
Abstract
Objectives:
The aim of this study was to determine whether erythropoietin (EPO) can enhance rotator cuff healing in rats as measured by histological analysis and biomechanical testing.
Methods:
A total of 72 rats were included in this study. In the control group (n = 24), repair was performed without EPO injection. In the local group (n = 24) EPO was injected in the repair site. In the systemic group (n = 24) EPO was administered as an intraperitoneal injection every day for 10 days after repair. Rats were euthanized on day 10 (n = 12 from each group) and day 28 (n = 12 from each group). Histopathological (n = 6) and biomechanical examinations (n = 6) were done.
Results:
Biomechanical results reveal that the maximum load to failure values of the early control group were statistically lower than those of the early systemic group (p = 0.006). Comparing the the total Bonar values histopathologically reveal that the early systemic group was statistically higher than those of the early local group (p = 0.043). The late control group was statistically higher than those of the late local group (p = 0.003) and the late systemic group (p = 0.034). The late systemic group was statistically higher than those of the late local group (p = 0.003).
Conclusions:
EPO application had a positive effect biomechanically in the early euthanized group and histopathologically in the late euthanized group.
Introduction
Rotator cuff rupture (RCR) is a disease that has an increased incidence with age. 1 The supraspinatus muscle tendon complex is most commonly affected by both degenerative and traumatic rupture. 2 Rotator cuff surgery is a clinically successful procedure. 3 However, this clinical success is not always accompanied by the complete healing of the repaired structure. 4,5 The percentage of bone tendon healing failure in massive tears is still high. 6 Usually, after repair, the rotator tendon heals with mechanically weaker fibrovascular tissue. 7,8 This result may explain higher incidence of recurrent tears after repair. 4 Erythropoietin (EPO) is a glycoprotein hormone that has a weight of 34 kDa and binds to the high-affinity receptor produced by erythroid progenitor cells, thereby regulating erythrocyte development. 9 Due to its hematopoietic effects, it is widely used in chronic renal insufficiency and chemotherapy-related anemia. 10
The EPO receptor has been found to be released in cells other than those of the hemopoietic system, indicating that EPO has other functions. Other proven effects in addition to the hematopoietic effect of EPO include antioxidant, 11 antiapoptotic, 12 angiogenic, 13 and neuroprotective properties. 14 EPO has also been shown to have a positive effect on wound healing, 15 cartilage cell proliferation, and fracture healing. 16 In the literature, there are few studies on the role of EPO in tendon healing. One study showed a positive effect of EPO on patellar tendon healing, 17 and another study showed the ineffectiveness of EPO on Achilles tendon healing. 18 Angiogenesis is necessary for repairing damaged tissue, and it is mainly provided by hypoxic stimulation and proangiogenic factors such as EPO. 13,18 The purpose of this study was to investigate the role of systemic and local EPO administration on the healing of an experimental RCR assessed both biomechanically and histopathologically. We hypothesized that the administration of EPO would have a positive effect on rotator cuff healing.
Materials and methods
Animals
The study was carried out in Acibadem University Experimental Animal Research Laboratory with the reference No. 2016/37 of Acibadem University Experimental Animal Center Local Ethics Committee. Seventy-two Wistar albino genus, female rats, aged 5–7 months with a weight of 300–350 g were included in the study. Each of the rats included in the study was housed separately in a cage with a controlled temperature and 12-h light/12-h dark cycle after operation. After wound healing, —three to four rats were housed in a cage. Rats were fed ad libitum without adhering to any nutrient restriction during the experiment.
Groups and treatment modalities
Before the procedure, power analysis using maximum load data from the most similar rat rotator cuff studies available from the literature was performed. This resulted in a sample size of 6, for a power of 80%, with a p value of 0.05 determining significance. In our study, we surgically planned to repair RCR surgically by creating a full-thickness supraspinatus tendon tear. The rats were divided into three large groups (n = 72). In the control group (n = 24), surgical repair was performed. In the local group after surgical repair (n = 24), EPO (Binocrit, Sandoz Pharmaceuticals, Istanbul, Turkey) was applied locally at a dose of 500 U/kg (150–175 U), where the tendon was sutured to the bone. In the systemic group (n = 24), systemic EPO was administered as an intraperitoneal injection at a dose of 500 U/kg/day (150–175 U) every day for 10 days, starting on the first day after surgical repair. According to time of euthanization, each group was divided into two groups. Half of the rats (n = 12) were euthanized on the 10th day (early group) to show an early effect, and the other half were euthanized on the 28th day (late group) to show the late effects of EPO. Thus, six subgroups were formed: early control, early local, early systemic, late control, late local, and late systemic groups. In each subgroup, half of the euthanized animals (n = 6) were examined histopathologically, and the other half were examined biomechanically (n = 6) (Figure 1).

Separation of groups.
Preparation of animals
The rats were anesthetized with 90 mg/kg ketamine hydrochloride (Ketalar®; Pfizer, NYC, New york, USA) and 70 mg/kg xylazine (Rompun®; Bayer, Germany). Then, the right shoulder region of each rat was shaved, and antisepsis was provided with a solution of 10% povidone-iodine (Batticon, Adeka Pharmaceuticals, Turkey). Subsequently, 10 mg/kg cefazolin Na (Sefazol®; Mustafa Nevzat Pharmaceuticals, Turkey) was administered intramuscularly as a preoperative antibiotic prophylaxis.
Surgical technique
The deltoid split technique was the preferred surgical technique. A craniolateral incision was made to reach the acromioclavicular joint. The acromioclavicular joint was sharply dissected, and from the origin of the deltoid on the acromion, the deltoid was split. The supraspinatus tendon was identified. A modified Mason–Allen technique was applied to the tendon with a 4.0 polypropylene suture, and the tendon was separated totally from the major tuberculum of the humerus. A hole was made 2 mm distal to the supraspinatus footprint and 2 mm lateral to the humerus joint surface with a 21-gauge needle. The suture was passed through the humerus via the hole and was tied (Figure 2). 19
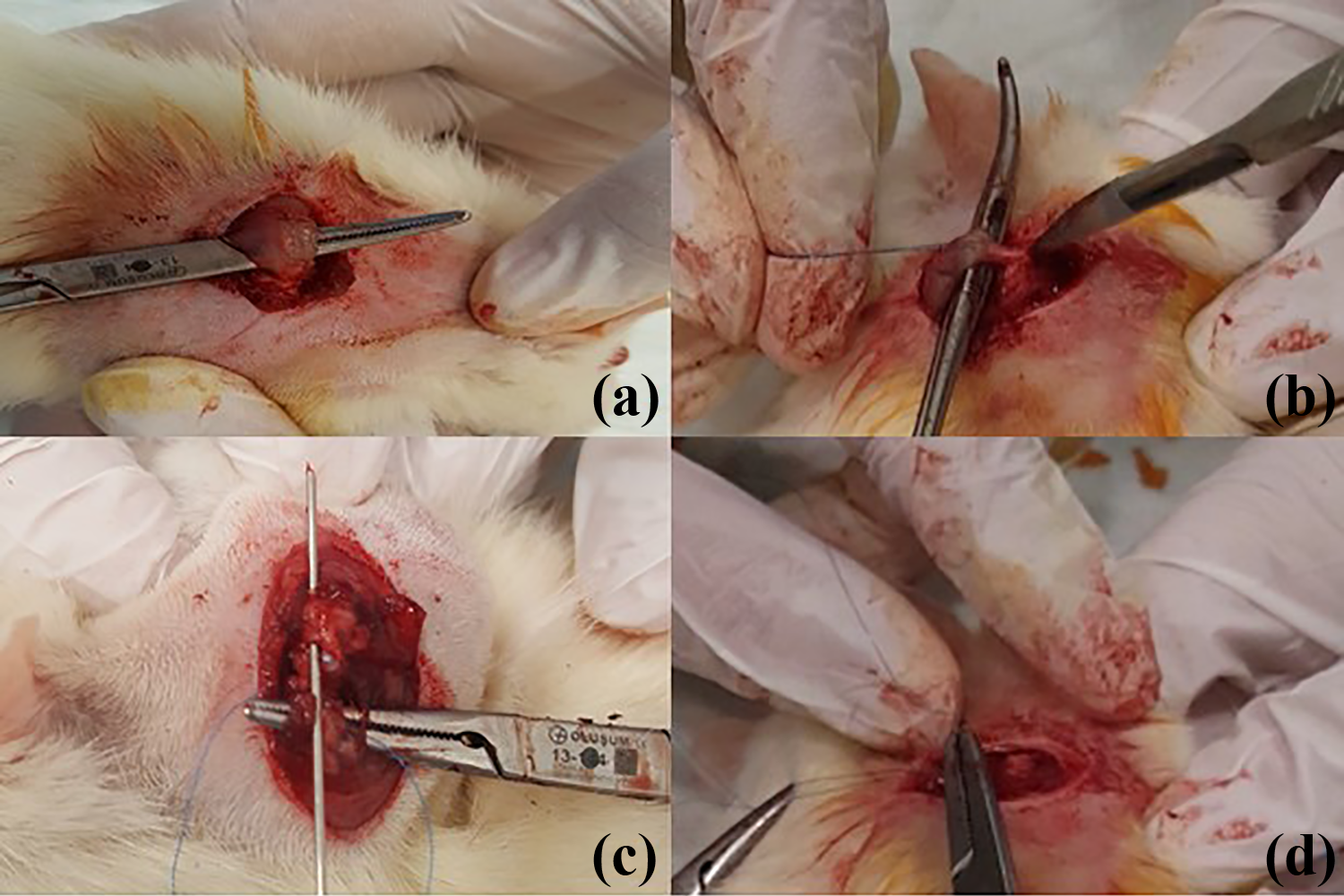
(a) Identification of supraspinatus tendon. (b) Sharp separation of the supraspinatus tendon from the humerus. (c) Making a hole in the humerus. (d) Passing the sutures through the hole.
Evaluation
Half of the animals from each group were euthanized at the end of the 10th day and the other half were euthanized at the end of the 28th day with high-dose isoflurane. The upper right limbs of the rats were removed en bloc, including the scapula.
Biomechanical evaluation
The specimens to be subjected to biomechanical testing were kept at −20°C until the test day. On the day of the test, the samples were thawed at room temperature. The test was performed with the “MTS Acumen Electrodynamics Test System” at the Biomechanics Laboratory of Response Ortho Technology Production, Inc. Samples were prepared for biomechanical testing, and the humerus was cut with a scissor. All muscle connections, including subscapularis and infraspinatus, were carefully detached, except for the supraspinatus from the scapula and humerus. A handmade system was designed using sand paper to stabilize the sample (Figure 3). In the biomechanical test, the system was set to a loading speed of 0.1 mm/s with 0.2-N preload. The maximum load and stiffness parameters were noted for each sample as described by Galatz et al. 19

(a) Dissection of all muscles except supraspinatus. (b) A handmade system using sand paper.
Histopathological evaluation
Each sample allocated for histopathological evaluation was sent to the Department of Pathology, Faculty of Medicine, Bahçeşehir University. Samples were placed in a 10% neutral formaldehyde solution for 48 h and then decalcified for 10 days. The samples were longitudinally cut and embedded in paraffin. After these routine procedures, three 5-mm-thick sections were prepared. Hematoxylin–eosin stain was used to evaluate the histopathological changes, Alcian blue stain was used to identify the mucinous material at the base, and trichrome stain was used to identify the amount of collagen. The examination was evaluated by a blinded pathologist with light microscopy. The tenocytes, ground substance, amount of collagen, and vascularity parameters were assessed using Bonar semi-quantitative scoring system developed by Maffulli et al. 20 (Table 1). In this scoring system, an increase in value indicates that healing is worse, whereas a decrease in value indicates that healing is better.
Bonar histological semiquantitative scoring system.

Statistical methods
The data were analyzed statistically using IBM SPSS Statistics 22 (IBM SPSS, Turkey). The normal distribution of the parameters was evaluated by the Shapiro–Wilk test. The Kruskal–Wallis test was used to compare the groups with an abnormal distribution in the comparison of the quantitative data, and the Mann–Whitney U test was used for the determination of the group causing the difference. Significance was assessed at the p < 0.05 level.
Results
A rat in the early control group and a rat in the early local group failed to awake from anesthesia. A rat from the early local group was found dead on the second postoperative day, and a rat from the late control group died on the third postoperative day. Hence, in the early local group, a rat was not subjected to histopathological examination and a rat was not subjected to biomechanical examination. A rat from each of the early control group and the late control group was not biomechanically examined. The results of the early and late groups were evaluated within themselves.
Biomechanical results
The maximum load to failure values of the early control group were statistically significantly lower than those of the early systemic group (p = 0.006; p < 0.05). There was no statistically significant difference in the maximum load to failure values between the other groups (p > 0.05). There was no statistically significant difference in the rigidity values between the groups (p > 0.05; Table 2, Figure 4).
Biomechanical results of the groups.
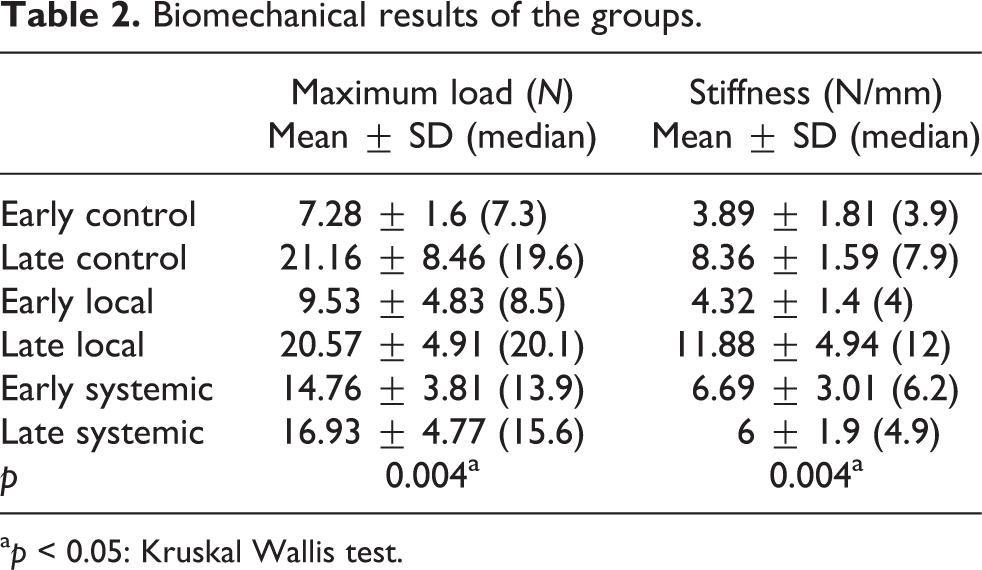
a p < 0.05: Kruskal Wallis test.
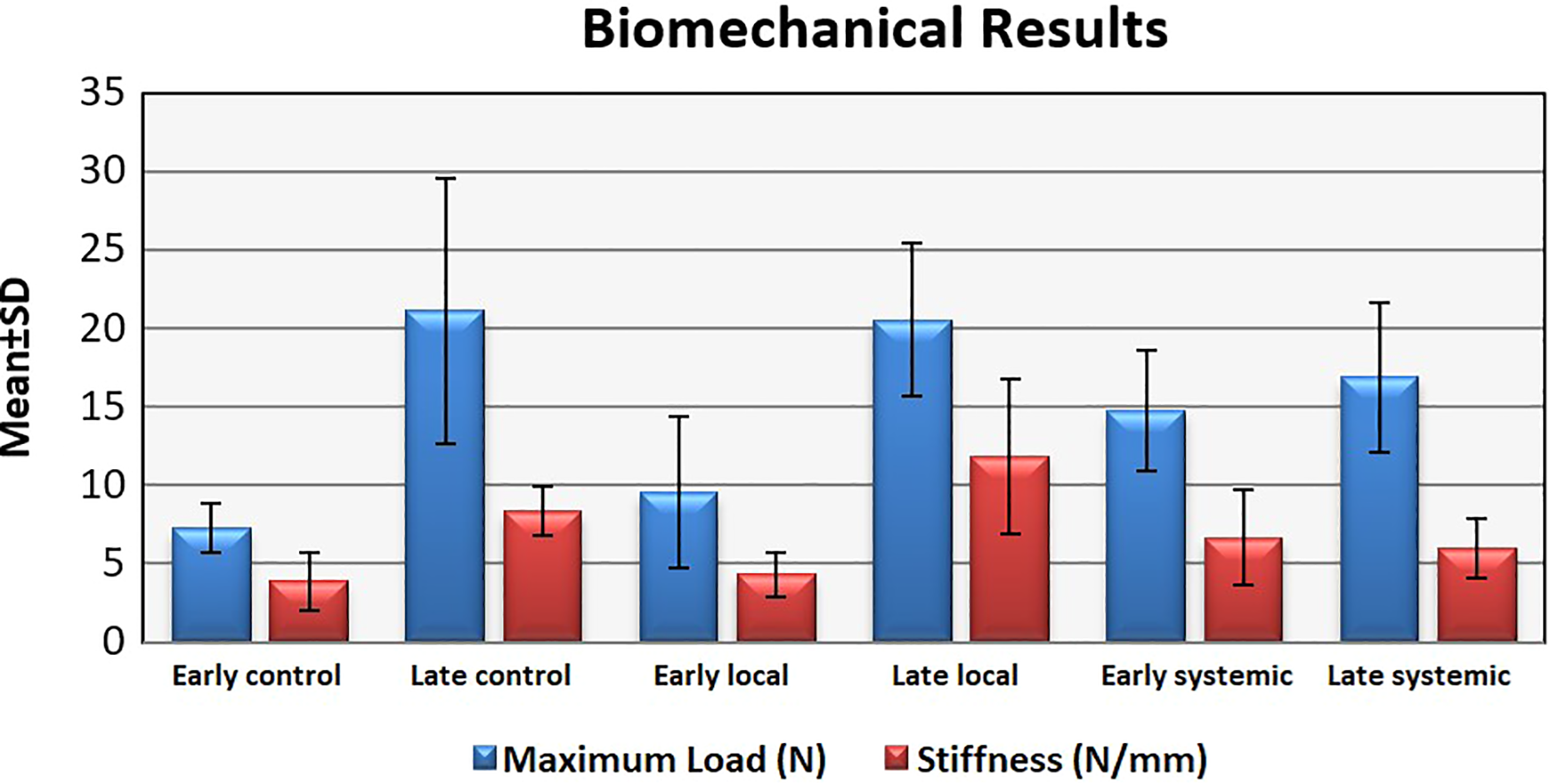
Biomechanical results of all groups.
Histopathological results
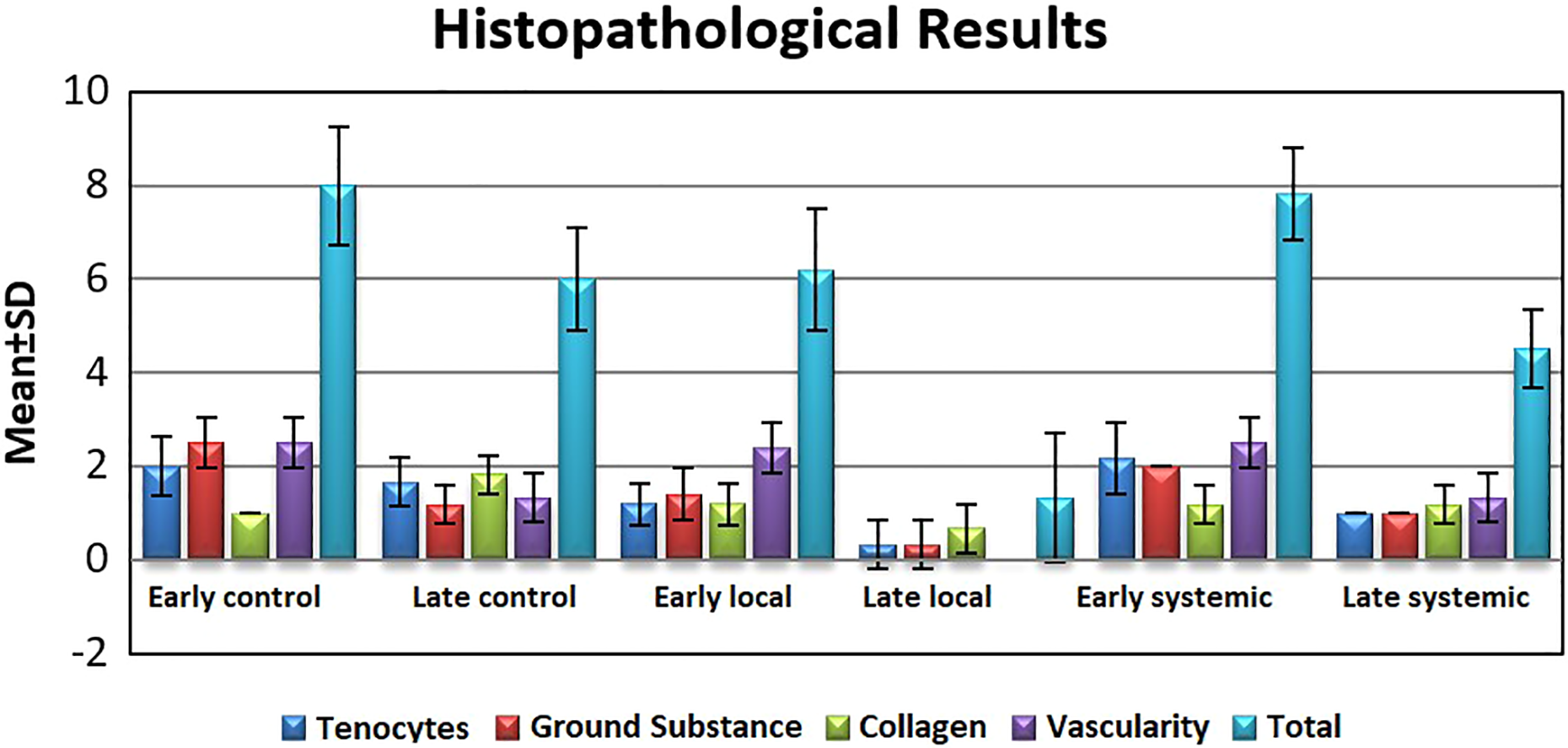
The tenocyte values comparison shows that early systemic (p = 0.039) and early control (p = 0.044) groups were statistically higher than those of the early local group (p < 0.05). Late control group was statistically higher than those of the late local (p = 0.007) and late systemic (p = 0.019) groups (p < 0.05). Late systemic group was statistically higher than those of the late local group (p = 0.019) (p < 0.05). There was no statistically significant difference between the other groups (p > 0.05). The ground substance values comparison shows that the early control (p = 0.019) and early systemic (p = 0.034) groups were statistically higher than those of the early local group (p < 0.05). Late control (p = 0.018) and late systemic (p = 0.019) groups were statistically higher than those of the late local group (p < 0.05). There was no statistically significant difference between the other groups (p > 0.05). The collagen values comparison reveal that the early systemic group was statistically higher than those of the early local group (p = 0.039) (p < 0.05). Late control group was statistically higher than those of the late local (p = 0.006) and late systemic (p = 0.027) groups (p < 0.05). There was no statistically significant difference between the other groups (p > 0.05). The vascularity values comparison reveal that the late control (p = 0.02) and late systemic (p = 0.02) groups were statistically higher than those of the late local group (p < 0.05). There was no statistically significant difference between the other groups (p > 0.05) (Figures 5 and 6).

(a) Nucleolar clearance, nucleolar largeness, and rounding in tenocytes in the early control group (hematoxylin and eosin ×400). (b) Irregularity of collagen fibers in the early control group, complete detachment of the collagen bundle (trichrome ×400). (c) Moderate irregularities in the collagen fibers, partial deterioration of the collagen bundle formation, and increased vascularity in the early systemic group (trichrome ×40). (d) Minimal irregularity in collagen fibers in the early local group (trichrome ×40).

(a) Increased vascularity in the late control group (hematoxylin and eosin ×400). (b) Increased mucin in the late control group (PAS AB2.5 ×100). (c) Decrease in moderate irregularities in collagen fibers in the late systemic group (hematoxylin and eosin ×40). (d) Enlarged view of (c), areas where collagen fibers showed more irregularity (hematoxylin and eosin ×400). (e) Near-normal appearance in the late local group (hematoxylin and eosin ×40). (f) Enlarged view of (e), normal appearance of tissue organization (hematoxylin and eosin ×100).
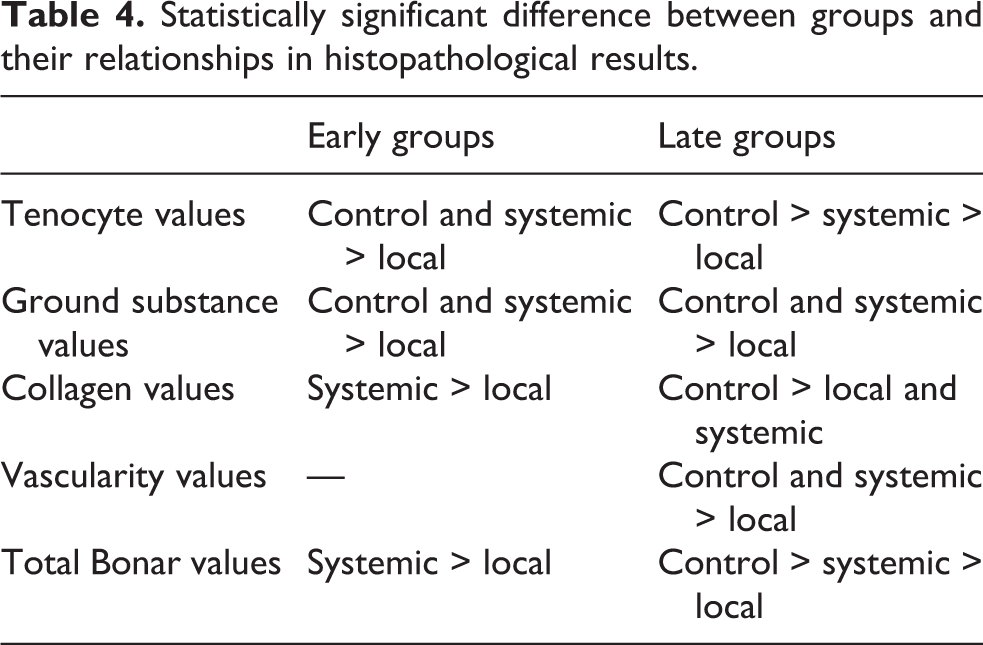
The total Bonar values comparison show that the early systemic group was statistically higher than those of the early local group (p = 0.043) (p < 0.05). The late control group was statistically higher than those of the late local (p = 0.003) and late systemic (p = 0.034) groups (p < 0.05). The late systemic group was statistically higher than those of the late local group (p = 0.003) (p < 0.05). There was no statistically significant difference between the other groups (p > 0.05; Tables 3 and 4, Figure 7).
Histopathological results of all groups.

a p < 0.05: Kruskal Wallis test.
Statistically significant difference between groups and their relationships in histopathological results.
Histopathological results of all groups.
Discussion
Although the results of rotator cuff repair have improved in recent years, the percentage of bone tendon healing is still at an unexpected level. 6 In this study, our aim was to demonstrate the contribution of EPO application to rotator cuff healing in rats, both biomechanically and histopathologically. In our study, it was observed that EPO application contributed to rotator cuff healing biomechanically only in the early systemic group while histologically in both the late systemic and the late local groups; in the late local group, histopathological healing was better than the late systemic group. Many studies have demonstrated the utility of EPO in musculoskeletal pathologies, most of which focused on cartilage and bone healing. 21,22 Uslu et al. compared systemic EPO (500 U/kg/day) administration with a control group in a patellar tendon repair model in rats. They showed that the maximum load values at 3 and 6 weeks were higher in the treated group than the control group. 17 In our study, although the maximum load values in the early phase (10th day) were superior to the control group, there was no statistically significant difference in the late phase (28th week) compared with the control group. This result shows that EPO had only accelerating effect in providing biomechanical strength, but it had no effect on increasing biomechanical capacity.
Histopathologically, Uslu et al. found worse results in the EPO group in the 3rd week but did not find any significant difference in the 6th week. 17 In our study, EPO application showed better results in the late period (4th week) histopathologically although in the early period (10th day), local group showed better results than the systemic group but neither of them had superiority to the control group. Such histopathological differences could be related to the lack of consensus in the scoring system evaluating tendon healing. In an Achilles tendon repair model, Bilal et al. found no effect on tendon healing with systemic EPO (500 U/kg) administration either histopathologically or biomechanically. 18 In our study, we found better results biomechanically in the early systemic group (10th day), and histopathologically, we found better results in the late systemic and the late local groups compared to the late control group (28th day). This result could be related to the differences between the rotator cuff and Achilles tendon structures.
In a rat model, Ross et al. found that granulocyte colony-stimulating factor (GSF) had a negative effect on rotator cuff healing biomechanically. 23 In a similar study, Beck et al. investigated the effectiveness of platelet-rich plasma (PRP) on a rotator cuff repair model and found no superiority to the control group biomechanically. 24 Kovacevic et al. examined the effects of the platelet-derived growth factor (PDGF) and found no difference between the groups. 25 Unlike the previous studies, Cheng et al. found that tumor necrosis factor alpha-stimulated gene/protein 6 (TSG-6) and tendon-derived stem cells contributed to the biomechanical recovery of the rotator cuff, which was parallel to our work. 26
In our study, there was no significant difference between rigidity values when the early groups and late groups were evaluated among themselves. This result is in line with Beck at al.’s PRP study, 24 although Ross et al.’s study with GSF control group had increased rigidity in the control group compared to the other groups. 23 In a study by Bilal et al. on the effects of EPO on the Achilles tendon investigated at 3 weeks, the EPO-treated group showed worse results than did the control group when vascular formation was examined. 18 This result is inconsistent with our findings. The reason for this conflict may be related to their design, because they observed that the control group also showed a decrease in vascular formation over time, but it was not statistically significant.
In our study, the early systemic group had a higher collagen Bonar score than did the early local group, although there was no significant difference between the control group and the other early groups. In the late groups, the control group had a statistically worse Bonar score than did the other two groups. In a rotator cuff repair model, PDGF did not appear to contribute to the maturation or orientation of the collagen fibers. 25 This result shows that EPO had a positive effect on collagen maturation, unlike PDGF. When vascularity values were considered, there was no statistically significant difference between the early groups. In the late group, the local group showed a significantly lower Bonar score than did the control and systemic groups. As a result, it has been suggested that local EPO administration contributes to vascularization in the late period. In a study evaluating patellar tendon healing with EPO, it has been shown that EPO contributes to capillary vessel formation. 17
Considering the total Bonar score, neither systemic nor local EPO administration was beneficial in the early period, but they seemed to be beneficial in the late period compared to the control groups. The histopathological results of our study are in parallel with the literature. 23,24 Local EPO application was found to be superior in both the early and the late periods compared to systemic application. This may suggest that the local administration of EPO was more effective by reaching higher doses in the tendon healing area than systemic application, but the biomechanical results are inconsistent with this situation. There are no studies comparing the local and systemic effects of EPO on tendon healing in the literature. Therefore, further studies are required for better understanding.
High-dose systemic EPO administration could increase the risk of thromboembolism. 27,28 Patients with comorbidities could have increased complication rates with high-dose systemic EPO usage. Because of these disadvantages, the current studies are more focused on systemically lower dose or local EPO administration. Thus, we preferred lower doses of systemic EPO in our study than the doses used in previous studies. 22,29
There were some limitations in our study. First, it was an animal study, with all the inherent limitations of experimental studies which have some degree of clinical relevance but lacks the clinical value and relative precision of the studies performed in a clinical setting. Second, in our study, an acute damage repair model was used, which differs from the usual pattern of rotator cuff tears in humans that are secondary to chronic degenerative changes in humans. This could have been addressed by creating a chronic rotator cuff tear model in such a study. Third, the preference of lower dose EPO than previous studies may also have reduced the systemic effect. 22,29 Finally, the difficulty of maintaining EPO in the repair site following local application can be considered as another limitation.
To the best of our knowledge, this is the first study to use EPO administration to enhance rotator cuff healing. In our study, EPO application was found to be successful in some groups but showed no effect in the other groups. This may be considered a promising result for the application of EPO to rotator cuff repair in the future. However, we believe that studies with more subjects that are prospective in nature, in addition to randomized controlled human studies, are essential to support this result.
Conclusions
The results of the current study showed that EPO application had a positive effect biomechanically in the early systemic group and histopathologically in the late euthanized groups. Further, histopathologically, EPO application showed better result in the late local group than the late systemic group. EPO may be an effective way to enhance rotator cuff repair.
Footnotes
Acknowledgements
We thank veterinarian Samed Ozer from Acibadem University Experimental Animal Research Laboratory for providing support with animal care. We also thank Biomechanics Laboratory of Response Ortho Technology Production, Inc. employees for helping with the use of “MTS Acumen Electrodynamic Test System.”
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was carried out in Acibadem University Experimental Animal Research Laboratory with the reference No. 2016/37 of Acibadem University Experimental Animal Center Local Ethics Committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.