
Abstract
Aim:
This retrospective study is aimed to analyze the effect of ultrasound-guided platelet-rich plasma (PRP) injections on grade 2 intrasubstance meniscal degenerations (IMDs).
Materials and Methods:
Fifteen patients who underwent PRP injections for symptomatic grade 2 meniscal lesions were included in the study. All injections were performed with ultrasound in the degenerated menisci. Patients were evaluated with Lysholm score and magnetic resonance imaging (MRI) before the injection and after a mean of 32-month follow-up. T2-weighted MRI images were evaluated on sagittal by two authors as double-blind.
Results:
Lysholm score was found to be statistically significantly increased, and in 67% of the patients, grade 2 degenerations were improved to grade 1.
Conclusion:
Intra-meniscal PRP injection under ultrasonography guidance provides good functional scores and radiological improvement in the patients with IMD.
Introduction
Reicher et al. classified meniscal lesions in four grades (0–3) on magnetic resonance imaging (MRI) images. 1 Grade 1 lesions are defined as mucoid degenerations without the signs of ruptures. Physical therapy is an accepted treatment approach for this kind of lesion. 2,3 Grade 3 lesions extend to the articular surface and are considered as meniscal ruptures. The surgical treatment may be an option in these meniscal lesions if conservative treatment fails. 4,5 However, grade 2 lesions are linear signal changes within the meniscus which does not extend to the joint surface. 6 These lesions are commonly accepted as intrasubstance meniscal degenerations (IMDs). 6,7 Generally, patients with IMD are asymptomatic. 8 –10 On the other hand, in some cases, IMD may present with the symptoms of typical meniscal tears and may lead to reduced physical activities. Furthermore, these lesions can be considered a pre-stage meniscal rupture and possibly turn into full thickness tears. 8,11 Today, there is still no consensus on the treatment modalities of symptomatic IMD and the controversy remains. Conservative treatment of IMD is often not satisfactory. 7,12 However, surgical treatment is not a suitable alternative for these lesions that do not reach joint surface. Therefore, there is a need for new treatment methods in IMD.
Platelet-rich plasma (PRP) is used in many areas of medicine for its positive effect on tissue healing. In recent years, it has also been used in the treatment of various meniscal injuries. 8,13,14 PRP may also be a promising method of treatment for IMD because it can be applied as minimal invasive and demonstrates ability to tissue healing. PRP can be delivered to the lesion within the meniscus when applied through ultrasound guidance. However, the effect of ultrasound-guided PRP injection in IMD is still unclear.
The aim of our study is to evaluate the efficiency of ultrasound-guided PRP injection on radiological and functional outcomes in IMD. Our hypothesis is that PRP will contribute to clinical and radiological improvement in patients with IMD.
Materials and methods
After approval from the institutional review board, 23 patients with intrasubstance meniscus degeneration who underwent PRP treatment between February 2013 and December 2014 were reviewed retrospectively. Patients with ligamentous injuries, instability, flexion or extension contractures, mechanical axis deviation of more than 10 mm, and grade 2 or higher osteoarthritis according to Ahlbäck classification 15 were excluded from the study. Patients with pregnancy, systematic diseases, rheumatologic symptoms, and bleeding disorders were also excluded from the study.
PRP was obtained with T-LAB PRP kit (T-Biotechnology Laboratory, Istanbul, Turkey) which provides 4.75 times higher concentration of platelets compared to blood. It could be classified type 2b according to Mishra et al. 16 Two 10-ml kit tubes have been centrifuged on 1500 × g for 8 minutes. Four ml of PRP were obtained.
All injections were performed by the same author under ultrasonography (USG) guidance. Dynamic coronal images were obtained when the knee was in 30° flexion 17 (Figure 1). The linear probe of USG (Esaute MyLab Five, Geneva, Italy, 2010) was used with 5–15 MHz frequency for visualization. An 18-gauge spinal needle was used. PRP injected into the hypoechoic lesions ensuring proper sterilization conditions (Figure 2).
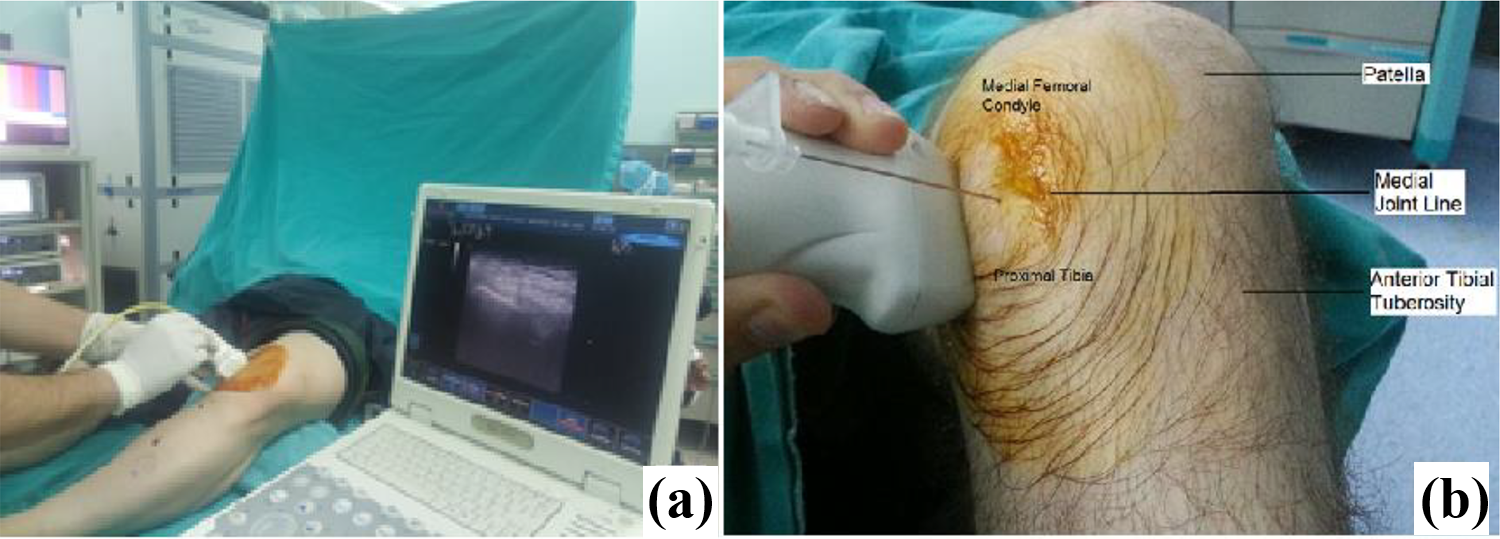
(a) PRP injection was applied under ultrasonography when the knee was in 30° flexion. (b) Ultrasound-guided injection of PRP and anatomical landmarks of the knee. PRP: platelet-rich plasma.
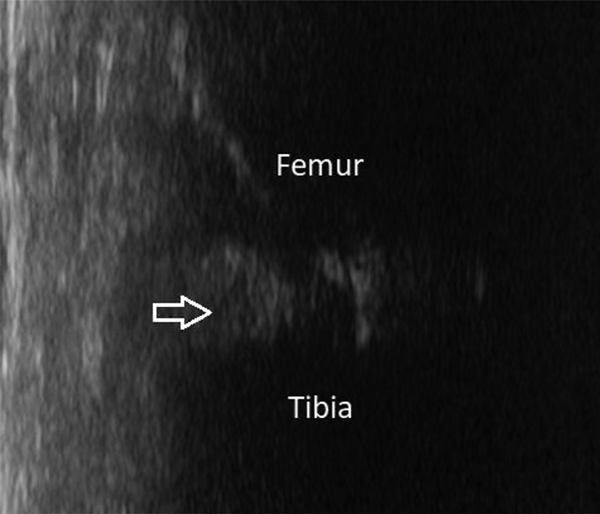
Gray scale indicates hypoechoic area at the medial meniscus considered as degeneration.
Patients were assessed clinically with Lysholm score and radiologically with MRI (1.0 T; Siemens Medical Systems, Iselin, New Jersey, USA) before injection and during the last follow-up.
MRI images were evaluated by two authors as double-blind on sagittal, T2-weighted pictures acquired in 3 mm cuts with 1.5 mm holes. The lesions were classified according to Reicher et al. 1 All patients were allowed full weight bearing, and physical therapy was not prescribed.
Statistical analysis was performed using SPSS version 17 (SPSS Inc., Armonk, New York, USA). Normality of the variable distribution was tested with the Kolmogorov–Smirnov test. Continuous variables were compared using the paired sample t test. Statistical significance was set as p < 0.05.
Results
Eight patients were lost to follow up and 15 knees of 15 patients were evaluated. Nine women and six men with a mean age of 33.2 ± 8.2 (range 19–45) years were included in this study. Mean follow-up time was 31.9 ± 5.6 (range 19–39) months. The data about the patients’ demographics, first–final evaluation of the Lysholm scores, and MRI findings are demonstrated in Table 1.
Patient data, about the Lysholm score 1–2: first–final clinical evaluation, MRI 1–2: first–final radiological evaluation.

MRI: magnetic resonance imaging; L: left; R: right.
All meniscal degenerations were localized in the posterior horn of the medial meniscus. The mean Lysholm score was increased from 71.1 ± 6.9 to 91.9 ± 6.6 after PRP application with statistically significant difference (p < 0.001). MRI grades before and after PRP application revealed significant regression (Figure 3). In 10 patients, grade 2 degenerations turned into grade 1, whereas in only one patient grade 2 degeneration advanced to grade 3. However, in four patients, no radiological change has been observed. There was a statistically significant correlation between decrease in the MRI grades and increase in the Lysholm scores (Table 2).

Transformation of a grade 2 lesion (a) to grade 1 (b) after 30 months after PRP injection. PRP: platelet-rich plasma.
Correlation between decrease in the MRI grades and increase in the Lysholm scores.

MRI: magnetic resonance imaging.
aCorrelation is significant at the 0.05 level (two-tailed).
Discussion
In this study, we conclude that ultrasound-guided PRP injection has positive effect both on the clinical and the radiological outcome in the treatment of IMD. The reason for this positive effect is probably the delivery of tissue-improving factors such as fibroblast growth factor, transforming growth factor-β1, platelet-derived growth factor, and vascular endothelial growth factor with PRP. 18 The positive effect of PRP on meniscus healing has also been shown in different studies. Ishida et al. conducted a preclinical study of the effects of PRP on meniscal tissue regeneration using a gelatin hydrogel. 19 They reported remarkable healing properties of PRP for the repair of the inner avascular part of meniscal injury in vitro and in vivo. In another study, Pujol et al. performed 34 open meniscal repair for grade 2–3 horizontal meniscal tears in a case–control study. 20 In group 1, they performed a standard open meniscal repair. However, in the second group, they injected PRP into the lesion at the end of the procedure, and they observed that PRP injection improved clinical outcomes.
The evidence for treatment options of IMD is rare. A randomized trial published by Biedert et al. reported the best short-term results with partial meniscectomy in patients with symptomatic IMD. 12 On the other hand, we achieved clinical and radiological improvement with a less invasive method. In addition, only 10% of the intra-meniscal lesions can be detected arthroscopically since these lesions do not extend to articular surface. Also the resection of meniscus increases contact stress on cartilage surfaces and accelerates the development of osteoarthritis. 21,22 Besides, partial meniscectomy is not free of complications. Excessive resection, damage to articular cartilage, neurovascular injury, and persistent drainage from portals are some of the possible complications after partial meniscectomies. 23 Therefore, we believe that partial meniscectomy is an excessive treatment for IMD. In another study, Blanke et al. performed percutaneous PRP injection under fluoroscopy in 10 athletes with IMD. 8 They observed significant improvement in clinical scores and the decrease of meniscal lesion grade in MRI at four (40%) patients. They performed the injection in the medial or lateral joint space. We believe that the reason why our radiological results are better is that the use of USG is a more reliable method than fluoroscopy for delivering the PRP to the desired lesion within the meniscus.
The limitations of our study are the absence of a control group, a low number of the patients, and a retrospective design of the study. In addition, imaging a small lesion in the meniscus with ultrasound is difficult and requires experience.
In conclusion, better functional scores and radiological improvement could be obtained after intra-meniscal PRP injection under ultrasound guidance in patients with symptomatic IMD. We believe that it should be considered as a treatment option before surgical intervention. There is a need for prospective randomized studies with larger patients that compares different treatment modalities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.