
Abstract
Background:
End-stage renal disease is an independent risk factor for postoperative mortality and cardiovascular events, but dialysis vintage and its relationship with perioperative complication is not well studied. We did a population-based study to investigate this issue.
Materials and methods:
We identified patients who had total knee arthroplasty (TKA) or total hip arthroplasty (THA) surgeries during 1999–2010 from the National Health Insurance Research Database of Taiwan. Patients who had regular dialysis before surgery were recruited in our analysis. The outcome of interest was mortality, morbidities, intensive care unit admission rate, hospitalization duration, readmission rate, and medical costs. We did multivariate regression to adjust for age, sex, and Charlson comorbidity index (CCI) and to analyze the relationship of dialysis vintage and clinical outcomes.
Results:
A total of 518 patients were enrolled for analysis. A total of 286 patients had TKA surgeries and 232 patients had THA surgeries. Patients who had TKA surgery were older and had more medical comorbidities than patients who had THA. After adjustment for age, sex, and CCI, TKA patients who had dialysis vintage <3 years had significantly higher medical costs (p < 0.05). For THA patients, dialysis vintage is not an independent risk factor for outcomes of interest.
Conclusion:
Perioperative complication is associated with age and medical comorbidities. Longer dialysis vintage is not related to perioperative morbidities and mortalities or higher medical costs in either TKA or THA patients.
Introduction
End-stage renal disease (ESRD) is a well-known risk factor for perioperative complications. In a meta-analysis of elective noncardiac surgeries, patients with chronic renal disease are independent risk factors for postoperative mortality and cardiovascular (CV) events. The incidence of complication is two to five fold higher than those with normal renal function. 1 With the improvement of renal replacement therapy (RRT), survival in dialysis patients increases, together with their chances for receiving other surgeries.
Long-term hemodialysis (HD) patients may develop renal osteodystrophy and β2-microglobulin amyloid deposition in and around joints. For dialysis patients, osteoarthritis is the most common indication for total knee replacement arthroplasty (TKA) or total hip arthroplasty (THA). 2 The incidence of avascular necrosis or amyloid-related arthropathy is also increased in HD patients. 3 In the United States, the cumulative incidence for dialysis patients having THA is six times higher than general population. 4 Despite higher perioperative risk, TKA or THA does relieve pain and increase function and is considered a valid option with careful medical management. 5,6
Although ESRD is a well-known risk factor for perioperative complications, dialysis vintage was not fully studied as an independent risk factor before. Previous studies on HD patient with TKA or THA had a wide range of HD vintage, ranging from 1 year to 28 years. 2 Chronic renal failure promotes hypertension and dyslipidemia, causing endothelium damage, and is known to associate with higher CV events. 7 However, other study showed that the long-term dialysis was only associated with a modest increase in risk of CV mortality. 8 We wanted to explore whether dialysis vintage is associated with increased perioperative risk of dialysis patients who need TKA or THA through a population-based study.
Materials and methods
Data set and study population
The National Health Insurance Research Database (NHIRD) contains de-identified registration files and original claims data of reimbursements from the Taiwan National Health Insurance (NHI) program. Details regarding the nature of data obtained from the NHIRD were described in our previous study. 9 In brief, the data set we used was a random sample from all individuals who had kidney diseases or severe neurological diseases between 1997 and 2011, with the sampling fraction being as high as 71%. The quality of NHIRD data is widely recognized, and the data have been used in clinical epidemiology and health service research. 10
Based on this data set consisting of two million patients, we constructed a sample for the current study. Firstly, we screened adult patients (≥20 years old) who received TKA or THA between 1999 and 2010. Secondly, we defined ESRD by maintenance dialysis for >3 months. We recruited TKA and THA patients who fit ESRD definition before surgery in our analysis.
Ethics statement
To keep individual information confidential to satisfy regulations on personal privacy in Taiwan, all personal identification numbers in the data were encrypted by converting the personal identification numbers into scrambled numbers before data processing. This study was exempt from full review by the National Taiwan University Hospital Research Ethics Committee, and the need for informed consent was waived because the data used in this study consisted of de-identified secondary data released for research purposes and were analyzed anonymously, which complies with the regulations of the Department of Health, Executive Yuan, Republic of China.
Variables
To investigate the relationship between vintage duration and perioperative outcome, we divided our patients into two groups by vintage ≤3 years and vintage >3 years. We also did sensitivity tests with cut point of 5-year vintage, and the results were similar to grouping by 3 years. To control for the potential confounding effect resulting from the imbalance in clinical characteristics, we calculated the Deyo’s Charlson comorbidity index (CCI). 11,12 This index is a weighted measure that incorporates 17 different medical categories, all of which affect mortality. For each patient, we identified preexisting comorbidities based on the presence of admission diagnostic codes (i.e., International Classification of Disorders 9th revision-CM codes) in their claims data in the NHIRD. Their diagnosis was acquired by tracking the ambulatory medical care and inpatient records in the NHI database in the year before the index admission surgery. The case ascertainment for these medical comorbidities was defined from ≥1 hospital discharge or ≥3 ambulatory visits with a relevant principal or secondary diagnosis code.
Study outcomes
A 30-day death was the primary outcome of interest. The date of death was defined from the records in the registry of catastrophic illnesses or the discharge status (death or critically ill discharge). The secondary outcomes included pneumonia (ICD-9-CM 480–486), septicemia (ICD-9-CM 038 and 998.5), stroke (ICD-9-CM 430–438), postoperative bleeding (ICD-9-CM 998.0, 998.1, and 998.2), deep wound infection (ICD-9-CM 958.3), acute myocardial infarction (ICD-9-CM 410), pulmonary embolism (ICD-9-CM 415), and urinary tract infection (ICD-9-CM 599.0). We also compared the hospitalization duration, medical costs, intensive care admission rate, readmission rate 90 days after discharge for patients with different dialysis duration.
Statistical analysis
The χ 2test, Fisher’s exact test, and Student’s t-test were used to examine differences in demographic variables, medical comorbidities, and clinical outcomes between the patients with different dialysis duration. Multivariate linear regression analyses and multivariate logistic regression analyses were used to adjust for age, sex, and medical comorbidities (presented by CCI) to reveal the influence of dialysis duration on clinical outcomes. An α level of 0.05 was considered statistically significant for all analyses. The analyses were performed using SAS 9.4 software (SAS Institute, Cary, North Carolina, USA).
Results
The patient selection processes are shown in Figures 1 and 2 for TKA and THA cohort, respectively. In our database, 0.7% of these TKA patients had long-term dialysis and 2.1% of these THA patients had long-term dialysis. The demographic data and clinical characteristics of the dialysis patients who had TKA or THA surgeries are presented in Tables 1 and 2, respectively. The comparison of TKA and THA patients with dialysis are presented in Table 3. TKA patient was about 10 years older (p < 0.001) and had higher CCI score (p < 0.05) than patients who had THA. More THA patients had their surgeries in teaching hospital (p < 0.05).
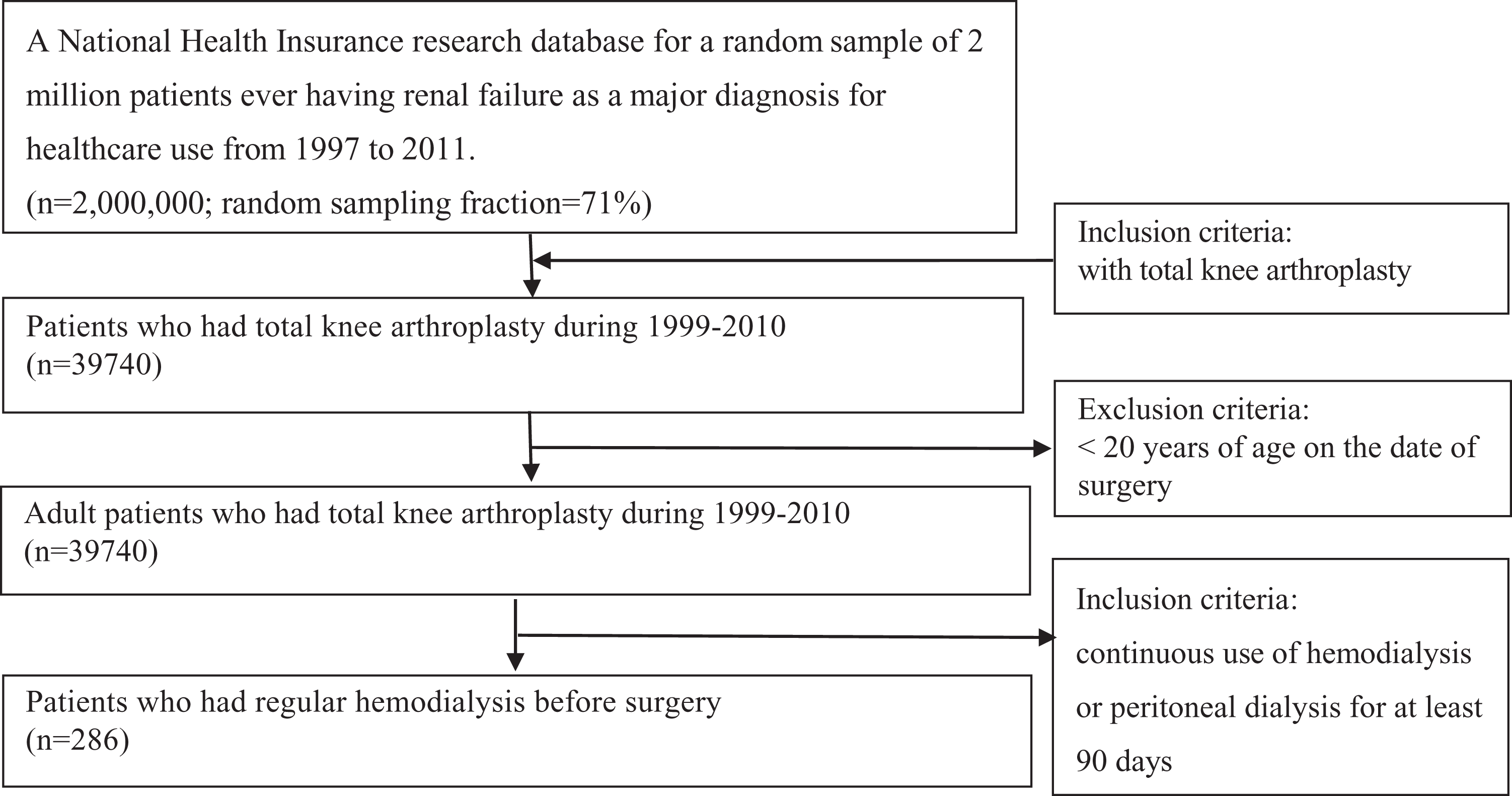
Flowchart of total knee arthroplasty patient selection.
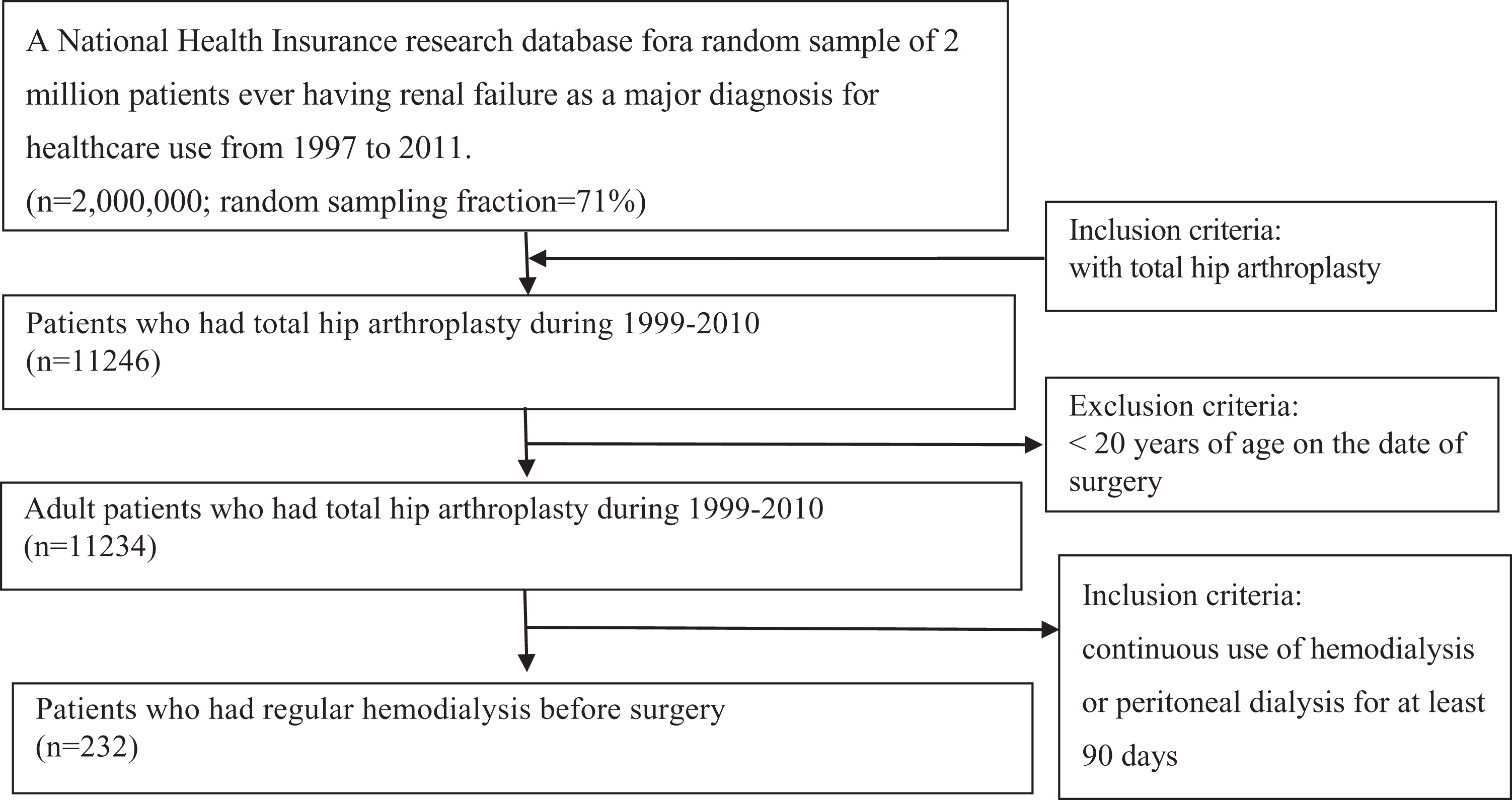
Flowchart of total hip arthroplasty patient selection.
Demographics data of dialysis patients with TKA.

TKA: total knee replacement arthroplasty; CCI: Deyo’s Charlson comorbidity index; SD: standard deviation.
Demographics data of dialysis patients with THA.

THA: total hip replacement arthroplasty; CCI: Deyo’s Charlson comorbidity index; SD: standard deviation.
Demographic data and clinical outcomes of dialysis patients who received TKA or THA.

TKA: total knee replacement arthroplasty; THA: total hip replacement arthroplasty; CCI: Deyo’s Charlson comorbidity index; SD: standard deviation.
aComposite complication: one of the following diagnosis was made during surgical admission: pneumonia, septicemia, stroke, postoperative bleeding, deep wound infection, acute myocardial infarction, pulmonary embolism, urinary tract infection.
The average age of patients who had TKA was 67.9 ± 8.7 years. Female patients comprise 67.8% of the TKA surgical population; 45.1% of the TKA patients had dialysis vintage <3 years (Table 3), and the CCI was significantly higher in patients who had shorter dialysis vintage (CCI 3.7 ± 1.7 vs. 3.4 ± 1.7; p < 0.05) (Table 1). There was no difference in physician age and operation hospital level in short or long dialysis vintage groups.
THA patients who had long-term dialysis were 57.6 ± 13.3 years. There were more female patients than male (female vs. male = 61.2% vs. 38.8%). CCI was significantly higher in patients who had shorter dialysis vintage (CCI 3.5 ± 1.5 vs. 3.0 ± 1.4; p < 0.05). Patients who had longer dialysis vintage received their operation at teaching hospital more than patients who had shorter dialysis vintage (97.06% vs. 88.54%; p < 0.01; Table 2).
Surgical mortality in TKA and THA was comparable (3.5% vs. 1.72%; p = 0.22), but readmission rate was higher in the THA group (TKA vs. THA = 24.83% vs. 32.76%; p < 0.05). The hospital stay in TKA or THA group was similar, but the costs of hospitalization was higher in TKA patients (p < 0.05; Table 3).
For TKA patients, 30-day mortality, the intensive care unit (ICU) admission rate, and 90-day readmission rate were not different in vintage <3 years or >3 years groups. However, TKA patient with vintage <3 years stayed in the hospital for about one and half more days longer (p < 0.05) and had higher medication costs (p < 0.05) compared with patients who had vintage >3 years (Table 4).
Clinical outcomes for TKA patients with different vintage.

TKA: total knee replacement arthroplasty.
aComposite complication: one of the following diagnosis was made during surgical admission: pneumonia, septicemia, stroke, postoperative bleeding, deep wound infection, acute myocardial infarction, pulmonary embolism, urinary tract infection.
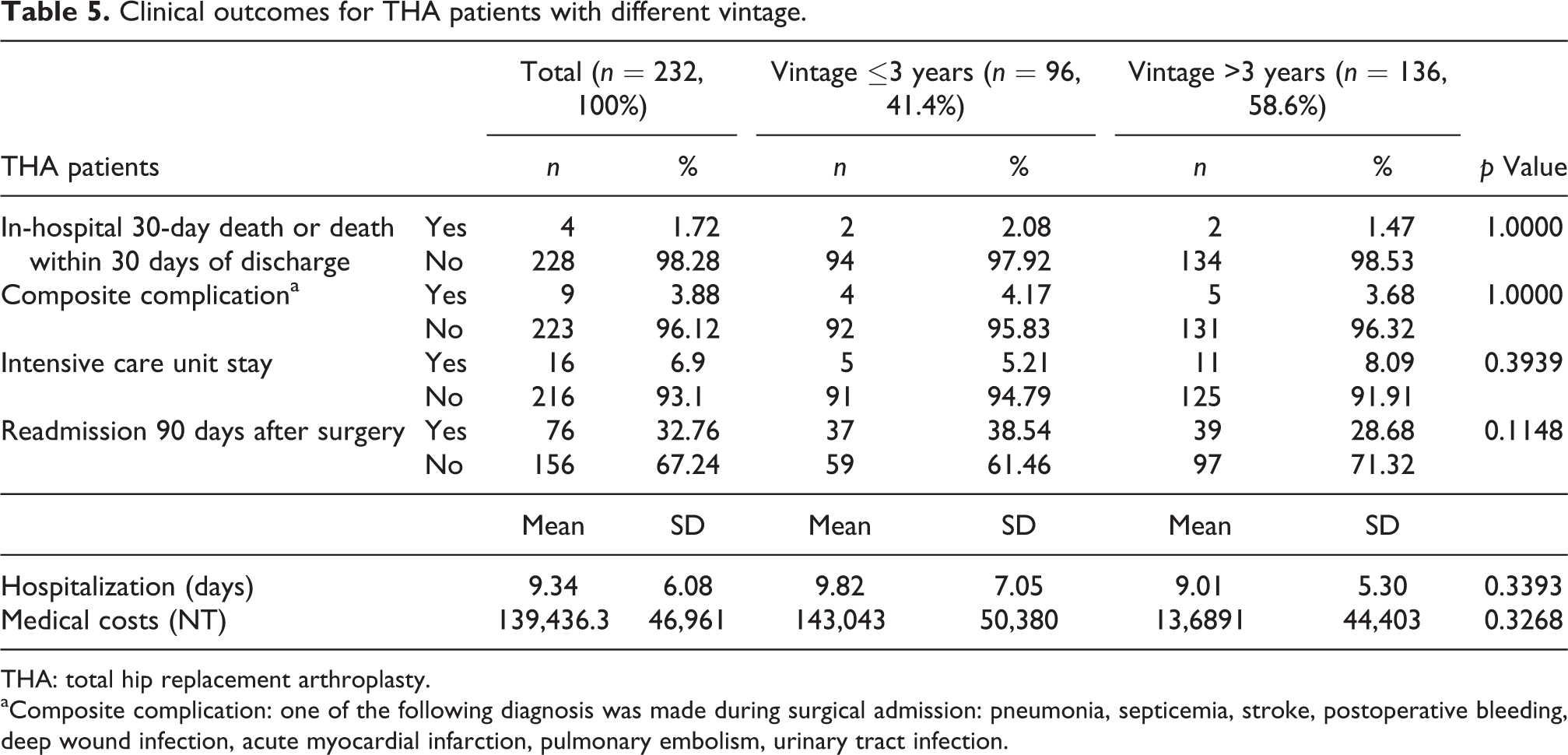
In THA patients, dialysis vintage <3 years or >3 years does not affect the difference in 30-day mortality, complication rate, ICU stay, readmission 90 days, the hospitalization days, and medical costs (Table 5).
Clinical outcomes for THA patients with different vintage.
THA: total hip replacement arthroplasty.
aComposite complication: one of the following diagnosis was made during surgical admission: pneumonia, septicemia, stroke, postoperative bleeding, deep wound infection, acute myocardial infarction, pulmonary embolism, urinary tract infection.
We did multiple linear regression and multivariate logistic regression to adjust the effect of age, sex, and CCI (Table 6). In TKA patients, 30-day mortality was associated with older age (odds ratio 1.137, 95% CI 1.021–1.266). Patients with higher CCI had more ICU admission, longer hospitalization, and medical costs. After adjustment for age, sex and CCI, shorter dialysis vintage was associated with longer hospitalization and higher medical costs. In THA patients, 30-day mortality, ICU admission, 90-day readmission, and medical costs were associated with higher CCI score. Dialysis vintage is not affecting the above outcomes in THA patients after adjustment for age, sex, and CCI.
Multivariate regression models for TKA and THA patients.

TKA: total knee replacement arthroplasty; THA: total hip replacement arthroplasty; N.A.: not available; ICU: intensive care unit.
aComposite complication: one of the following diagnosis was made during surgical admission: pneumonia, septicemia, stroke, postoperative bleeding, deep wound infection, acute myocardial infarction, pulmonary embolism, urinary tract infection.
Discussion
In the present study, we showed that longer dialysis vintage did not increase 30-day mortality, complication rate, 90-day readmission rate, ICU admission, hospitalization days, and medical costs in patients who had TKA or THA surgeries.
In Taiwan, the life expectancies of peritoneal and hemodialysis patients after the start of dialysis were reported to be 7.9 and 8.7 years. 13 With improving medical treatment and survival, patients with ESRD are more likely to keep their life quality while remaining on dialysis for more years than in the past. ESRD is associated with significant alterations in CV function; homeostasis of body fluid, electrolytes, and acid–base equilibrium; bone metabolism, erythropoiesis; and blood coagulation. Thus, despite improvement in RRT, ESRD is associated with higher perioperative CV mortality than non-ESRD patients in either cardiac or noncardiac surgeries. 14 –16
The influence of ESRD on CV events was supposed to increase with ESRD duration. Dialysis vintage with peritoneal dialysis(PD) <2 years is associated with better hydration, nutritional state, and survival, and the benefit was not found in PD patients who had vintage longer than 4 years. 17 A cause-specific mortality study on dialysis vintage demonstrated that longer dialysis vintage is related to a higher risk for infection-related mortality with worse outcome observed with vintage >30 years. 8 Whether dialysis vintage is associated with higher perioperative CV events or mortality was not fully investigated before. Our results suggested that longer dialysis vintage was not associated with major complications.
Earlier studies showed that long-term dialysis patients had high infection rate and early complications in THA. 18 Furthermore, surgical death was usually not related to the index procedure, but to patients’ medical comorbidities. 9 –11 In our study, longer dialysis vintage did not contribute to higher surgical mortality or composite complication rate. Instead, higher CCI, which was a surrogate for more medical comorbidities, was associated with more ICU stay and medical costs in either TKA or THA. We suggest that to evaluate the perioperative risk of dialysis patients, we should emphasize more on patients’ age and medical comorbidities, but not dialysis vintage.
Since the present study is a population-based study, this enabled us to establish an association between dialysis vintage and perioperative risk. However, several limitations should be addressed. First, the diagnosis of medical comorbidities in our study was entirely determined by the ICD codes from the NHI claim database and there may be concern about the diagnostic accuracy of the database. However, the Bureau of the NHI has formed different audit committees that randomly sample the claim data from every hospital and review charts on a regular basis to verify the diagnostic validity and quality of care. Accordingly, the NHI claim database is an established research database and has been used in various biomedical research fields. Moreover, we used case ascertainment algorithms that required at least two ambulatory medical care visits with a relevant diagnosis code to validate the diagnosis, which might be expected to provide adequate diagnostic accuracy. 19 Second, dialysis patients comprised a complex group of patients who suffered from different etiology of renal failure, and their dialysis conditions vary from person to person. For example, duration of the dialysis procedure is an important element in determining patient mortality, 20 but this information is not obtainable in our database. Third, due to the inherent limitations of the NHI database, information was lacking regarding lifestyle factors, such as smoking, alcohol consumption, and obesity, which is important for perioperative risk assessments. Nevertheless, we did multivariate regression to adjust for possible confounding factors. Finally, most inhabitants of Taiwan are of Chinese ethnicity, and it is uncertain whether our findings can be generalized to other ethnic groups. Since it is a retrospective study, we could not exclude the possibility of selection bias. Patients’ fitness, willingness, previous drug therapy, and orthopedic surgeons’ evaluation on dialysis patients may interfere with our interpretation of end-point analysis. 21
Conclusion
Longer dialysis vintage is not related to perioperative morbidities and mortalities or higher medical costs in patients receiving TKA or THA. Surgical mortality and perioperative complications are associated with advanced age and medical comorbidities for TKA patients and TKA patients are older than THA patients. In contrast, medical comorbidities in patients receiving THA are the main risk factor for surgical mortality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.