
Abstract
Purpose:
Ankle arthroscopy has been used as a standard tool by foot and ankle surgeons. To overcome the narrowness of ankle joint, a noninvasive distraction technique is used for the successful visualization in ankle arthroscopy. The aim of this study was to investigate the incidence and type of complications associated with ankle arthroscopy using a noninvasive distraction technique and to report a troublesome complication.
Methods:
We reviewed 514 patients’ charts from 2003 to 2011. The same noninvasive distraction technique was used. Patients’ demography, duration of follow-up, diagnoses, procedures, and complications related to ankle arthroscopy were analyzed.
Results:
There were 388 male and 126 female; mean age was 37.2 years; mean follow-up duration was 33 months. The diagnoses were osteochondral lesion of talus, chronic ankle instability, anterolateral soft tissue impingement syndrome, and anterior bony impingement. We performed arthroscopic synovectomy, osteochondral procedure, bony spur excision, and loose body removal. The mean time of arthroscopic procedure was 47 min. There were neurologic complications (eight cases), skin necrosis of posterior thigh (three cases), instrument breakage (two cases), and superficial wound infection (one case). All complications were well resolved. The total duration of distraction plus tourniquet inflation exceeded 120 min in the three cases of skin necrosis. Skin necrosis was deemed to be resulted from the long tourniquet time.
Conclusion:
The noninvasive distraction technique is safe and effective for ankle arthroscopy. However, the distraction plus tourniquet requires attention because it can cause high pressure on posterior thigh resulting in soft tissue injury.
Introduction
Since Watanabe first introduced a no. 24 arthroscope for small joints in 1972, 1 ankle arthroscopy has been widely used as an indispensable tool for various ankle disorders. Ankle arthroscopy is particularly useful for treating the osteochondral lesion of the talus (OLT), excision of bony impingement spurs, and arthrodesis. 2 –4 To overcome the narrowness of the ankle joint, the joint distraction technique is important for successful visualization in ankle arthroscopy. Recently, there has been a shift from invasive to noninvasive distraction because the noninvasive distraction technique for ankle arthroscopy is safe and effective. 5 Non-neurologic complications could be reduced as well by exclusively utilizing noninvasive distraction. 6 Several studies have reported the complications of ankle arthroscopy, and neurologic injuries were the most common. 6 –16 Earlier studies reported higher rates of complications because the practice of ankle arthroscopy had not developed and many of these studies involved the use of invasive joint distraction devices.
In this study, we performed ankle arthroscopy for various ankle disorders using a noninvasive distraction technique. We hypothesized that the ankle arthroscopy using a noninvasive distraction technique is safe and effective. The purpose of the present study was to investigate the incidence and type of complications associated with ankle arthroscopy using a noninvasive distraction technique and to report a troublesome complication.
Methods
From March 2003 to February 2011, 514 patients who underwent ankle arthroscopy were consecutively included in this study. We undertook a review of patients’ chart. Patients with acute ankle fracture, systematic inflammatory arthritis, long-standing neuromuscular disease, or peripheral vascular disease were excluded. The cohort included 388 male (75%) and 126 female (25%) and had a mean age of 37.2 (range 12–73) years. The mean duration of follow-up was 33 (range 12–67) months, which started from February 2004 and ended on March 2012. The diagnoses of included patients were categorized and the various arthroscopic procedures were classified. The mean duration of the arthroscopic procedure and the mean duration of tourniquet inflation for open procedures were assessed. Complications were regarded as any unexpected conditions that resulted from the ankle arthroscopy itself and also from the patient’s position during the whole surgical process including an additional open procedure.
The patients’ chart review, data analysis, and surgery were performed by a senior author (JHA). The operative setup, surgical technique, assessments, and documentation were standardized by one surgeon and his assistant team. The assessment of radiographs, computed tomography, magnetic resonance imaging, and arthroscopic finding were done by corresponding author (YCK). The data abstract and outcome assessment were performed by other coauthors (DP, YTP, and JP). We did not seek Institutional Review Board (IRB) approval for this study because we did not employ the use of protected health information in this investigation.
Operative technique
Surgery was performed under general or spinal anesthesia. Arthroscopic procedures were performed via noninvasive distraction alone without thigh tourniquet inflation. The noninvasive distraction devices used were the FerkelTM Thigh Holder and Guhl® Non-invasive ankle distractor system (Smith and Nephew, Andover, Massachusetts, USA). The distraction device was applied with the patient in the supine position and with the hip and knee flexed 45° using a well-padded thigh holder. The foot was placed in a resterilizable strap around the midfoot and hindfoot (Figure 1). 17 In all procedures, a 2.7- or 2.4-mm 30° arthroscope was used.

The FerkelTM Thigh Holder and Guhl® non-invasive ankle distractor system (Smith and Nephew, Andover, Massachusetts, USA) were applied to the patient positioning 45° flexed hip and knee.
The arthroscopy was performed using three portals (anteromedial, anterolateral, and posterolateral portals) in most cases. Care was taken to avoid damage to the nerve branches, such as the superficial peroneal nerve, by delicately incising the skin alone without penetrating the subcutaneous tissues during portal placement. This “nick and spread” technique during portal placement is helpful for preventing nerve damage. The anteromedial portal was first established just medial to the tibialis anterior tendon because it is relatively easy to create and no major neurovascular structures exist at this point. The anterolateral portal was created lateral to the peroneus tertius tendon and care was taken to avoid the branches of the superficial peroneal nerve. The posterolateral portal was established 1–1.5 cm proximal to the tip of the lateral malleolus and just lateral to the achilles tendon, avoiding the course of the sural nerve. It mostly serves as an inflow portal allowing optimal visualization throughout the procedure. The portals were used interchangeably as viewing or working portals during the entire arthroscopic procedure. Other portals such as accessory anteromedial and accessory anterolateral portals were created as needed.
An automated pump system (Stryker® 1.5L High Flow Pump (Stryker Osteo GmbH, Mülheim, Germany)) was used during the arthroscopic procedures. The intraarticular fluid pressure was set at 50–80 mmHg. After completing the arthroscopic procedures, the distraction devices were all removed. Other open procedures were performed after the thigh tourniquet was inflated to 280–300 mmHg.
Statistical analysis
Since this study was an uncontrolled retrospective case series, the inferential statistical analysis was not performed. Simple descriptive statistics were used instead. This case series was attempted in an effort to minimize, or at least identify, potential biases according to a suggestion by Kempen. 18
Research ethics approval and patient consent
All patients provided written informed consent before surgery. Data were collected only from patient charts and electronic records. All patients provided written informed consent for publication. The authors did not employ the use of protected health information in this study.
Results
The most common diagnosis was OLT in 151 cases (22.9%), followed by chronic ankle instability in 137 cases (20.8%), anterolateral soft tissue impingement syndrome in 118 cases (17.9%), anterior bony impingement in 107 cases (16.3%), and there were many others as described in Table 1. The most common arthroscopic procedure was synovectomy in 382 cases (40.6%), followed by marrow stimulation procedures in 177 cases (18.8%), bony spur excision in 151 cases (16.0%), and loose body removal in 87 cases (9.2%; Table 2). The mean duration of the arthroscopic procedure was 47.0 min (range 15–117). The mean duration of tourniquet inflation was less than 100 min in all our cases.
Categorized diagnoses of the patients.

OLT: osteochondral lesion of talus.
aThe cohort consisted of 514 patients who underwent ankle arthroscopy in this study. However, one patient could have two or more diagnoses, so the total number of cases was larger than 514.
Types of arthroscopic procedure.
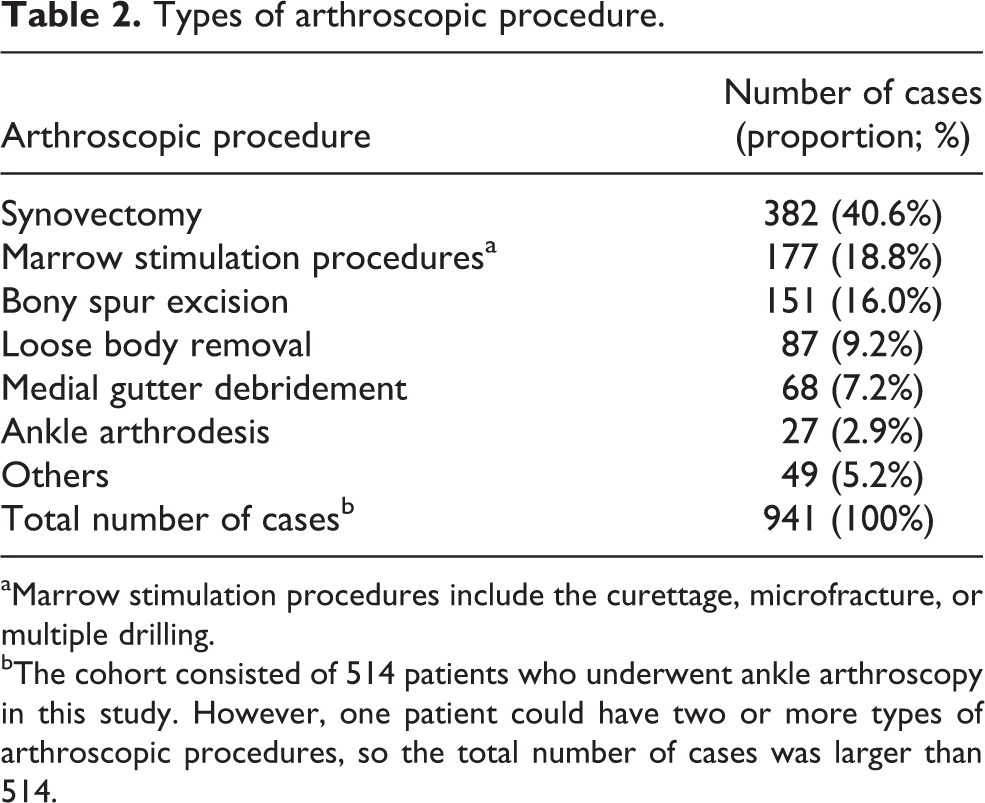
aMarrow stimulation procedures include the curettage, microfracture, or multiple drilling.
bThe cohort consisted of 514 patients who underwent ankle arthroscopy in this study. However, one patient could have two or more types of arthroscopic procedures, so the total number of cases was larger than 514.
Complications related to the ankle arthroscopy occurred in 14 of 514 patients (2.7%; Table 3). The most common complication was neuropraxia (eight cases; 1.6%). There were six cases (1.2%) of superficial peroneal nerve paresthesia, one case (0.2%) of deep peroneal nerve injury, and one case (0.2%) of sural nerve dysesthesia. Damage to the skin of the patient’s posterior thigh was noted (Figure 2) in three cases (0.6%). Patients with complications were analyzed in terms of demographics, the time of arthroscopic and open procedures, comorbidity, diagnosis, treatment, and clinical outcome (Table 4). The complication cohort included 11 male (79%) and three female (21%) and had a mean age of 39.0 (range 20–54) years. The mean duration of the arthroscopic procedure in complication cohort was 50.3 min (range 30–88). The mean duration of the open procedure was 30.2 min (range 0–95). One case of superficial peroneal nerve paresthesia did not improve until 1 year after surgery. Another one case of posterior thigh skin breakdown was treated with a split-thickness skin graft. The total duration of traction plus tourniquet inflation was over 120 min in the three patients who experienced skin damage of their thighs, because they underwent an additional open surgery such as subtalar ganglion excision, bone graft harvesting from distal tibia for OLT, and tarsal tunnel release, respectively. Two cases (0.4%) of arthroscopic instrument breakage (Figure 3) and one case (0.2%) of superficial wound infection were also recorded. Most complications were managed conservatively.
Complications related to the ankle arthroscopy.

SPN: superficial peroneal nerve; DPN: deep peroneal nerve.

An unexpected damage developed at the posterior thigh during the ankle arthroscopy. The wound was eventually treated with a split-thickness skin graft.
Patients with complications regarding demographics, the time of procedures, comorbidity, diagnosis, treatment, and clinical outcome.

A/S: arthroscopic; SPN: superficial peroneal nerve; DPN: deep peroneal nerve; OLT: osteochondral lesion of talus.

The broken chondral pick instrument was confirmed intraoperatively using an image intensifier.
Discussion
In 1931, Burman suggested that the ankle joint was unsuitable for arthroscopy because the ankle joint space is so narrow that even a very thin needle cannot be inserted into it. 19 However, the pioneers of ankle arthroscopy constantly strived to overcome this hurdle and reported favorable results with ankle arthroscopy thereafter. 1,5 The advent of arthroscopy has been accompanied by numerous benefits. 8 Similar to the expansion of arthroscopic applications to other joints such as the knee and shoulder, ankle arthroscopy has the potential to shorten recovery times and limit surgical morbidity compared to open arthrotomy. The currently acceptable indications for ankle arthroscopy include impingement (bone and soft tissue), osteochondral lesions, ankle arthrodesis, loose bodies, ankle instability, septic arthritis, arthrofibrosis, ankle osteoarthritis, synovitis, and fractures. 4,5,20 –22 To overcome Burman’s earlier concerns about the narrowness of the ankle joint space, the distraction technique was introduced as an important component of ankle arthroscopy. Earlier studies of ankle arthroscopy showed higher rates of complications, since the invasive distraction device was used in the early period of ankle arthroscopy. With the evolution of ankle arthroscopy, invasive distraction has been replaced with the noninvasive method. 6 The complications of ankle arthroscopy have been studied over the past decades, 7 –9,23 –27 and various complication rates ranging from 0.7% to 17% have been reported. 5 –7,9,28 Ferkel et al. 10 reported an overall 9.0% complication rate in 612 patients that underwent ankle arthroscopy using a noninvasive or invasive distractor. Nerve injury accounted for 49% of all complications and was the most common complication, occurring due to portal or distractor pin placement. 24 Young et al., 6 in a study of 294 consecutive ankle arthroscopies using a noninvasive distraction technique, reported an overall complication rate of 6.8%, and 80% of these were neurological in nature. In our study, the overall complication rate was 2.7% in 514 patients, which was lower than found in most previous reports. 6,15,16,24 Carlson and Ferkel 23 emphasized that portal placement is technically important for minimizing neurovascular injury. They recommended a “nick and spread” technique which we used in the current study. As the noninvasive distraction for ankle arthroscopy has been recommended for reducing complications in several recent studies, 6,23 we suggest that a noninvasive distraction technique for ankle arthroscopy is safe and effective. Other possible reasons for reducing complication rates of ankle arthroscopy over the years are the refined technique and the closer attention to structures at risk as well. Malagelada et al. 29 revealed that dedicated anatomic lectures and portal-related complications during ankle cadaveric courses can reduce the overall number of injuries especially superficial peroneal nerve, the commonest complication in ankle arthroscopy.
With the improvements in ankle arthroscopy, the procedure has become an important therapeutic tool for managing various ankle disorders. Many studies have reported good results after ankle arthroscopy. 2,30,31 Glazebrook et al. 4 suggested that the evidence-based indications for ankle arthroscopy were osteochondral procedure, bony spur excision, and arthrodesis. The authors also performed various arthroscopic procedures.
Many orthopedic surgeons routinely use a tourniquet for ankle arthroscopy to obtain a bloodless operative view. 32 Tourniquet use for less than 30 min during arthroscopic meniscectomy of knee does not affect postoperative pain, return to activities, and serious muscle damage. 33 Previous studies also reported that visualization was better with tourniquet inflation in knee arthroscopy. 34,35 However, the incidence of tourniquet-related complications increases as tourniquet time increases. 36 Tourniquet use is still associated with risks including neurovascular complications, muscle damage, and occasionally, severe deep venous thrombosis, pulmonary embolism, and cardiac arrest. 37,38 Johnson et al. 39 even recommended that the routine use of a tourniquet for knee arthroscopy might be discontinued. In 2005, Younger et al. 40 published the results of a survey on tourniquet use in foot and ankle surgery. They reported that many surgeons determined cuff pressure and time without explicit guidelines and even the most commonly used pressure ranges were higher than necessary for many patients. A prospective case–control study showed that ankle arthroscopy using the noninvasive distraction device without tourniquet inflation was technically feasible, without the reduction of operative visibility and without complications. 32 Fitzgibbons et al. 41 recommended principles and guidelines for safe tourniquet use regarding duration, pressure, and reperfusion period.
An automated pump or gravity flow system has the benefits of a tamponade effect on bleeding, an intraarticular irrigation effect, and a decreasing need for tourniquet use. 39,42 However, since the pump system can generate higher flow rates and pressures, more marked damage can occur. 39,43 Intraarticular fluid pressure increase via the pump system combined with the distraction force during arthroscopy should not be overlooked, even when arthroscopic procedures are performed without tourniquet inflation.
In the current study, we observed a quite rare but troublesome complication of skin necrosis of the patient’s posterior thigh. We assumed that it was associated with consecutive tourniquet use after ankle distraction, since we used the noninvasive distraction device with a well-padded thigh holder for the arthroscopic procedure and then performed open procedures with tourniquet inflation at the same time in some patients to treat combined foot and ankle disorders such as chronic ankle instability. Although the duration of tourniquet inflation was less than 100 min in all our cases, the total duration of traction plus tourniquet inflation exceeded 120 min in some cases. Young et al. 6 also noted a trend toward an increasing prevalence of neurologic complications as distraction time increased. They highlighted the importance of releasing the distraction as soon as possible and suggested decreasing the force of distraction to relax the soft tissue after approximately 1 h in prolonged procedures. Dowdy et al. 44 recommended noninvasive distraction in ankle arthroscopy with up to 135N of distraction for less than 1 h to safely evaluate the ankle. Our three cases of skin necrosis were not associated with neurologic complications and were all well treated without any serious sequelae. We suspect that the prolonged duration of mechanical compression due to the combined use of traction and tourniquet inflation can cause skin necrosis of the patient’s posterior thigh. The total duration of traction following tourniquet inflation exceptionally exceeded 120 min in the three cases of skin necrosis. Because the additional open procedures using tourniquet inflation after the arthroscopic procedure using the distractor were performed consecutively. In the earlier period of our study, we inflated the tourniquet for open procedures immediately after completing the arthroscopic procedure. Since our experience of these three cases of skin necrosis, we have precluded this complication by starting the open procedure for 20 min without tourniquet inflation. Thereafter, an interval of at least 20 min was routinely applied between the removal of the distractor and tourniquet inflation. No more skin complications occurred after this protocol. We propose that protecting the posterior thigh from prolonged pressure is very important to avoid inadvertent complications.
The ankle arthroscopy has become a standard surgical tool worldwide and it is universally accepted that the noninvasive distraction is necessary for ankle arthroscopy as of now. During clinical practice, we also encounter some patients who need an additional open procedure using tourniquet inflation as well as an arthroscopic procedure. We have thought that surgeons should beware of any accompanying complications related to ankle arthroscopy during the whole surgical process. However, most previous studies repetitively reported “arthroscopic procedure related” complications such as neurovascular, tendon, cartilage injuries, and known orthopedic postoperative complications such as deep vein thrombosis, portal wound infection, sinus tract formation, uncontrolled swelling, and complex regional pain syndrome. 45,46 Lozano-Calderón et al. 47 conducted a comparative prospective study and they suggested that a noninvasive distraction facilitated complete ankle arthroscopy. Our literature search during this study revealed that there are few published literatures about complications related to noninvasive distraction method. Although Zaidi et al. 32 stated that ankle arthroscopy is feasible without tourniquet inflation, they only focused on arthroscopic visibility and portal site complication, not the distractor or tourniquet related complications. To the best of our knowledge, there were no reports focusing on skin breakdown complication related to ankle arthroscopy with ankle distraction device and tourniquet inflation for the prolonged operation time up to now. Even though the posterior thigh skin breakdown is not a life-threatening complication, one of our patients should have been treated by skin graft eventually. In this regard, our study is distinguishable from the previous studies about complications related to ankle arthroscopy. Most previous literatures investigated surgical outcome from multicenter or from several surgeons’ data even in a single facility. 45 In our study, all patient data were collected from a single facility and all surgeries were performed by one surgeon who is a senior author of this article. We are convinced that this study design could make our data be more homogeneous and this is another strength of our study.
Our study had some limitations as well. First, it was a retrospective non-comparative cohort study. Second, the traction force across the ankle could not be quantified. With these limitations in mind, the high-quality randomized controlled trials or meta-analyses are needed to achieve a more robust consensus about the incidence and type of complications associated with ankle arthroscopy using a noninvasive distraction technique.
Conclusion
The ankle arthroscopy with noninvasive distraction has become a standard surgical tool for various ankle disorders. Even though a noninvasive distraction is safe and effective for ankle arthroscopy, combined use of tourniquet for additional open procedure requires special care since it can cause skin and soft tissue injury of the patient’s posterior thigh due to prolonged high pressure.
Footnotes
Authors’ note
All authors read and approved the final manuscript. All data analyzed during this study are included in this published article. The data sets during and/or analyzed during the current study available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT) (No.2018R1C1B5085206).
※ MSIT : Ministry of Science and ICT.