
Abstract
Purpose:
Osteoarthritis is the most common articular disease. The aim of this study was to observe the outcome after intra-articular platelet-rich plasma (PRP) injection in our patients presenting with knee osteoarthritis.
Methods:
This study was conducted in Dow University of Health Sciences, Karachi, Pakistan, from December 2014 to December 2015. All patients between 35 years and 60 years of age diagnosed with grade I and II arthritis were included in the study. Three PRP injections were injected in the knees at 4-week interval. Patients were followed up in outpatient department (OPD) and were assessed for pain and physical activity associated with arthritis using the Western Ontario and McMaster University Arthritis Index (WOMAC) score at the time of induction in the study and at 6 months interval.
Results:
Two hundred fourteen patients with the mean age of 55.15 (±6.93) years were studied. Female to male ratio was 3:1. One hundred fifty-five patients were classified as having Kellgren–Lawrence grade 1 osteoarthritis, while 59 were grade 2. One hundred eighty-nine patients had clinical symptoms for less than 2 years and 25 for more than 2 years. Mean WOMAC score before the start of treatment was 83.05, and after 6 months, it was reduced to 38.84 which was statistically significant (p = 0.000). WOMAC score was improved more in the subgroup with patients having symptoms less than 2 years (p = 0.005). Three patients developed minor hyperemia which was managed conservatively with activity limitation and ice application, but none of the patient developed gross infection.
Conclusion:
The sequential use of PRP injection for the treatment of early osteoarthritis proved to be effective in our study.
Introduction
Osteoarthritis is the most common articular disease that results from defects in articular cartilage. It affects significantly the quality of life and is one of the main causes for musculoskeletal disability. 1 Osteoarthritis can affect any joint but mostly seen in knees, hip, hands, facet joints, and feet. 2 With advancing age, there is increase in the prevalence of symptomatic knee osteoarthritis with the annual incidence being highest in people aged between 55 years and 64 years among the US population. 3
Osteoarthritis is not merely a process of cartilage wear and tear. Rather, it is a complex disease characterized by secretion of inflammatory mediators such as inflammatory cytokines which are claimed to play a leading role in the pathophysiology of this debilitating disease. 4 In a normal joint, chondrocytes remain inactive with very small turnover of the cartilage matrix. In osteoarthritis, stimulation of extracellular matrix receptors over chondrocytes transforms them into activated chondrocytes. They exhibit cellular proliferation and cluster formation and produce matrix degrading proteinases and inflammatory cytokines. 5 In addition to cartilage destruction, osteoarthritis is also characterized by synovial inflammation, subchondral sclerosis, ligament laxity, and osteophyte formation. 6 The series of these pathological changes in all joint tissues led to the consideration of osteoarthritis as a disease of joint as an organ. 5
There have been a number of supportive treatments for osteoarthritis including analgesics, viscosupplements, and corticosteroids that are used to alleviate the symptoms of arthritis. 7 Intra-articular hyaluronic acid is also another treatment option being utilized for long in this regard. 8 Recently, there is increase in the use of platelet-rich plasma (PRP) for the treatment of osteoarthritis. PRP derived from autologous blood containing growth factors is claimed to activate the healing process in damaged cartilage and helps in tissue regeneration. 9,10 Comparing both hyaluronic and PRP injections, some studies support PRP to be superior in terms of symptomatic relief. 11,12
The aim of this study was to observe the outcome after intra-articular PRP injection in our patients presenting with knee osteoarthritis.
Materials and methods
This study was conducted in Dow University Hospital, Dow University of Health Sciences, Karachi, Pakistan, from December 2014 to December 2015 after approval from institutional review board. All patients between 35 years and 60 years of age diagnosed with grade I and II (Kellgren–Lawrence 13 ) osteoarthritis, symptoms persisting for more than 6 months, having hemoglobin above 12 g dL−1, platelets above 150,000 µL−1, and failure of pharmacological agents and physiotherapy for significant long-term relief were included in the study. Patients having autoimmune/platelet disorders, under treatment with anticoagulants or immunosuppressive therapy, history of diabetes mellitus, infection, recent trauma, or malignancy were excluded. According to inclusion criteria, all patients presenting in outpatient clinics were briefed in detail about the procedure, possible benefits, and complications related to the procedure and included after written and informed consent. A questionnaire was designed and the data regarding demographics, occupation, body mass index, blood group, duration of symptoms, and grade of arthritis were recorded. Patients were assessed for pain and physical activity associated with arthritis using a Western Ontario and McMaster University Arthritis Index (WOMAC) score. 14
Dhurat and Sukesh 15 described two methods for preparation of PRP using differential centrifugation, namely PRP method and buffy-coat method. We utilized PRP method in our study group. Patients were registered with the orthopedic department, and PRP was prepared in hematology department at Dow University of Health Sciences, Karachi, Pakistan. Blood was drawn from patient’s cubital vein to make 4–6 mL of PRP. Blood samples were collected in bags containing anticoagulant (citrate phosphate dextrose and adenine). The collected blood samples were then transferred into a tube and centrifuged at a constant acceleration to separate the red blood cells (RBCs) from whole blood volume. It separates blood in three layers (platelets with white blood cells (WBCs), buffy coat rich in WBCs, and RBCs from top to bottom). Then, the upper layer and superficial buffy coat are centrifuged again in a new sterile tube sufficient enough to form soft pellets at the bottom. Upper two-thirds of this centrifuged volume is discarded, while the remaining lower one-third is homogenized to make PRP. The PRP was dispensed in a sterile syringe.
Patients were given appointment in outpatient department (OPD) for PRP injection. Under aseptic technique, PRP was injected in the knees through supralateral approach in suprapatellar pouch. After given with injection, patients were observed for 20 min and discharged home with clear instructions for signs of infection including increasing pain, redness, warmth, and inability to bear weight. Patients were prescribed paracetamol in case of pain and advised not to take nonsteroidal anti-inflammatory drugs and steroids. Patients were followed up in OPD on regular basis. A total of three injections were given to each patient at 4 weeks interval. WOMAC score was calculated at the time of induction in the study and at 6 months interval to assess the effect of PRP injection.
Data were presented as frequencies. WOMAC score at the start of treatment was compared with the final score using paired t-test and in-between subgroups using independent t-test.
Results
A total of 225 patients were registered for this clinical trial based on the inclusion criteria. At the end of the trial, 214 patients completed the study period, while 11 patients did not complete the study period and lost to follow up. The mean age of the patients was 55.15 (±6.93) years. Females outnumbered males in presenting with knee osteoarthritis. There were 144 (67.3%) females and 70 (32.7%) males. Female to male ratio was 3:1. One hundred fifty-five (72.4%) patients were classified as having Kellgren–Lawrence grade 1 osteoarthritis, while 59 (27.6%) were grade 2. Most of the patients (n = 189; 88.31%) had clinical symptoms for less than 2 years and 25 (11.7%) for more than 2 years. Seventy-six patients (35.5%) had A+ve blood group, 100 (46.7%) had O+ve blood group, and 36 (16.8%) had AB+ve blood group. The mean WOMAC score before the start of treatment was 83.05 (±4.3) and after 6 months it was reduced to 38.84 (±5.5), which was statistically significant (p = 0.000; Table 1). WOMAC score was improved more in the subgroup with patients having symptoms less than 2 years (p = 0.005). There was no significant difference in the WOMAC score at 6 months among males or females (p = 0.071) and subgroups with Kellgren–Lawrence grade 1 or 2 (p = 0.113; Table 2). Three patients developed minor hyperemia which was managed conservatively with activity limitation and ice application, but none of the patient developed gross infection.
Difference between WOMAC score at the start of treatment and at 6 months follow-up.
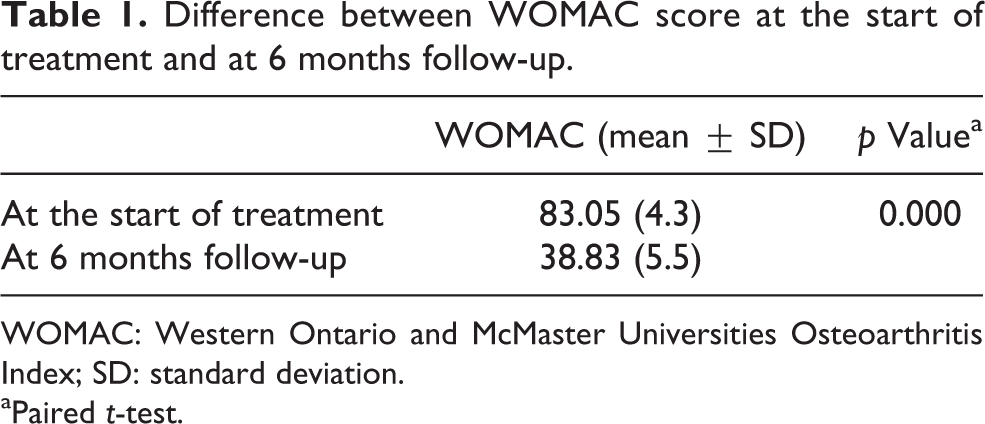
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; SD: standard deviation.
aPaired t-test.
Comparison of WOMAC score after 6 months between subgroups.
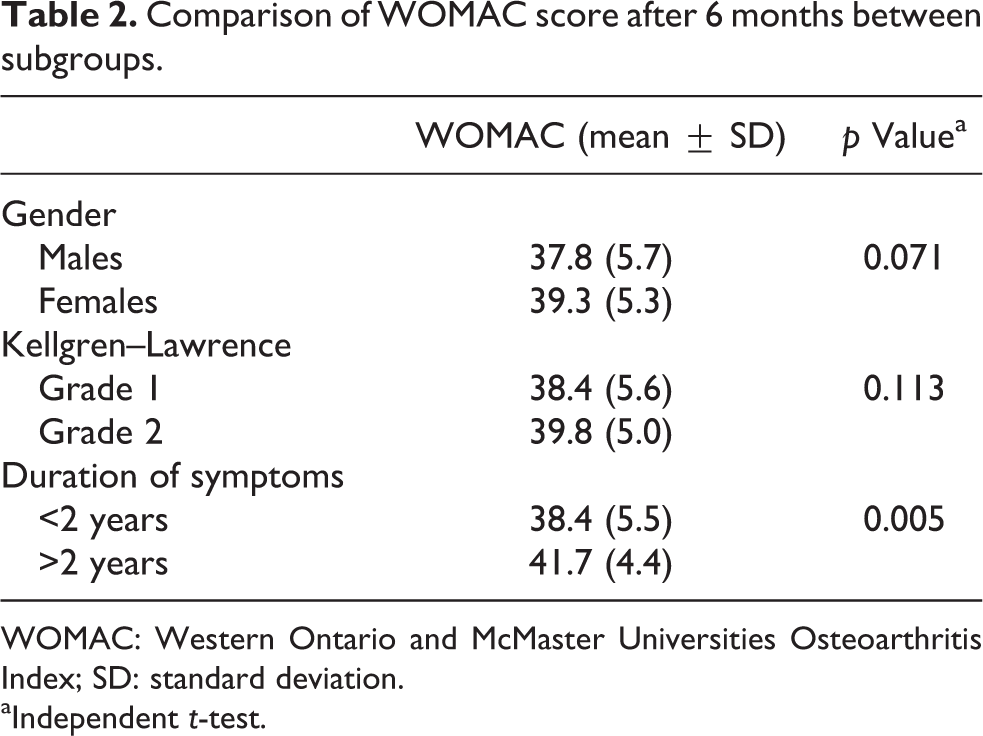
WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; SD: standard deviation.
aIndependent t-test.
Discussion
In this study, there was remarkable clinical improvement among patients with arthritis who received PRP injection. Difference in WOMAC score at 6 months interval was significant. Patients having symptoms for less than 2 years showed more improvement in WOMAC score.
Osteoarthritis is a debilitating disease affecting the mobility and quality of life among individuals. Nonsurgical treatments including PRP, corticosteroids, and hyaluronic acid have been prescribed by physicians with good short-term results. There has been increasing interest in biological and regenerative methods including PRP. 16,17 However, it is to be noted that any invasive procedure may have some placebo effect. To better understand the effect of each treatment modality, it is always recommended to have a comparative group in any trial. Unfortunately, in our study, we did not have any comparative group with other mode of treatment. But in the literature, there are some comparative studies and meta-analyses favoring the use of these modalities with favorable outcomes.
A recent systematic review and meta-analysis by Sadabad et al. showed superior efficacy for PRP as compared to hyaluronic acid in alleviating the clinical symptoms over a period of 2 years. However, they recommended the need of long-term studies for the effects of PRP. 12 Another systematic review by Khoshbin et al. shows that multiple sequential PRP injections have better symptomatic relief as compared to hyaluronic acid or normal saline solution at 6 months follow-up. 18 In our study also we found significant improvement in the WOMAC score in patients with PRP injections at 6 months interval. PRP therapy is minimally invasive and a simple alternative, being used to enhance the healing process and tissue regeneration. It has the potential to improve the quality of life, relieve pain, and enhance knee joint function. 19
Kon et al. studied the effects of PRP injection in the treatment of chronic degenerative condition of the knees. They studied the effects in 115 patients at 6 and 12 months follow-up. There was an overall significant improvement at 6 and 12 months interval. However, they observed that in the initial 6 months, the results were stable; in the second half (7–12 months), the results became worse at 12 months as compared to the first 6 months. In addition, the results were better in patients with early grade of arthritis. 20 In our study, we had favorable results at 6 months, but our overall study duration was shorter (i.e. 6 months follow-up only). Secondly, we had selected patients with early arthritis (Kellgren grade 1 and 2).
Jang et al. presented the outcome of his 65 patients who were treated with PRP injection. There was improvement in Visual analogue scale (VAS) and International Knee Documentation Committee (IKDC) scores; however, the developing degeneration in the joint had been associated with reduced clinical effects of PRP. The results were better in younger age-group with early osteoarthritis. 21 In our study, the study group was relatively younger (mean age, 55.15 years) with early arthritis and showed significant improvements at 6 months follow-up.
Patel et al. compared the effects of PRP in three subgroups and concluded that there was a significant improvement in patients receiving either single (group A) or two (group B) PRP injections. The third group (group C), received normal saline instead of PRP, showed deterioration of symptoms. Mild complications including nausea and dizziness were observed in some patients but for shorter duration. 22 In our study, unfortunately, there was no comparison group, but PRP injection showed significant clinical improvement. Mild hyperemia was observed in three patients but managed conservatively.
The effects of PRP had been compared with hyaluronic acid in various studies. Kon et al. 9 reported better outcome with PRP in younger patients with early arthritis as compared to hyaluronic acid. Filardo et al. compared the effects in 192 patients and concluded that there was no significant difference in both modes of treatment. 23 Cole et al. compared both the injection modalities in 111 patients. There was no significant difference in the WOMAC score of both groups (primary outcome measure); however, there were better results with PRP in other outcome measures. 24 In contrary to these individual studies with mixed results, some of the systematic reviews favor PRP beneficial over hyaluronic injections. 12,18
There were some limitations of this study including short follow-up and no comparison group.
Conclusion
The sequential use of PRP injection for the treatment of early osteoarthritis proved to be effective in our study. However, larger studies are required to observe the long-term effects in patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.