed up for an average of 15.0 ± 2.3 months (12–18 months). At the final follow-up, no obvious swelling, tenderness, or fluctuation sensation existed in any of the patients. The preoperatively existing sinus completely healed, and all the patients had no recurrence sign and returned to normal work and life. All the patients were satisfied with the treatment effect.
Pathological outcome
Intraoperative removal of tendinous sheath tissue for pathological examination exhibited hyperplasia of the fibrous wall connective tissue and mucus degeneration in the outer space of the fibrous capsule wall, which were all consistent with the signs of tenosynovitis, so other diseases can be ruled out.
Clinical score
The AOFAS score was improved from preoperative 61.57 ± 10.70 to 90.28 ± 9.41 at the final follow-up, and the difference was statistically significant (p = 0.001); four patients completely recovered the normal function (AOFAS score: 100 points); the VAS score (4.00 ± 0.82 before surgery) was improved to 0.43 ± 0.53 at the final follow-up (p < 0.001), and the difference was statistically significant (Table 2).
Comparison of AOFAS and VAS scores of the 14 patients before and after surgery.
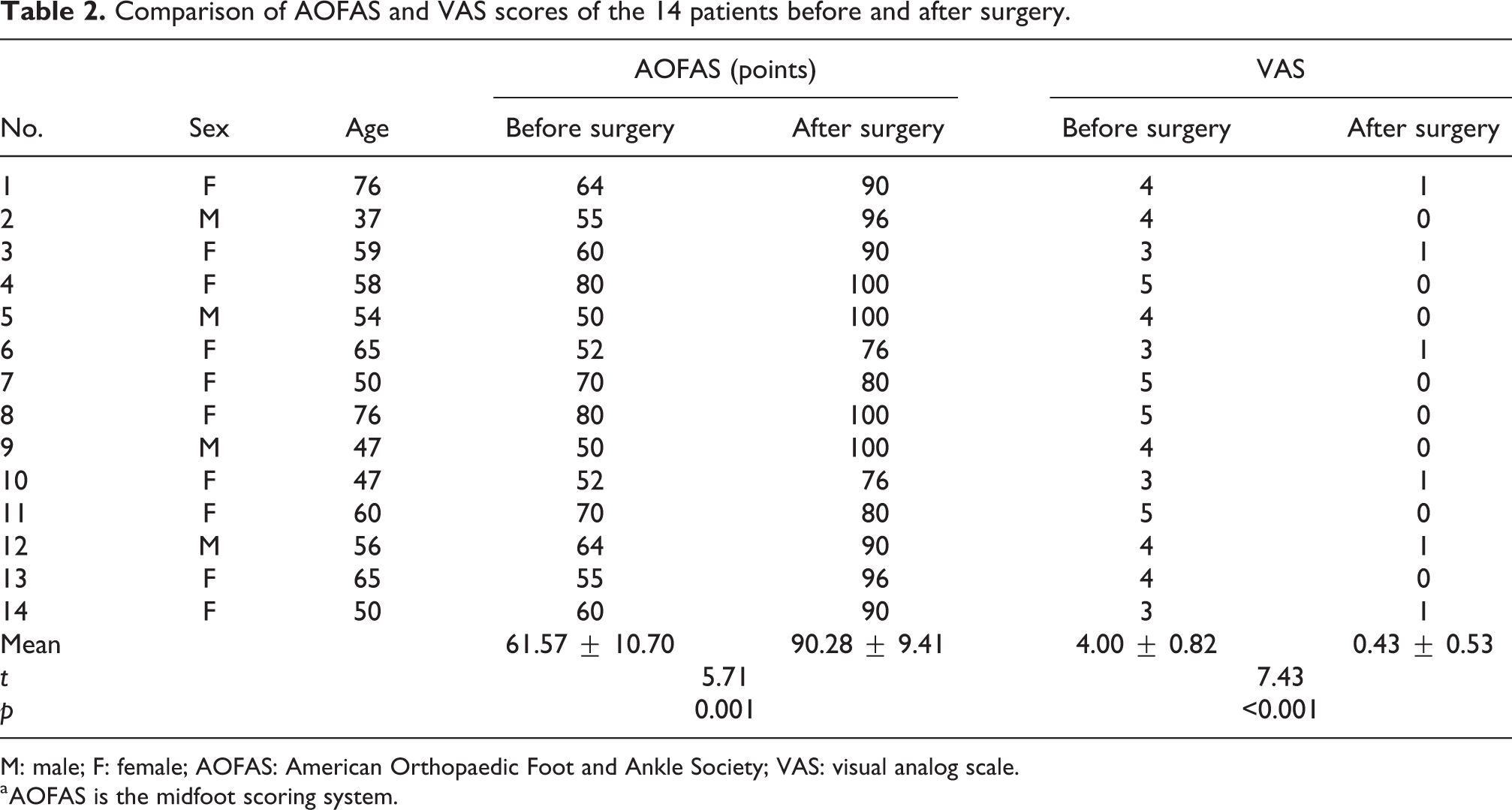
M: male; F: female; AOFAS: American Orthopaedic Foot and Ankle Society; VAS: visual analog scale.
a AOFAS is the midfoot scoring system.
Radiological evaluation
MRI (1.5 T) of 1 year after surgery revealed small residual local effusion, with no clinical symptoms in two patients. All the patients recovered the normal shape of FHL. The patient with longitudinal fissure exhibited normal MRI signals of FHL, and the patient who was performed intraoperative loose FHL shortening and suture exhibited no obvious disorder of MRI signals at the suture site.
Complications
Superficial pin infection was observed in one patient, which was relieved by partial incision suture removal and redressing, and no deep infection occurred. There were two cases of transient neurostimulation, which showed numbness and sensory dysfunction of the big toe and was considered to be caused by intraoperative traction, but these cases recovered 6 weeks after surgery.
Discussion
The clinical manifestations of FHLT-E are often lack of specificity. Most of the previously reported cases are just local lesions, and most of the patients have a history of big toe trauma or special occupations such as ballerinas or professional athletes, who have tendon sheath stenosis and wedge pressure-caused tendon sliding disorder, so it can be easily diagnosed. 4,9,10 Another type of easily identifiable case is the case combined with os trigonum and posterior malleolus impact, in which FHLT-E may be found coexisting during treating the posterior malleolus impact. 11,12
DFHLT-E is easily misdiagnosed for the following reasons. First, the clinical manifestations are diverse, and the pain position is not specific. In particular, the incidence of DFHLT-E at the distal end of Henry nodule in zone 1 is low (four patients in this study were involved in zone 1), and the clinical manifestations are more concealed. Michelson and Dunn 1 reported 81 cases of FHLT, most of which were misdiagnosed as plantar fasciitis. Second, the causes are complicated. The etiologies of FHLT-E reported previously, in addition to the excessive use of tendon, include acute tearing of tendon and tendon sheath, rheumatoid disease, or pigmented villus synovitis. 7 Third, inappropriate prophase treatment. Local puncture and lesion removal are often used to treat symptomatic cysts. Most of the patients in this study had undergone puncture and/or debridement before the surgery in our hospital, by which the integrity of the tendon sheath was further destroyed, thus making the diagnosis more difficult. In terms of diagnostic techniques, the author’s experience is to apply compression force from the proximal end to the distal end at the inner side of the plantar arch. When the distal mass is obviously enlarged or the sinus has fluid overflow, it should highly suspect the possibility of FHL effusion in zones 1 and 2.
MRI can confirm the diagnosis and is the most valuable noninvasive auxiliary examination for the observation of tendon tissue lesions. 13 For the case with swelling and tenderness in the extending direction of FHLT, especially the case with recurrence after puncture or lesion removal in the early stage, the possibility of FHLT-E should be suspected so as to give early MRI examination. The inflammatory signal changes in the tendon sheath are usually correlated with edema in the surrounding soft tissues, and T1-weighted postgadolinium injection sequences are particularly useful to distinguish the thick tenosynovium from the surrounding structures. 14
When treatment is required due to pain or appearance complaints caused by tenosynovitis and effusion, the most common conservative treatments are performed including nonsteroidal drugs and foot movement restriction. In our clinical data over the past decade, approximately 70% of the patients got clinical symptoms relieved after 3 months of conservative treatment. It should be noted that once the sinus tract is formed, conservative treatment is often ineffective and recurrence is hard to avoid. Tenosynovitis ineffective to conservative treatments was treated surgically to relieve the adhesions of tendons and remove the synovial membrane that secretes excessive synovial fluid. 1 Surgical treatment can be performed by open or myoscopic surgery. Because the tendon is deep, and the surrounding important blood vessels and nerves are adjacent, no matter which technique is employed, it is challenging to reveal the whole FHL and tendon sheath. 8 Arthroscopy or myoscopic surgery is mainly used to treat the lesions in zone 1, such as os trigonum and posterior malleolus impact syndrome, 15 while the lesions in zones 2 and 3 require specialized tendonoscopy, which is rarely used at present. Lui reported the microscopic treatment techniques of lesions in zone 2 and zone 3 and summarized its advantages and disadvantages: the advantage is that the small incision does not form painful scars in the weight-bearing area and the disadvantages include inadequate debridement, tendon and toe nerve damage, or infection spreading. 5,16 Keeling and Guyton 17 conducted a study of eight cadaveric specimens and found that the tibial nerve branches in zone 2 are closely adjacent and paralleled to FHL, so common arthroscopic instruments will be very easy to cause nerve damage. Whole arthroscopic treatment in zone 2 is believed to be more likely to damage the vessels and nerves than open surgery, and the tendon sheath of all the specimens in zone 2 failed to be completely removed by microscopic operation. Limited by equipment and technology, we still lack the experience of applying related microscopic techniques to remove FHL in zones 2 and 3.
Although open surgical treatment has larger incision, it has the advantage of clear revealing. The tendon can be retracted during surgery, so the tendon sheath in the field of incision can be fully removed, and the adjacent vessels and nerves can avoid injury under direct vision. The plantar side of the head of metatarsal is a weight-bearing area, so it is not advisable to design an incision in this area. Therefore, a small curette scraping is inserted into the tendon sheath in the distal part of zone 3 (the distal side of the big toe sesamoid) to remove the synovial membrane by scratching; although a small amount of inflammatory tendon sheath remains, the synovial fluid decreases significantly than that before surgery and cannot accumulate locally. The follow-up results also confirmed that the small amount of residual sacral sheath in the distal part of zone 3 did not cause recurrence. Therefore, it can be considered that extensive tenosynovectomy effectively avoided postoperative recurrence because it eliminated most inflamed tendon sheath, which significantly reduced the secretion of synovial fluid. Nine patients in this study had a history of recurrence after partial or multiple local lesion debridement, and it was considered to be related to the incomplete tendon sheath removal. The main disadvantage of open surgery is that it may cause large scars at the plantar side of the foot, leading to potential risk of scar pain.
Postoperative pathological examination is of great significance to exclude other diseases such as neoplastic diseases. All excised tendon sheath tissues were pathologically examined postoperatively. The results revealed obvious synovitis and confirmed the preoperative diagnosis of synovitis-caused synovial effusion.
DFHLT-E is difficult to diagnose before MRI examination. Most of the patients in this study experienced a puncture or local lesion removal before our surgical treatment without undergoing extensive tenosynovectomy and therefore resulted in recurrence. Such patients are also uncommon in our hospital and further accumulation of them is necessary. Although tendon sheath resection is the usual method for treatment of tendon sheath diseases and is widely used in the treatment of diseases in other parts, such as posterior tibial tendonitis, 18,19 there is still no report about the long-term effects of tendon sheath resection on FHL. We will continue to follow-up and observe the patients in this study. In addition, minimally invasive surgery is the developing trend of surgery. 20 Under the condition of being familiar with local anatomy and proficiency of the myoscopic technique, microscopic operation can significantly reduce the injury of the incision, which is conducive to early postoperative recovery, and we will actively try such techniques in our future work.
Conclusions
DFHLT-E is easily misdiagnosed. Once diagnosed by MRI, extensive tenosynovectomy is an effective alternative for the treatment of this disease with fewer postoperative complications and recurrence.
Footnotes
Authors’ note
Each author certifies that his institution has approved the human protocol for this investigation, that all the investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained from each participant.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.