
Abstract
Purpose:
The aim of our work is to evaluate results obtained from a cohort of patients affected by periprosthetic joint infection and treated with a primary cementless stem in a two-stage technique framework.
Methods:
Eighty-four patients were evaluated at a mean follow-up of 37.4 months. The main demographic, surgical, clinical, and radiographic data were recorded. A femoral window for stem removal was performed in 33 patients.
Results:
Statistically significant improvement was noted for both the Harris Hip score and the Oxford Hip score. Postsurgical complications included thigh pain in three patients, subsidence (>2 mm) in one patient, implant dislocation in two patients, cup revision in one patient, implant revision for septic failure in two patients, and stem revision for varus position in one patient. The stem survivorship rate was 96.3%. There were no significant differences between the groups in which a cortical window was created or not.
Conclusion:
Femoral stem revision with primary cementless stems is a viable option in selected patients undergoing two-stage hip revision surgery. Correct indication is a cornerstone of good outcome. The use of a cortical window does not affect the final outcome or implant survivorship rate.
Keywords
Introduction
Data from orthopedic registries show that the number of total hip replacements is increasing, 1 –3 particularly among middle-aged patients (<55 years) 4 and older healthy patients with elevated functional demands. Hip implant revisions have risen in parallel, posing considerable challenges to orthopedic surgeons. 5 Infection accounts for about 17.5% of reasons for revision surgery. 1 Periprosthetic joint infection (PJI) has become increasingly common and a frequent cause of multiple revisions, resulting in diminished quality of life for patients and higher costs for society. 3 Surgical solutions for chronic PJI are one- or two-stage revision with the use of interim antibiotic-loaded cements spacers or beads. Both approaches provided good results even in complex cases. 6 –10
Surgeons performing revision hip arthroplasty will pay scrupulous attention to both the acetabular and the femoral aspects, particularly the latter, to achieve adequate primary stability with a stem implant that provides fixation as proximal as possible and as distal as necessary. 11 In this way, the proximal portion of the femur can be loaded to help preserve diaphyseal bone stock in the event of future revision reconstructions. With careful preoperative surgical planning and optimal patient selection, femoral revision with primary stems may offer a valid alternative.
The use of primary stems for revision surgery is not new. Early attempts were burdened by aseptic implant loosening in 44% of patients at 4.5 years. 12 The shift to cemented stems was equally unsuccessful, and failure rates were unacceptably high. Encouraged by the good outcomes with primary cementless stems, several authors obtained optimal mid-to-long-term results with cementless stems with distal anchorage. 13 –17 Although good results with primary cementless stems have recently been reported, most of the case series are highly heterogeneous and often include patients with aseptic implant loosening.
The aim of the present study was to evaluate the clinical and radiographic mid-term outcomes after two-stage hip revision for PJI in which the femoral component was exchanged with a primary cementless stem. Specifically, we wanted to (1) evaluate the feasibility of two-stage hip revision with primary cementless stems; (2) identify a patient subgroup with PJI that could benefit from primary stem implantation; and (3) determine whether cortical fenestration has an effect on the outcome in these patients.
Methods
The study protocol was approved by the local institutional review board. Informed consent was obtained from patients prior to surgery. The data were collected from the prospective institutional arthroplasty registry. We reviewed the clinical and radiographic data of 86 patients (86 hips) who underwent two-stage femoral revision with a primary cementless stem for PJI between March 2010 and June 2017. In the same time period, we treated 136 hip PJI. Of these 86 patients, 84 were assessed at the final follow-up and 2 had died of causes unrelated to surgery during the follow-up period. Two types of stems were used the CLS Spotorno stem (Zimmer-Biomet, Warsaw, Indianna, USA) and the Wagner Conus stem (Zimmer-Biomet). The CLS Spotorno stem has a 3-D wedge shape and a trapezoidal cross section; it comes in two versions, one with a caput–collum–diaphyseal (CCD) angle of 125° and the other with a CCD angle of 135° for different anatomical configurations. 18 The Wagner Conus also comes in two versions (CCD 125° and 135°) with eight longitudinal ribs for rotational stability. 19 Both implants are made from a special titanium alloy (Protasul-64), which, by virtue of its grit-blasted surface, promotes osseointegration of the entire stem.
Inclusion criteria were definitive diagnosis of PJI according to Musculoskeletal Infection Society criteria, 20 having completed two-stage revision with a primary cementless stem, minimum of 6 months since surgery. Exclusion criteria were one-stage revision, implant loosening, and not having completed two-stage revision. PJI were classified according to Tsukayama. 21 Patients were examined before surgery, during the period between stages to evaluate the development of sepsis, at 3, 6, and 12 months after revision surgery, and then yearly thereafter. Demographic data (age, sex, body mass index, and serious comorbidities) were recorded. Microbiological isolates obtained before and during surgery were identified. Surgical data included type of stem removed, number of previous surgeries, type of bone defect according to the Paprosky classification, 22 use or not of acetabular spacer, 23 type of femoral spacer (long stemmed or short stemmed), creation or not of a cortical window for stem removal, length and degree of integration, operating time for stem removal and implantation, mean time between the first and the second stage, type of stem, and collar used for revision. Clinical evaluation was based on changes in the Harris Hip score (HHS) and Oxford Hip score (OHS) before revision and then at follow-up. The HHS measures functional ability, hip dynamics, and range of movement on scale from 0 to100 (with higher scores indicating better function) as excellent (≥90), good (89–90), moderate (79–70), and poor (<70). Thigh pain was also assessed. Radiographic parameters included leg length discrepancy (LLD), subsidence > 2 mm (calculated as the increase in distance between the apex of the great trochanter and the most lateral side of the stem shoulder between the immediate postoperative period and the last follow-up evaluation), signs of implant loosening, osteolysis in the Gruen zones, 24 defined as new, expansive radiotransparent lesions not present in the immediate postoperative period, stem in varus or valgus position (>5 mm from the anatomical femoral axis), and cortical hypertrophy or heterotrophic calcification according to Brooker’s classification. LLD was calculated using a line tangent to both ischium bones as a landmark of the pelvis position. The two parallel lines crossing the tip of the lesser trochanter of each femur, respectively, were used to measure LLD. In addition, the horizontal offset of the healthy side was calculated by comparing it with the treated side on completion of the procedure. Radiographs were evaluated independently by two orthopedic surgeons expert in septic revision. In case of disagreement, the definitive decision was made by collegial evaluation. Complications arising during the two surgical stages, during the period between the stages, and during follow-up were evaluated and recorded. For comparison of outcomes, the patients were subdivided into two groups: one with and the other without a cortical window.
Surgical technique and postoperative management
Patients were operated through the posterolateral approach; the implant was removed in a standard fashion. 23 A lateral cortical window was created for stem removal in 33 patients (Figure 1). Fenestration was performed in cases in which endofemoral removal of the stem was unsuccessful. In 66 cases, a femoral spacer (Tecres, Sommacampagna (VR), Italy) was used together with a custom-made acetabular spacer in the bone cement with antibiotic (Palacos® R + gentamicin, Heraeus Medical, Wehrheim, Germany). A short-stem femoral spacer was used in 46 cases and a long-stem spacer in the remaining 38. The choice of definitive stem type was based on preoperative planning and intraoperative evaluation of the surgical field, which can be done only after removal of the spacer and meticulous debridement. During revision implantation, six biopsies were taken for culture and one sample was obtained for intraoperative frozen section histology and definitive histology. A double mobility cup was used in 23 patients to prevent postoperative instability or dislocation. A drain was maintained in place until postoperative day 2. Patients were mobilized starting on day 2 with partial weight-bearing (50% body weight). Thromboprophylaxis with low-molecular-weight heparin and elastic compression stockings was continued until full weight-bearing. Antibiotic therapy was continued based on the sensitivity of pathogens isolated from intra and postoperative samples.

(a) Creation of a cortical window with an orthopedic bone saw, (b) femoral window with anterior-based periosteal flap, (c) the cortical window is lifted with an osteotome, and (d) white arrow indicating stem exposure of the underlying.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation and were compared using Student’s t-test for dependent and independent data. Categorical variables are expressed as the number of cases or percentage. A p value of <0.05 was considered statistically significant. Associations were evaluated using Fisher’s exact test. Implant survivorship was estimated using Kaplan–Meier analysis. The interobserver concordance was calculated using Cohen’s kappa.
Results
All patients were classified as having late-onset PJI. Table 1 presents the main demographic and surgical data. Comorbid conditions included diabetes in nine patients, rheumatoid arthritis in four patients (two of which with diabetes), substance use in four patients, cardiac disease in three patients, active neoplasia in three patients, and chronic renal insufficiency in two patients (one of which with systemic lupus erythematosus). Seventeen patients were smokers (≥10 cigarettes per day). The mean follow-up was 37.4 ± 19.7 months. Baseline microbiological data are presented in Figure 2. Two patients were implanted with a revision cementless stem, that is, two cases of de-escalation (Figure 3). Consolidation of the cortical window was completed at revision implantation (Figure 4); however, dislocation of a fragment occurred in 5 cases and radiographic persistence of the osteotomy lines, with intraoperative stability of the cortical fragment, was noted in 18 cases. The primary stem was combined with a custom-made cup in nine patients with severe acetabular bone defects. A Trilogy Trabecular Acetabular system (Zimmer-Biomet) was implanted in the remaining cases.
Demographic and surgical characteristics.

BMI: body mass index; SD: standard deviation.
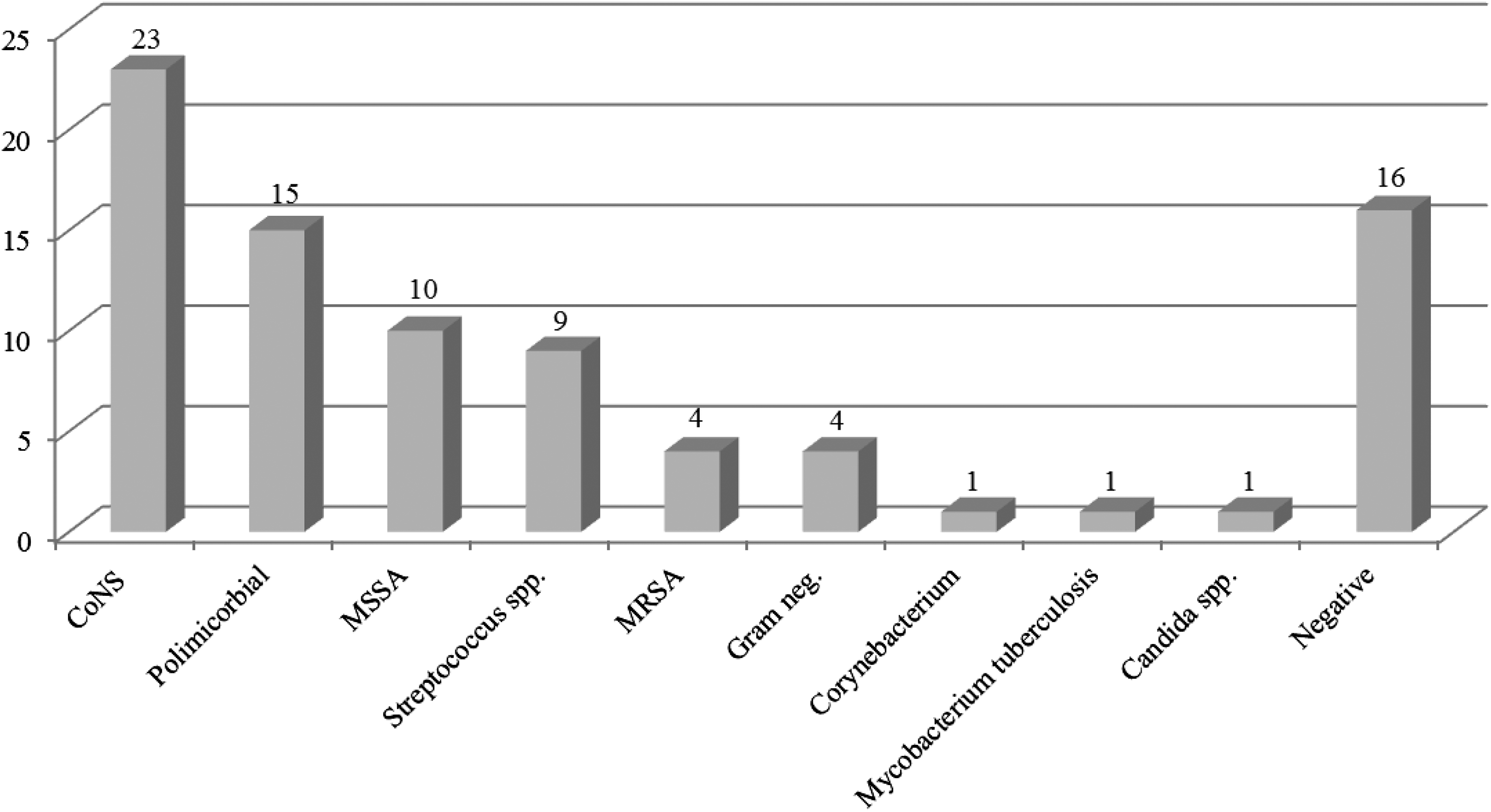
Microbiological isolates. CoNS: coagulase-negative staphylococci; MSSA: methicillin-sensitive Staphylococcus aureus; MRSA: methicillin-resistant S. aureus; Gram: gram negative.

Radiographic analysis of a case of therapeutic de-escalation. A 36-year-old man with a history of acetabular fracture treated with fixation and a PJI with MSSA. (a) Preoperative plain film; (b) immediate postoperative plain film showing long femoral spacer, acetabular spacer in place, and cortical window; and (c) control plain film at 3 months, note the good healing of the femoral window. Plain film at 1 year 2 months of follow-up showing a CLS primary stem. PJI: periprosthetic joint infection; MSSA: methicillin-sensitive Staphylococcus aureus.

Radiographic follow-up of stem removal by means of cortical window technique. (a) Preoperative plain film, AP view of femoral spacer immediately after implantation, (b) white arrows indicate osteotomy lines, and (c) evaluation at 4 months after spacer implantation showing good healing of the cortical window. Radiograph at 27 months of follow-up showing well-positioned CLS stem and consolidation of the femoral window. AP: anteroposterior.
There was a statistically significant improvement in the HHS from 41.7 ± 9.1 before to 90.8 ± 4.8 after surgery and a change in OHS from 22.9 ± 4 to 42.5 ± 3.8. All patients but one reported excellent or good results. Three patients reported thigh pain at follow-up assessment, in one of which cortical fenestration was performed. Radiographic follow-up showed no cases of implant migration or loosening. Seven patients presented with further areas of osteolysis in Gruen zone 1. No other cases of cortical hypertrophy occurred. Heterotrophic ossification was observed in six cases: four type I, one type II, and one type III. Postoperative radiographic LLD was 2.1 ± 3.9 mm in one patient with subsidence >2 mm. Three implants were classified as varus (one of which in a patient with subsidence) and one as varus. In 16 of the 84 cases (19.0%), the new stem extended the point of the previous femoral stem: the distal extension of the new stem was equal to or less than that of the previous stem. The mean horizontal offset was 54.3 ± 5.8 mm on the healthy side and 63.1 ± 7.8 mm on the operated side, with offset maintained or lateralized in all patients.
No complications during stem removal occurred. During the interstage period, spacer dislocation occurred in four patients, femoral spacer fracture in one patient, and fixation with cerclage wires of a greater trochanter fracture in one patient. No fractures occurred during the interstage interval. One Wagner Conus stem was revised on postoperative day 5 because of extensive varus positioning and was replaced with the same type of stem. Cup revision was performed on postoperative day 7 in one patient because of excessive inclination. Dislocation occurred in one patient 1 month postoperative; the dislocation was resolved with noninvasive treatment. Repeated dislocation occurred in 1 patient: optimal mid-term outcome was achieved with reoperation with substitution of the implant cup. Neither of these patients had been implanted with a double mobility cup. Two cases of implant failure due to infection occurred a fungal infection (Candida tropicalis) in one patient was successfully resolved with a second two-stage revision. In the other patient, a smoker and substance abuser, methicillin-resistant Staphylococcus aureus was isolated. A second two-stage revision was carried out but, because of persistent infection, a Gidlerstone resection arthroplasty was performed. No other specific or general complications were recorded. The total revision complications rate was 7.1%, and the Kaplan–Meier function showed a stem survival rate of 96.3%, considering as end point stem revision for any cause (Figure 5). Evaluation of patients with and those without a cortical window showed fairly comparable results at the final follow-up examination. The main differences are highlighted in Table 2. Statistically significant differences between the two groups were found for operating time for stem removal and new stem implantation. The interobserver correlations for the radiographic variables were 0.95 for subsidence, 0.91 for implant loosening, 0.83 for osteolysis, 0.89 for heterotrophic calcification, 0.96 for cortical hypertrophy, 0.92 for stem malposition, and 0.87 for LLD, with nearly complete concordance between the two surgeons.
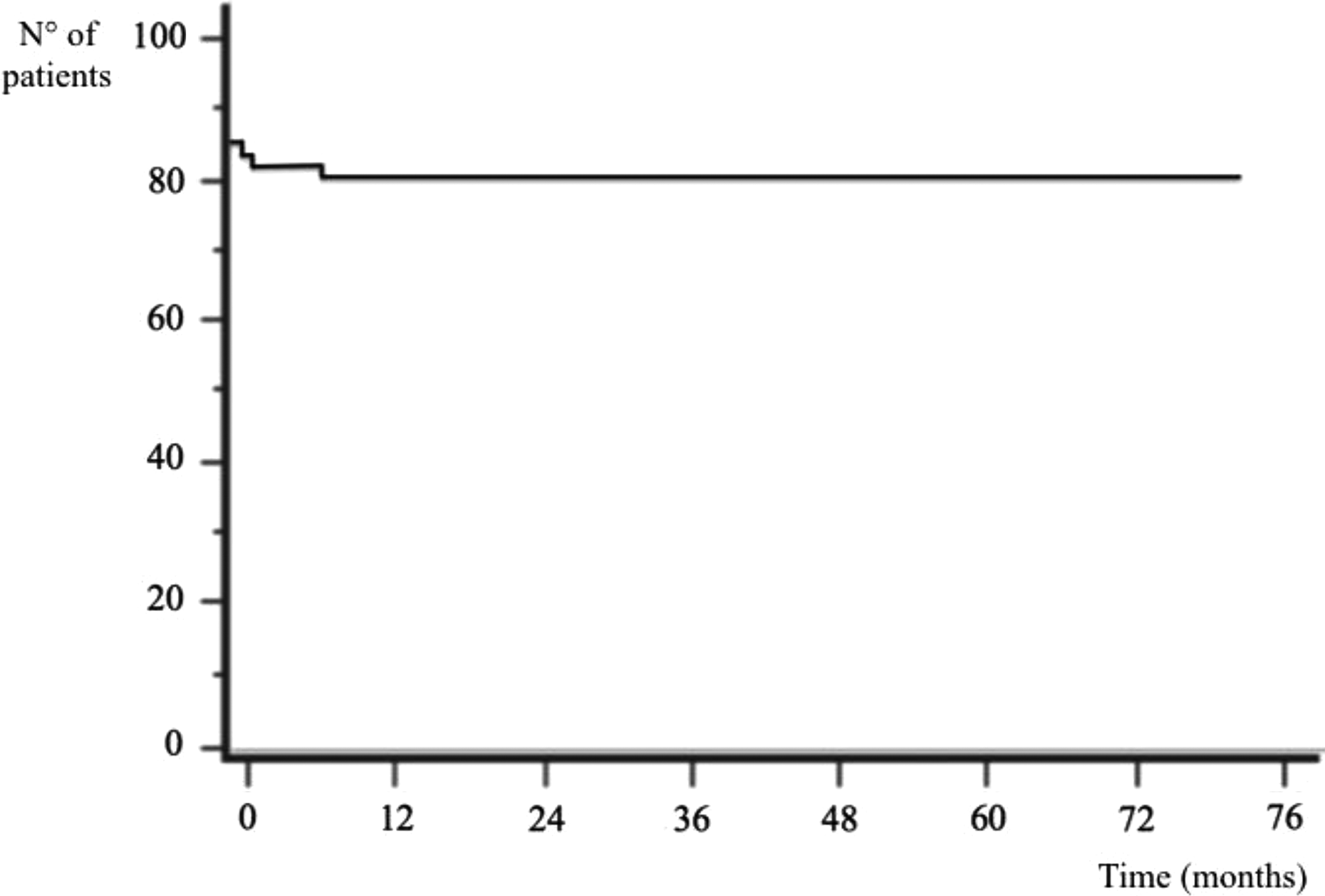
The Kaplan–Meier survival function for stem revision for any reason (n° 84) in patients treated with two-stage revision managed with primary cementless stems.
The two groups are substantially homogeneous. a
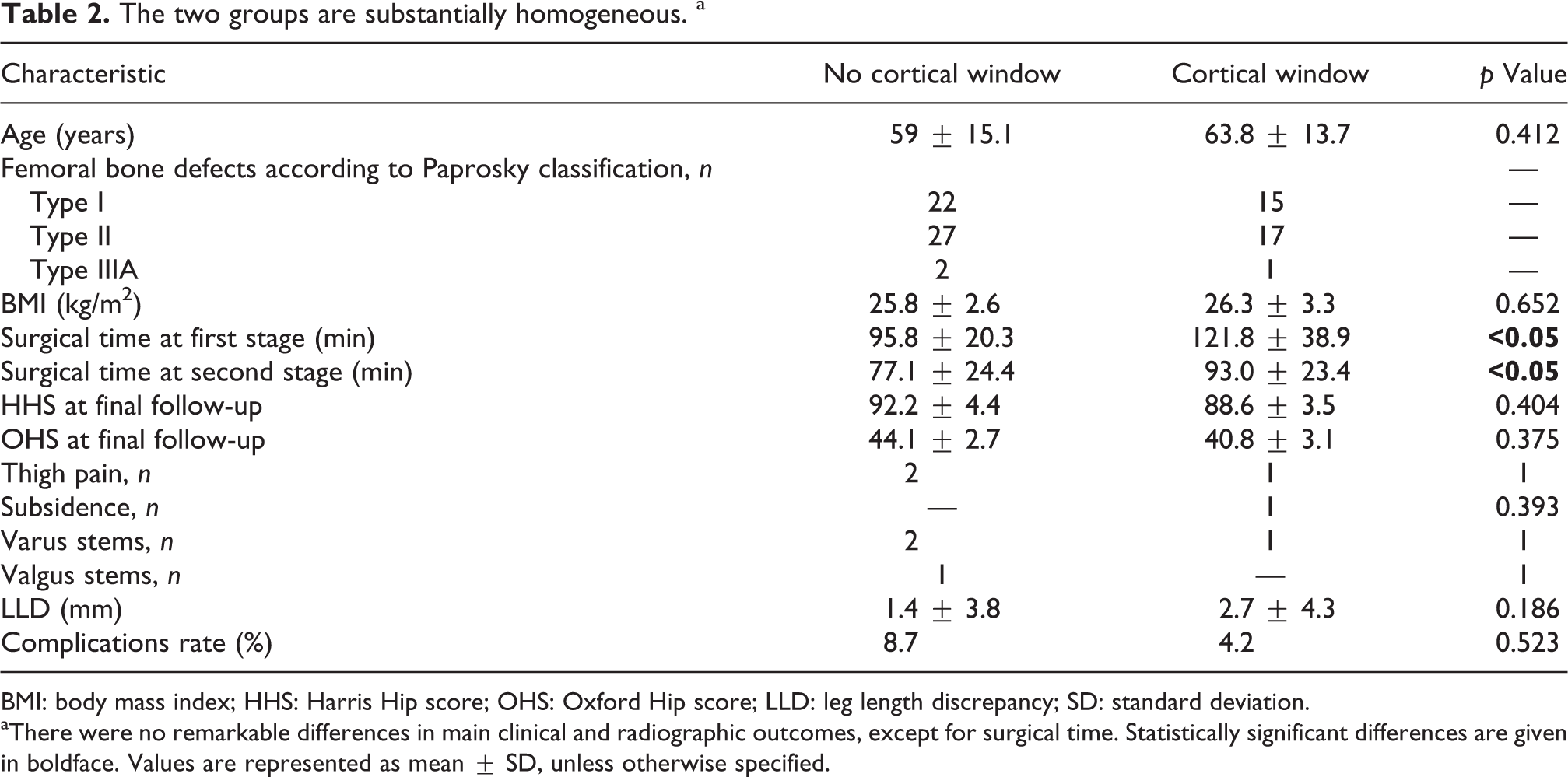
BMI: body mass index; HHS: Harris Hip score; OHS: Oxford Hip score; LLD: leg length discrepancy; SD: standard deviation.
aThere were no remarkable differences in main clinical and radiographic outcomes, except for surgical time. Statistically significant differences are given in boldface. Values are represented as mean ± SD, unless otherwise specified.
Discussion
It is a common opinion that in hip revisions, the femoral stem should extend past the femoral bone defect by at least double the cortical diameter 25 ; however, this is not borne out by the literature. Strict adherence to this idea would result in overtreatment and further damage to the femoral bone stock. The aim of the present study was to analyze the data from a cohort of patients treated with a two-stage femoral revision with a primary stem. The secondary outcomes were to (1) identify the preoperative criteria for selection of patients potentially eligible for this type of revision and (2) determine whether fenestration for stem removal can affect this type of approach. Our study is the first to date that describes this type of approach in a homogeneous group of patients treated with two-stage revision for PJI.
In 2014, Tetreault et al. 26 published their results after hip revision with a primary stem in the largest cohort treated up to then with this technique. A total of 144 patients were evaluated after 4-year follow-up to determine the percentage of revisions (Paprosky femoral bone defect types I and IIIA) that could benefit from primary stem implantation. Fifty-four cases were septic revisions, but the authors did not specify which technique they had used. Despite the optimal clinical outcomes and osseointegration of the stem in 96% of cases, there was a 9.8% re-revision rate of the femoral component, with intraoperative fracture in five patients, postoperative fracture in three patients, and implant dislocation in eight patients. Half of the patients were implanted with a primary stem. Consistent with our observations, the authors reported that the new stem need not extend beyond the point of the previous stem. Comparison of our data with the literature shows that our results are comparable with, if not better than, the average.
Globally, 63% of patients treated in the considered time period were managed with primary stems. The remainders were not suitable for this treatment mainly for the presence of massive bone defect that jeopardize the primary stem stability.
The use of primary stems in femoral revision is not new. In 1987, Pierre Vivès et al. developed the concept of de-escalation—replacement of a locked long stem with a primary stem. 27 In 2012, Miletic et al. 28 reported the mid-term outcomes with this technique: 15 patients underwent locked long-stem revision with a standard stem and femorotomy for stem removal was performed in all cases. Based on the optimal outcomes and 100% stem survivorship, the authors concluded that the technique could be considered reliable. Furthermore, as demonstrated also by our data, femoral fenestration does not affect the surgical outcome.
The problem of therapeutic escalation in revision arthroplasty was mentioned also by Pinaroli et al. 29 ; the aim of their study was to identify a subgroup of patients undergoing hip revision who could potentially benefit from the use of a primary stem. Their results are comparable with ours and share our concepts of revision and patient selection. But because only 6 of the 41 patients included in their study were classified as septic and 4 were treated with a two-stage revision, the conclusions we can draw about this patient subgroup are necessarily weak.
Tauber and Kidron 30 were the first to experiment with the press-fit CLS Spotorno cementless stem in hip revision. They implanted the stem in 24 patients (one of which septic) and obtained satisfactory mid-term results (96% implant survivorship), particularly when the trochanteric bone stock could be preserved. Other authors obtained different results with this approach using proximally hydroxyapatite (HA)-coated primary cementless stems. In 2006, Kelly et al. 31 published the results obtained in 33 revisions (six of which septic) using partially HA-coated stems. They reported that the main factors to be considered in revision with a primary stem are the presence of good diaphyseal bone stock of the lesser trochanter and at least 4 cm of diaphyseal bone at the bone–prosthesis interface. Following these criteria, the authors observed optimal osseointegration of the implant at 60 months of follow-up and a 91% stem survivorship rate (three septic failures). While our data support the need for good metaphyseal bone stock, they are contrary to the need for so large a diaphyseal engagement, as demonstrated by the optimal results obtained in patients with femoral osteotomy. Two years later, Salemyr et al. 32 published their data on 62 aseptic revisions with another type of partially coated stem. Despite the 95% implant survivorship rate, excellent or good results were obtained in only 38.3% of patients. The authors also reported a high local complications rate: thigh pain in 13.3% of patients and stem subsidence in 19 patients. More recently, Khanuja et al. 33 reported results of revision in 19 patients, 15 of which septic, treated with a two-stage revision with a proximally HA-coated cementless stem. Despite the small patient sample, the authors stated that this type of stem may be a valid surgical choice for treating patients with type I and type II Paprosky femoral bone defect. These observations are shared by Thorey et al. 34 in their study published in 2008 that reported the data on 79 revisions with an uncemented partially HA-coated primary stem at a mean follow-up of 6.8 years. Again, few firm conclusions can be drawn from such a small patient subgroup.
The complications rate in our study is in line with more recent studies. 35 The patient in whom the stem was replaced due to varus positioning had a history of acute bilateral epiphysiolysis treated with minimal fixation and osteotomy for femoral reorientation in four previous interventions. In one of the patients with implant dislocation, the underlying cause was fracture of the proximal epiphysis of femur and three previous interventions; the other patient had a Paprosky bone defect type IIIA, previous revision for repeated dislocation, plate fixation of femoral periprosthetic fracture, and five previous interventions.
As pointed out by Gastaud et al. 36 , these situations emphasize the importance of accurate patient selection. We share their observation that patient selection hinges on meticulous evaluation of bone deficiency; however, we differ in the opinion that cortical fenestration does not affect good surgical outcome.
Our study has several limitations. The retrospective design and short medium-term follow-up may constitute a bias in our conclusions. Nonetheless, the study’s strong points are the homogeneous patient cohort, the systematic evaluation of primary stems in septic patients, and the comparison between patients with and without a cortical window.
Conclusion
Based on our data, we can state that femoral revision with primary cementless stems may be considered a valid option in a subgroup of patients undergoing two-stage revision for PJI. Preoperative criteria for achieving good surgical outcome are moderate femoral bone defect (Paprosky type I or II), a low number of previous interventions (two or less), and a previous cementless femoral stem. When these criteria are followed, de-escalation may be considered if necessary. Lastly, in cases where needed, cortical fenestration does not affect the clinical outcome or the implant survivorship rate.
Footnotes
Acknowledgements
We gratefully acknowledge Avicenna s.n.c for the English version of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.