
Abstract
Background:
The purpose of this study was to assess the influence of developmental dysplasia of the hip (DDH) on patella alignment.
Methods:
The radiographic data of all the patients who met the inclusion criteria from January 2015 to July 2017 were reviewed, including the quadriceps angle (QA), patellar lateral tilt (PTA), sulcus angle (SA), lateral shift of patella (LSP), and lower limbs alignment. The patients were divided into three groups in accordance with lateral center-edge angle (LCE) and femoral neck torsion angle (FNTA): group A (LCE > 25° and FNTA < 40°), group B (LCE < 20° and FNTA < 40°), and group C (LCE < 20° and FNTA > 40°).
Results:
One hundred thirty-eight patients with 230 hips (115 females and 23 males) were recruited with an average age of 22 years. There were significant differences between group A and group C as well as group B and group C in QA, SA, PTA, LSP, and lower limbs alignment (p < 0.01). There were no differences in SA, PTA, LSP, and lower limbs alignment (p >0.05) and significant differences in QA (p < 0.01) between group B and group C. The “Pearson’s” correlation analysis of the data in total of group B and group C showed that FNTA and LCE and QA and LCE were negatively correlated, whereas FNTA and QA, PTA, SA, and lower limbs alignment as well as SA, PTA, and lower limbs alignment were positively correlated.
Conclusion:
Patients with DDH not only have hip joint change, but also have the patella alignment abnormality, which may lead to patella instability. In the clinic, we should pay attention to the hip development of the patella instability patients for excluding DDH.
Introduction
Developmental dysplasia of the hip (DDH) or congenital dislocation of the hip (CDH) 1 is the most common condition resulting into secondary osteoarthritis of the hip. DDH mainly shows the morphology abnormity of the acetabulum or the proximal femur. The bone defect of the acetabulum may lead to shallow acetabulum and the outward shift of the hip center. 2 Many studies indicate that the satisfied effects are gained by early discovery and treatment. 3,4 In clinic, we found that part of the patients with DDH complained the knee pain, even as the first symptom. As a result, it was supposed that DDH may affect the knee. Indeed, Hasegawa and Iwata showed that DDH promoted the development and degeneration of the patellofemoral and tibio femoral joints leading to knee pain. 5 And the reports 6 –8 were concluded that DDH may give rise to the knee symptom due to femoral condyle diameter and patellofemoral angle change and the limb alignment. However, we found that DDH not only lead to the limb alignment and the knee morphology change, but also cause obvious patellar tilt and lateral shift with patellar instability in the daily work.
Patellar instability, especially in young woman, is the common cause of patellofemoral osteoarthritis or chondromalacia patellae leading to the knee pain. 9 Dejoure et al. 9 adopted the bilateral knee joint imaging data comparison to present that the patellar instability was due to multiple factors, such as femoral trochlear dysplasia, quadriceps dysplasia, patella alta, and tibial tuberosity–trochlear groove abnormity. Alexis and Robin considered that patellar instability was caused by the limb alignment, bone structure, and soft tissue, and it should adopted the operation to balance the multiple factors. 10
Many studies 7,8 mainly explored the limb alignment and the knee morphology change in DDH patients. However, very few manuscripts discussed the patella alignment in DDH patients by far. Herein, the purpose of this study was to assess the influence of DDH on the patella alignment.
Methods
The study was approved by the institutional review board and the medical ethics committee (number 2014KY003) of the first author’s institution. The patients with hip disorder who met the inclusion criteria were retrospectively reviewed in the period between January 2015 and July 2017. The affected knees were defined as the ipsilateral knees to the DDH, and the unaffected patellae were defined as the patellae on the contralateral side in patients with unilateral DDH. To be included in the study, the patients (10–45 years) were diagnosed with a past medical history of Hartofilakidis et al.’s 11 type DDH that has never been treated and had whole radiography data including pelvic plain film, weight-bearing full-length film of the lower limbs, and pelvic and knee computed tomographies (CTs). We also chose one side hip joint of the patients with normal lateral center-edge angle (LCE) and femoral neck torsion angle (FNTA), for contrast. Patients were excluded if they had other musculoskeletal abnormalities, neuromuscular disease, or hip osteoarthritis of Tönnis’s grade 3, 12 or if they had prior surgical treatment for hip or knee problems. One hundred thirty-eight 138 patients (115 females and 23 males) with a mean age of 22.4 years ranging from 12 years to 39 years were recruited during the study period. The study included 120 left hips and 110 right hips. All the patients took full-length films of lower limbs by standard standing position. The standard standing position is the tibial tubercle and tiptoe facing forward. 13,14
Radiographic data
After informed consent was obtained from all the participants, a full medical history and data collection examination were performed by the first author and the second author. All individuals were evaluated with direct radiography and computerized tomography. Direct radiography was used for analysis in the coronal plane and computerized tomography was used for analysis in the transverse plane, according to a standard protocol. Definitions and a list of all the measurements performed are shown in the below.
DDH includes acetabulum and thighbone abnormities. LCE 15 was calculated by measuring the angle between the vertical reference and the lateral edge of the sourcil, with the apex located at the center of a circle superimposed over the femoral head (Figure 1). FNTA 16,17 was the angle between the frontal plane and femoral neck axis projected onto the transversal plane of line between the medial and lateral femoral condyle midpoint based on CT scans (Figure 2). Jessel et al. showed that the normal value of LCE was more than 25° (critical value 20–25°). 18 If the LCE < 20 was defined as DDH. Sugano et al. 19 considered that FNTA > 40° was abnormal FNTA. In our study, the patients were divided into three groups on the basis of LCE<20° and FNTA > 40°: group A (LCE > 25° and FNTA < 40°), group B (LCE < 20° and FNTA < 40°), and group C (LCE < 20° and FNTA > 40°). Patients were excluded due to merely FNTA increase and reduction and LCE > 40°.

Representative anteroposterior image of the pelvis illustrating the measurement of LCE between (a) the lateral edge of the sourcil, (b) the apex located at the center of a circle superimposed over the femoral head, and (c) the vertical reference. LCE: lateral center-edge angle.

FNTA based on CT scans was the angle between (d) the frontal plane and femoral neck axis and (e) and (f) projected onto the transversal plane of line between the medial and lateral femoral condyle midpoint. FNTA: femoral neck torsion angle; CT: computed tomography.
The radiographic data include the quadriceps angle (QA), lower limbs alignment, patellar lateral tilt (PTA), sulcus angle (SA), and lateral shift of patella (LSP). QA was measured as the angle between a line drawn from the cranial lip of the acetabulum to the center of the patella (Figure 3(a)) and a line from the center of the patella to the center of the tibial tuberosity (Figure 3(b)). 20 Lower limbs alignment was calculated on the coronal plane of weight-bearing full-length film as the angle between the femoral mechanical axis between the femur head and apex of the femoral condyle (Figure 3(c)) and the tibial mechanical axis between the tibial intercondylar eminence midpoint and the ankle center (Figure 3(d)). 21 We defined that the value of the lower limbs alignment was negative if varus, while positive if valgus. PTA 22 was measured between the coronal axis of the patella and a line tangent to the medial and lateral trochlear ridges (Figure 4(a)). SA was measured in the axial plane. 23 The angle was calculated using the most anterior points on the medial and lateral facets and the deepest point in the trochlear groove (Figure 4(b)). SA > 145° was considered the trochlear groove maldevelopment. 9 LSP was measured as the distance (I) between the perpendicular line of the apex of the medial femoral condyle to the line of the apex of the medial femoral condyle and the apex of the lateral femoral condyle to the medial edge of the patella. 24 The value of LSP to the transverse diameter of the patella is smaller than 0.5. The normal value of the LSP was less than 5 mm. LSP more than 5 mm was defined as patella lateral shift (Figure 5).
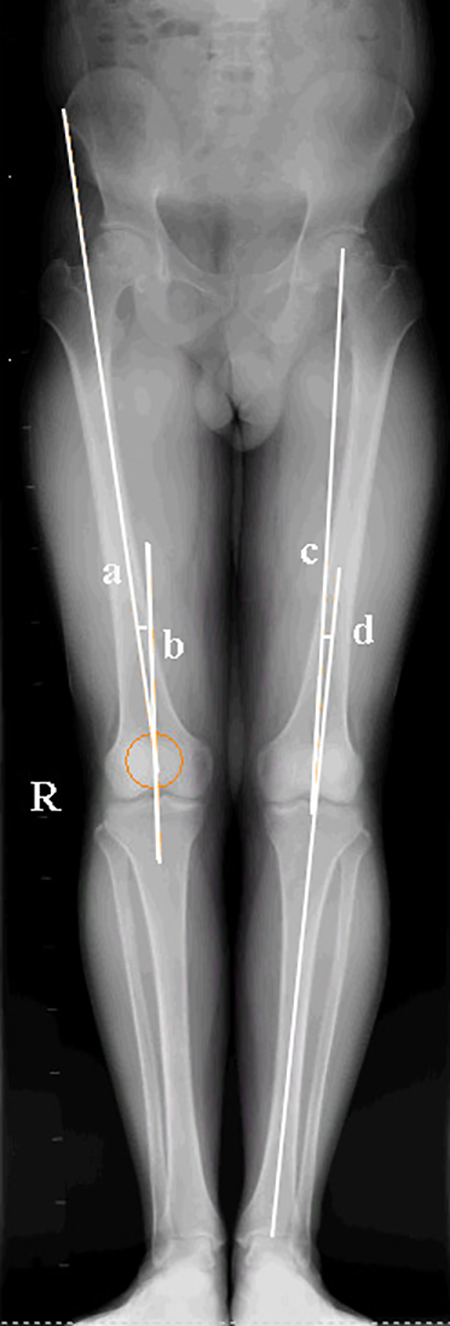
QA was measured on the coronal plane of weight-bearing full-length film as the angle between (a) a line drawn from the cranial lip of the acetabulum to the center of the patella and (b) a line from the center of the patella to the center of the tibial tuberosity. Lower limbs alignment was calculated on the coronal plane of weight-bearing full-length film as the angle between (c) the femoral mechanical axis between the femur head and apex of the femoral condyle and (d) tibial mechanical axis between the tibial intercondylar eminence midpoint and the ankle center. QA: quadriceps angle.

(e) PTA was measured in the axial plane (right) between the coronal axis of the patella and a line tangent to the medial and lateral trochlear ridges. (f) SA was calculated in the axial plane (left) using the most anterior points on the medial and lateral facets and the deepest point in the trochlear groove. PTA: patellar lateral tilt; SA: sulcus angle.

LSP was measured in the axial plane as the distance (I) between the perpendicular line of the apex of the medial femoral condyle to the line of the apex of the medial femoral condyle and the apex of the lateral femoral condyle to the medial edge of the patella. LSP more than 5 mm was defined as patella lateral shift. LSP: lateral shift of patella.
Statistical analysis
Statistical analysis was performed using SPSS 22.0 software (SPSS Inc., Chicago, Illinois, USA). To minimize measurement error, all measurements were made by two doctors (HBJ and SLL). HBJ and SLL measured 230 hip-patella samples first. After an interval of 1 month, HBJ and SLL measured 230 samples again, respectively. The intra- and interobserver reliabilities were determined by intraclass correlation coefficient (ICC). All the measurement data (
Results
One hundred thirty-eight patients with 230 hips (115 females and 23 males) were prospectively recruited with an average age of 22 years. The average LCE and FNTA of group A (34 hips), respectively, were 27.75° ± 2.73° and 21.58° ± 7.16°. The average LCE and FNTA of group B (116 hips), respectively, were 7.65° ± 10.42° and 29.58° ± 6.91°. The average LCE and FNTA of group C (80 hips), respectively, were −2.97° ± 11.50° and 48.48° ± 7.01°. There were no differences in age, gender, and the hip count among the three groups (Table 1).
Comparisons of general data among three groups (n = 230,
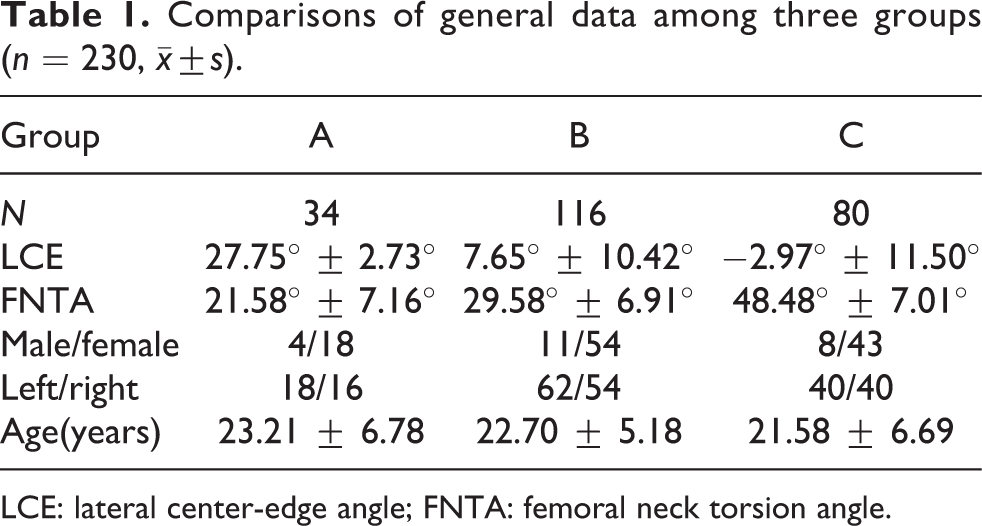
LCE: lateral center-edge angle; FNTA: femoral neck torsion angle.
There were significant differences between group A and group C as well as group B and group C in QA, SA, PTA, LSP, and lower limbs alignment (p < 0.01). There were no differences in SA, PTA, LSP, and lower limbs alignment (p > 0.05) and significant differences in QA (p < 0.01) between group B and group C (Table 2).
Comparisons of PTA, QA, SA, lower limbs alignment, and LSP among three groups(n = 230,

PTA: patellar lateral tilt; QA: quadriceps angle; SA: sulcus angle; LSP: lateral shift of patella.
a p < 0.05 was statistical difference.
b p < 0.01 was statistical significant difference.
cAB, BC, and AC were comparisons with each other among group A, group B, and group C.
The Pearson’s correlation analysis of the data in total of group B and group C showed that FNTA and LCE and QA and LCE were negatively correlated, whereas FNTA and QA, PTA, SA, and lower limbs alignment as well as SA,PTA, and lower limbs alignment were positively correlated (Table 3).
Correlation analyses of LCE, FNTA, QA, PTA, SA, and lower limbs alignment in group B and group C.

LCE: lateral center-edge angle; FNTA: femoral neck torsion angle; PTA: patellar lateral tilt; QA: quadriceps angle; SA: sulcus angle.
a p < 0.05 (two-tailed) was statistical difference.
b p < 0.01 (two-tailed) was statistical significant difference.
c r was Pearson’s correlationcoefficient.
The intra- and interobserver reliabilities were determined by ICC. The intra- and interobserver reliabilities were considered as good (Table 4).
The intra- and interobserver variations of measurements.
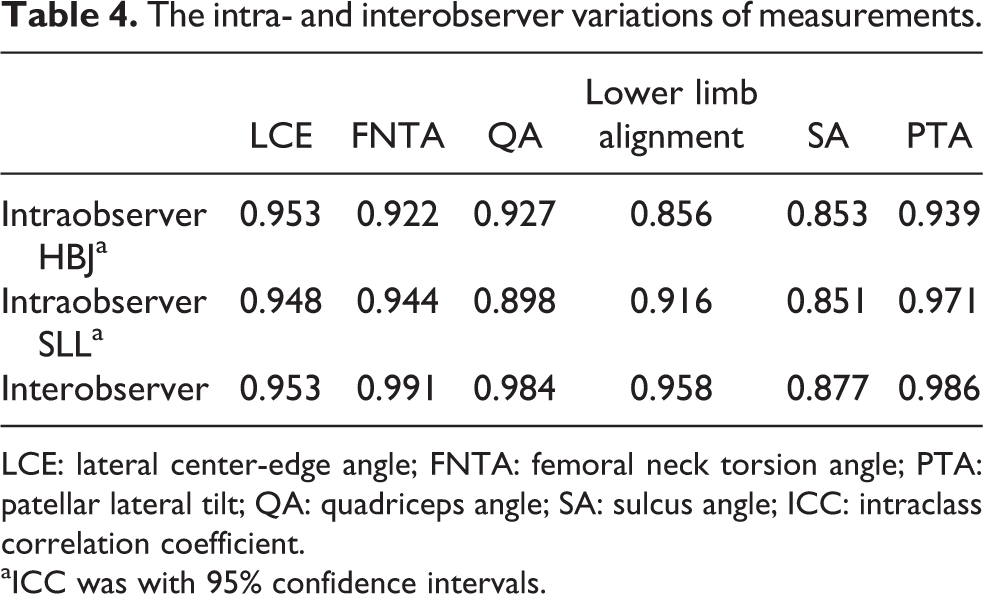
LCE: lateral center-edge angle; FNTA: femoral neck torsion angle; PTA: patellar lateral tilt; QA: quadriceps angle; SA: sulcus angle; ICC: intraclass correlation coefficient.
aICC was with 95% confidence intervals.
Discussion
Patients with DDH present with the size, shape, or morphology abnormalities of the femoral head and acetabular. 25 Acetabular dysplasia is characterized with the immature development and the shallow acetabulum leading to subluxation or dislocation of the femoral head and eventually developing into hip osteoarthritis, which may need the therapy of the total hip replacement. 26 About 1–2 out of every 1000 newborns have suffered from hip dislocation and about 15–20 newborns have hip instability. 3 The Hartofilakidis et al.’s system for classification of congenital hip disease (CDH) 11,27,28 in adult was below. I type was defined as femoral head contained within the original acetabulum, despite the degree of subluxation. II type was defined as femoral head articulate with a false acetabulum that partially covers the true acetabulum to a varying degree. II type was defined as femoral head completely out of the true acetabulum and migrated superiorly and posteriorly to a varying degree.
DDH in preliminary stage showed hip soreness and pain after long standing or walking or even the knee pain. Many studies were on DDH diagnosis and treatment, while less attention was to the natural development of DDH. 29 Hasegawa and Iwata 5 considered that the knee pain of DDH patients was due to the patellofemoral and femorotibial degeneration. Moreover, the studies showed that the cause was lower limbs alignment change. 6 –8 Patients with DDH often complained of knee pain as the mainly symptom in the first visit. Therefore, we may ignore hip disorder. In the clinic, we found that DDH may lead to obvious patellar tilt and lateral shift with the patellar instability. Many studies 7,8 mainly explored the limb alignment and the knee morphology change in DDH patients. However, very few manuscripts discussed the patella alignment in DDH patients by far.
Patellar instability is the common cause of patellofemoral osteoarthritis or chondromalacia patellae leading to the knee pain. 9 The construct balance around patella may be damaged, which may cause patella tilt, subluxation, and dislocation. 30 Fulkerson et al. 31 considered that the patellar instability is divided into three types, such as patellar subluxation, patellar tilt, and both of them. Patellar instability may be due to femoral condylar dysplasia with shallow intercondylar fossa (SA > 140°), knee valgus, increscent QA leading to high pressure of lateral patellofemoral joint, and patella dysplasia. 32 Dejour and Le Coultre showed that 96% of patients with patellar dislocation have trochlear dysplasia. 33
We retrospectively divided the patients into three groups, which were aimed to assess the influence of DDH on the patella alignment. The results suggest that patients with normal development of hips have normal patellar alignment and no patella instability. There were significant differences between group A and group C as well as group B and group C in QA, SA, PTA, LSP, and lower limbs alignment (p < 0.01; Table 2). The results suggested that compared with those in group A, increasing QA, SA, PTA, LSP, and valgus angle of the lower limbs in group B and group C leads to patellar instability. When comparing group B and group C, we found that FNTA and QA may increase along with the LCE reduction. And the differences were significant. Moreover, increasing QA, SA, PTA, LSP, and valgus angle of the lower limbs are all likely to cause patellar instability. The Pearson’s correlation analysis of the data in total of group B and group C showed that FNTA and LCE, and QA and LCE were negatively correlated, whereas FNTA and QA, PTA, SA, and lower limbs alignment as well as SA,PTA, and lower limbs alignment were positively correlated (Table 3). With the increase of FNTA, QA, and SA may cause large valgus angle of the lower limbs, which ultimately leads to patellar instability.
We have recognized limitations to this study. The use of retrospective method makes the evidence insufficient. The patients of group A were with normal LCE and FNTA in radiograph, in contrast, which were not represented in the normal population. In addition, we only provided the radiograph data and not recorded the clinical symptoms and its evolution process, which failed to determine whether the knee pain of the patients is due to hip dysplasia. The data analysis from one institution center may be biased. Herein, we should adopt prospective study of multiple institutions to analyze the influence of DDH on patella alignment and recruit appropriate sample of normal development of the hip, in contrast.
Conclusion
In conclusion, patients with DDH not only have hip joint change but also have the patella alignment abnormality, which may lead to the patella instability. FNTA and QA, PTA, SA, and lower limbs alignment as well as SA,PTA, and lower limbs alignment were positively correlated. With the increase of FNTA, QA and SA may cause large valgus angle of the lower limbs, which ultimately leads to the patellar instability. In the clinic, for the patella instability patients, we should pay attention to the hip development excluding DDH.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.