
Abstract
Introduction
Meniscal injuries are one of the most common knee injuries. The menisci are crucial to well-functioning knees, as they transmit load, stabilize knee joints, secrete lubricants, and provide nutrients to the cartilage. Traumatic lesions predispose an individual to develop osteoarthritis. With the increasing understanding of the biomechanical properties of the meniscus and the advancement of surgical techniques and repair devices, meniscectomy is no longer a routine treatment.
Early literature reports supported restricted rehabilitation until the meniscus was healed. 1 However, more recent studies suggested immediate weight-bearing and early mobilization did not consistently result in loads sufficiently large enough to cause repair failure.2,3 An increasing number of surgeons around the globe reported satisfactory outcomes with an accelerated rehabilitation program.4–6 This study aimed to examine the clinical and functional outcomes for consecutive patients who underwent meniscal repair followed by standardized progressive rehabilitation that allows early mobilization. We hypothesized that early protected weight-bearing with a limited flexion range is a safe option for rehabilitation after meniscal repair procedures.
Methods
This study was carried out in a district general hospital in Hong Kong. Data of patients who underwent meniscal repair from January 2017 to June 2019 were retrospectively analyzed. The starting time was set to 2017, when the standardized meniscal repair rehabilitation protocol was adopted, and 2019 was chosen as the end point, to allow an adequate follow-up period for evaluating patient outcomes. Data were searched from the Clinical Data Analysis and Reporting System of the Hospital Authority of Hong Kong.
The patients were followed up during routine check-ups at 6 weeks, 3 months, 6 months, and 1 year postoperatively. At each follow-up, patient-reported symptoms, the McMurray test, and the International Knee Documentation Committee (IKDC) subjective knee form were used to evaluate the outcomes. The success rate and the time required for patients to resume their sports activities were assessed. When re-tear of the repaired meniscus was suspected based on the patient's symptoms, magnetic resonance imaging (MRI) and knee arthroscopy were performed to assess the repair site.
The difference in the pre- and postoperative IKDC clinical parameters was assessed with the paired Student's t-test using IBM SPSS 22 software with the significance level set at p < 0.05.
The Research Ethics Committee of our institute approved this study, and informed consent was obtained from all study participants.
Inclusion and exclusion criteria
Patients between 15 and 50 years old were included. They had meniscal injury confirmed by clinical examination and MRI scan. They received a course of conservative treatment but failed with persistent symptoms affecting activities of daily living and sports performance. They underwent knee arthroscopy with meniscal repair and received standardized meniscal repair rehabilitation. Patients who had meniscal tears unamenable to repair, who underwent revision surgeries, or those who did not return for clinic follow-up were excluded.
Tear type and location
The meniscal tear characteristics were assessed and documented by a sports specialist during knee arthroscopy. The most frequent type of tear in the lateral meniscus group was a longitudinal tear, observed in 14 of 17 knees (82%), while most bucket handle tears were identified in the medial meniscus (62.5%). Regarding the location of tear, the posterior horn was the most frequent site for both medial (54.5%) and lateral (88.2%) meniscal tears. Of those with medial meniscal tears, four (36.3%) were in the ramp zone, and all had anterior cruciate ligament (ACL)-associated lesions.
Repair procedure
Posterior horn tears were repaired by the all-inside technique using Fast-Fix (Smith & Nephew, London, UK) with a horizontal mattress suture configuration, while anterior horn and middle horn lesions were repaired by the outside-in technique using MENDER II (Smith & Nephew, London, UK) with a horizontal mattress suture configuration.
Meniscal repair rehabilitation protocol
The patients in this study were enrolled in our standardized protocol for meniscal repair rehabilitation. (Figure 1). They were referred to physiotherapists for rehabilitation 8–12 weeks before the operation. Early mobilization and weight-bearing were started immediately after the operation. They were prescribed with a hinged knee brace allowing 0–30 degrees of knee motion for close kinetic chain exercise and partial weight-bearing walking exercise within the first two weeks after the operation. Then, the brace was adjusted to allow 30 degrees more of flexion range every two weeks while maintaining partial weight-bearing until 6 weeks after meniscal repair. Patients were then instructed to take off the brace and wean off the walking aid gradually and started on knee strengthening exercise. At 3 months, they were started on open kinetic chain knee exercise, and agility training specific to their sports was started as early as 5 months after the surgery. Their progress was monitored with close follow-up by the clinicians and physiotherapists with aid of functional score assessment and isokinetic testing. They were advised to return to sports at 9 months if physically fit.
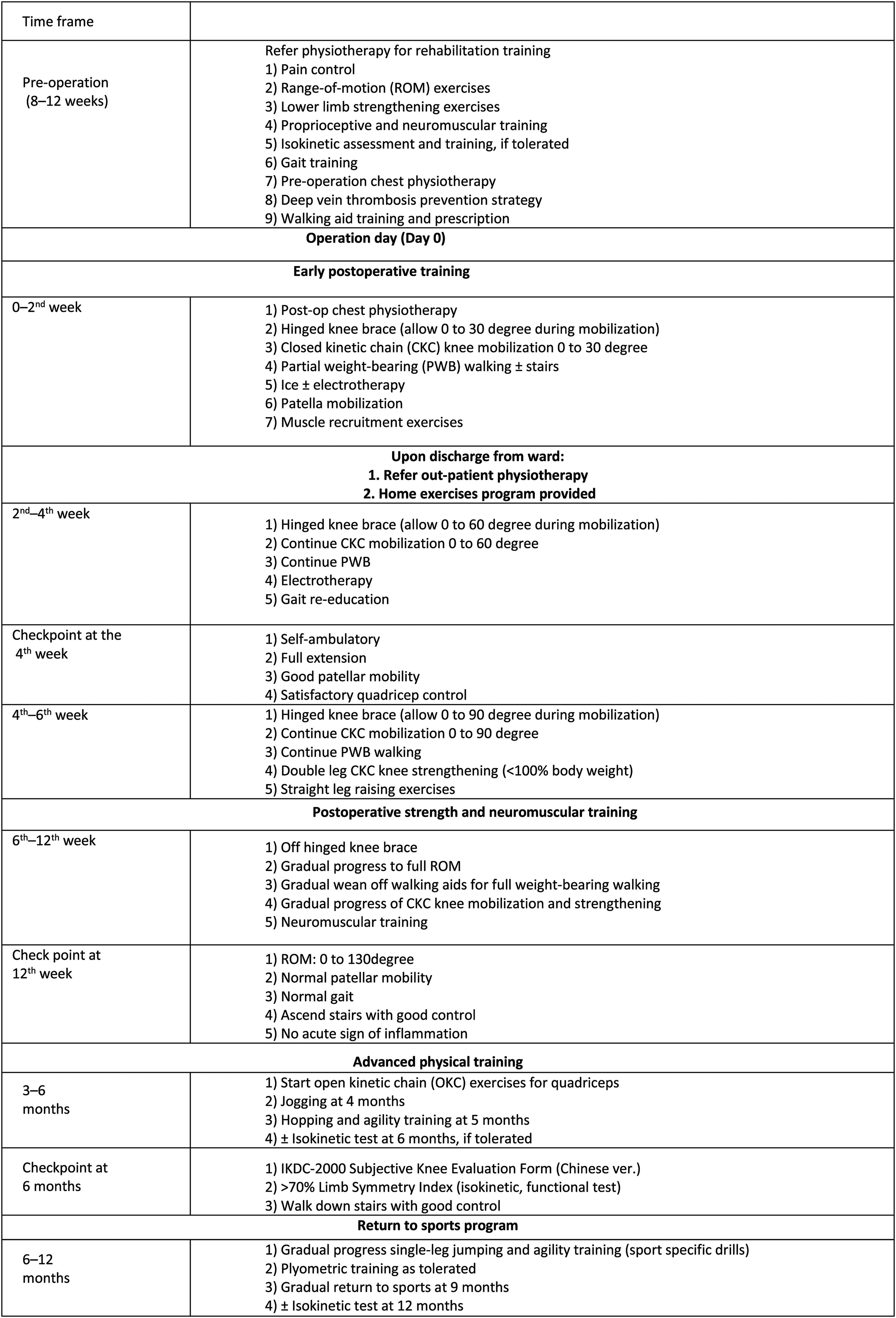
Meniscal repair rehabilitation guideline.
Results
Patient profiles
Altogether, 28 patients (17 knees with lateral meniscal lesions and 11 knees with medial meniscal lesions) who underwent meniscal repair from January 2017 to June 2019 were included in this study. Most patients (22/28, 78%) had a concomitant ACL lesion associated with meniscal injury. All patients who sustained an ACL lesion underwent single-bundle hamstring reconstruction in the same session. The mean age of these patients was 26.6 years (range: 15–47 years), and the mean follow-up period of all patients was 13 ± 3.1 months (range: 9–20 months) (Table 1).
Profile of the study population.
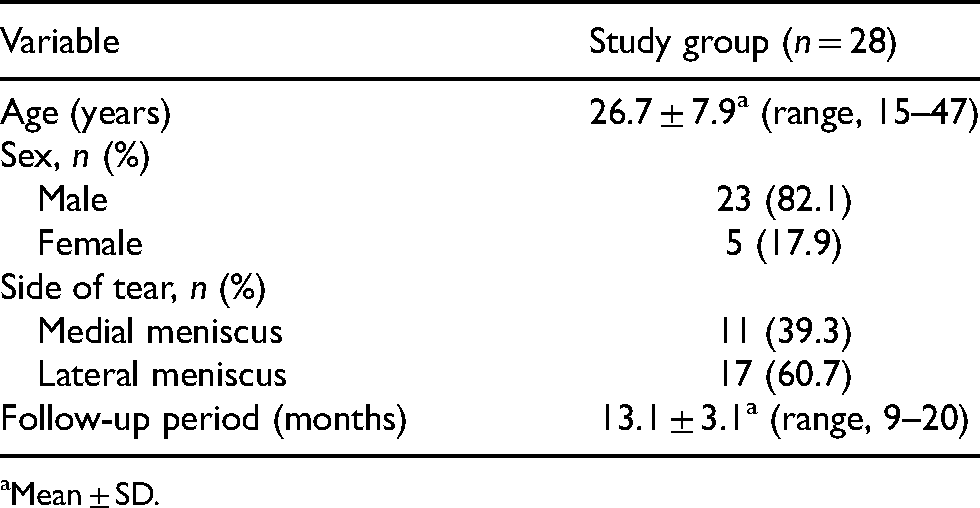
Mean ± SD.
Return to sports and clinical outcomes
Of the patients, 75% (21 of 28) could resume their original sports activities. Seven cases (63.6%) in the medial meniscus group returned to play at an average of 9.2 months, and 14 cases (82.3%) in the lateral meniscus group returned to play at an average of 10.2 months (Table 2). At the final follow-up, the majority of patients displayed satisfactory results, with a mean postoperative IKDC score of 81.4 in the total population (81.4 ± 7.9 in the lateral meniscus group (Figure 2) and 81.5 ± 3.5 in the medial meniscus group (Figure 3)), which was significant compared to preoperative scores.
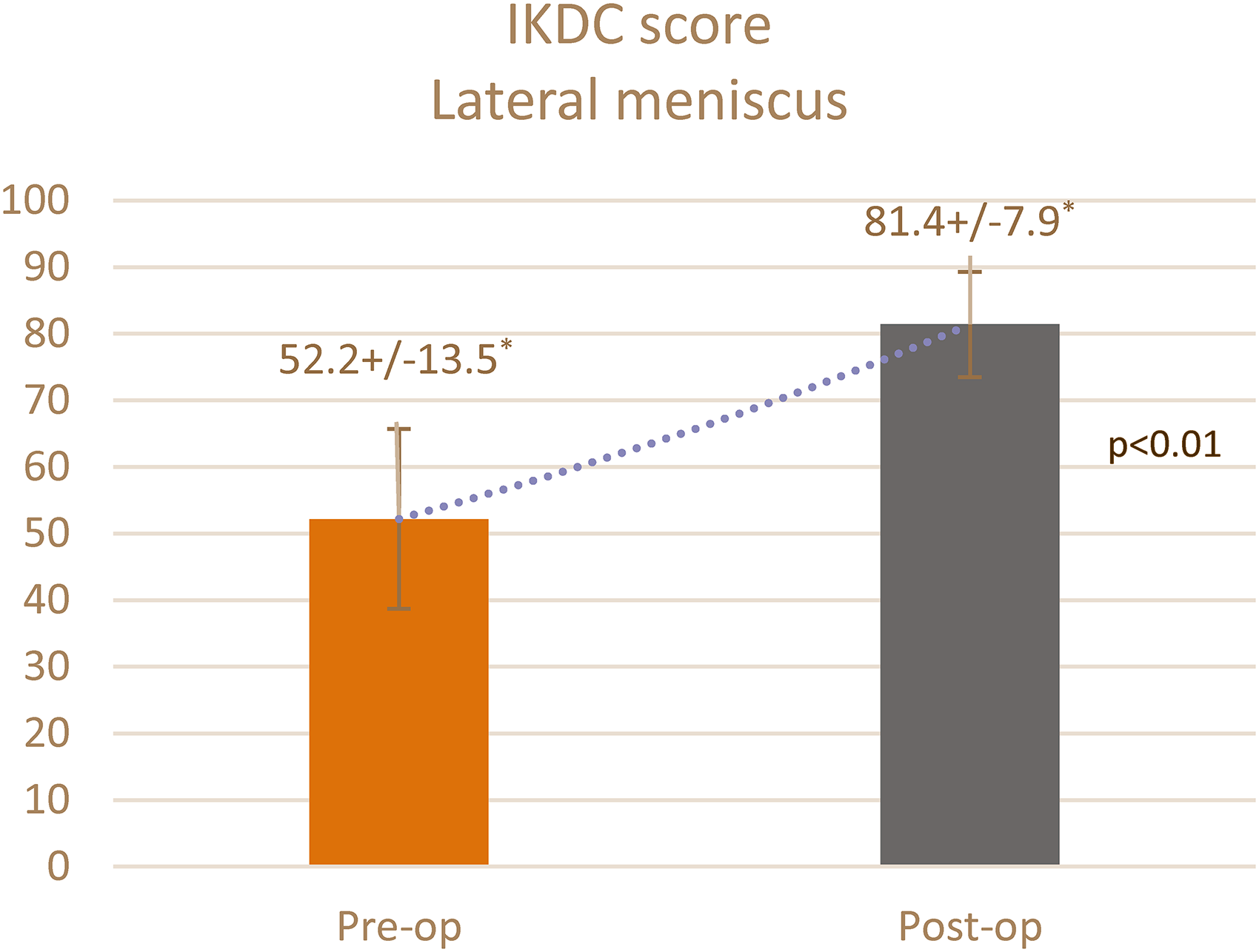
IKDC score lateral meniscus. *Mean ± SD.
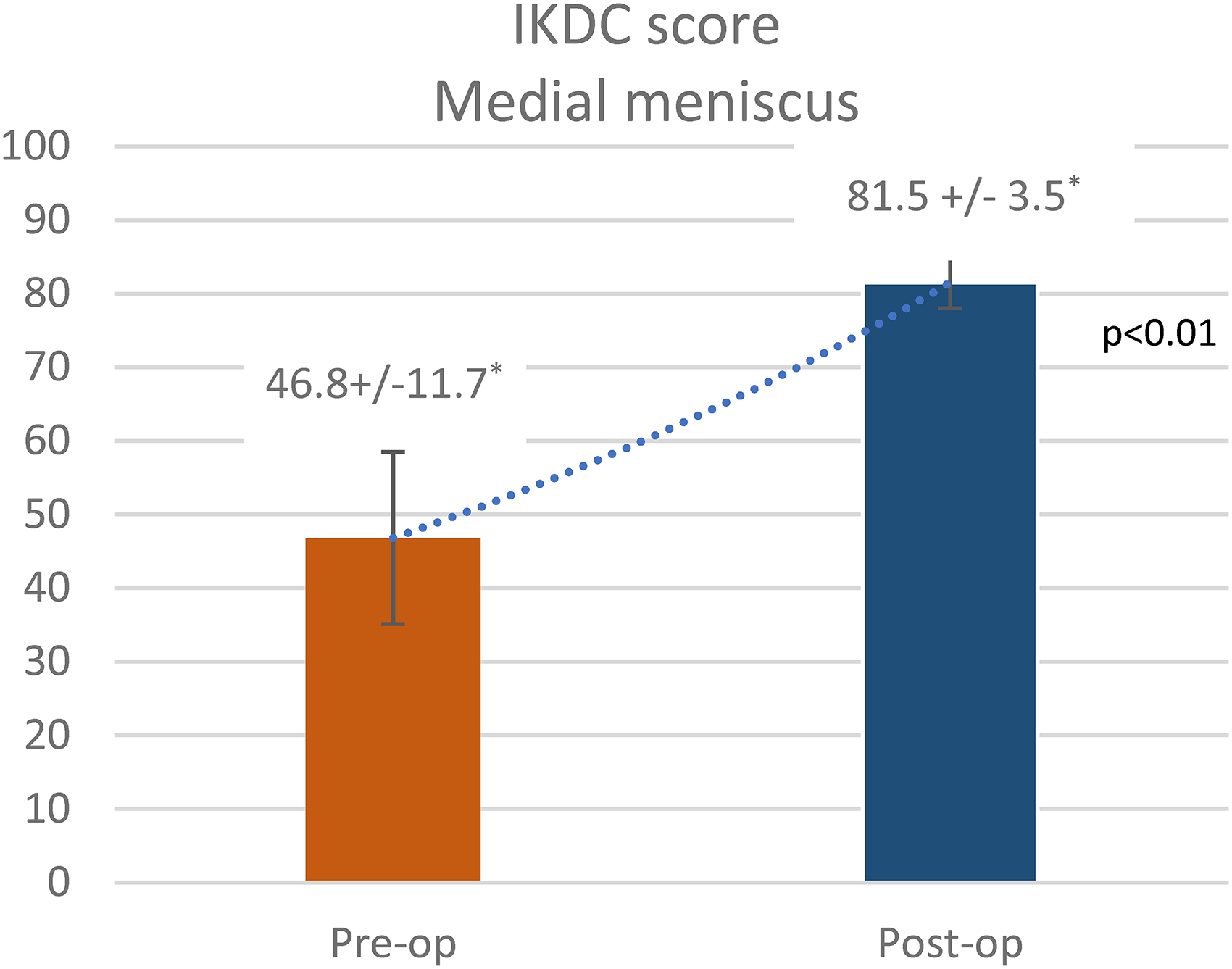
IKDC score medial meniscus. *Mean ± SD.
Return to sports after surgery.
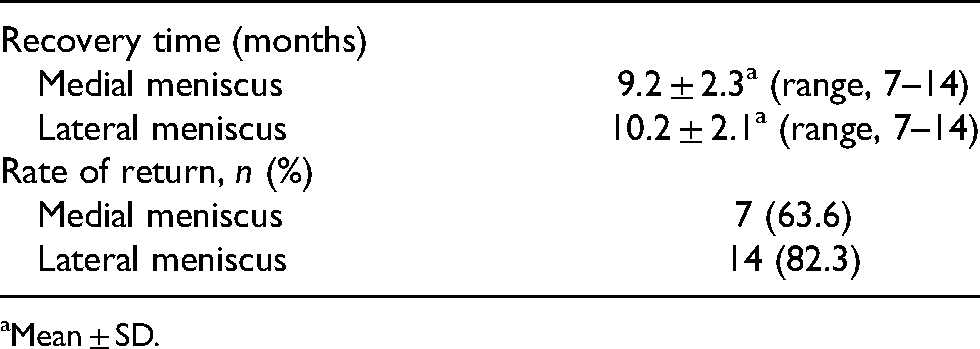
Mean ± SD.
Re-tear of the repaired site
On follow-up, no patient reported locking symptoms, and the McMurray tests performed in patients postoperatively were all negative.
Discussion
This study demonstrated satisfactory outcomes for the participants, as there was a significant improvement in the IKDC scores postoperatively and the majority of participants returned to sports at 9–10 months. No incidence of re-tear was reported after participating in this accelerated rehabilitation protocol.
Meniscal repair has been more prevalent than partial meniscectomy over the past two decades due to advancements in surgical techniques and repair devices. 7 Although meniscal preservation therapy can offer long-term benefits, such as avoiding early degeneration of the knee joint, the recovery period might take longer. However, there is no consensus regarding the optimal postoperative rehabilitation protocol following meniscal repair. 8 Institutions propose their own rehabilitation programs with individual variances in the following aspects: weight-bearing status, range of motion (ROM) of the operated knee, and time to return to pivoting sports. These factors are crucial in a rehabilitation program and should be addressed to facilitate a safe return to sports or work.
Restricted weight-bearing to avoid a high compressive force until the complete healing of the repaired meniscus was supported in early practice. 1 However, some authors held a different belief. Becker et al. investigated changes in the contact pressure of the interface between the meniscus and femur. 2 Cadaveric knees were mounted on a hydraulic materials testing machine, loaded to resemble partial weight-bearing walking, and the meniscofemoral contact pressure was measured while cycling the knees from full extension to 90°. They observed no impact on the repaired meniscus, even when meniscofemoral pressures increased in both compartments with knee flexion. VanderHave et al. described similarly good outcomes for starting weight-bearing immediately after the meniscal repair versus restricting the weight-bearing. 4
Some surgeons prefer postoperative restriction of the ROM of the knee with the intention of limiting the risk of re-tear. Cadaveric studies have revealed that femorotibial contact pressures increase with knee flexion. 9 Morgan et al. and Busenkell et al. put patients in full extension knee splints for 4 weeks after the meniscal repair while allowing full weight-bearing and isometric quadricep and hamstring exercises.10,11 In a weight-bearing MRI study of the knee during deep flexion by Vedi et al., there was subluxation of the lateral meniscus posteriorly due to the roll-back of the lateral femoral condyle. This leads to increased shear stress and subsequent failure of the repair. 12
However, more recent studies have supported early ROM of the operated limb. 13 Sherman et al. concluded that protected early ROM is beneficial for meniscal healing and a protective factor against arthrofibrosis after the operation. 14 In their in vivo studies, Bray et al. described that immobilization delayed the healing process. 15 To avoid the prolonged immobilization and deep flexion of knee that compromises the repair, our protocol advocates controlled and stepwise knee mobilization assisted by a hinged knee brace. Ganley et al. have reported that minimal edge separation occurred in repaired and unrepaired longitudinal posterior meniscal tears when loaded with 45 kg at 60° of flexion. The authors concluded that with limited knee flexion, partial weight-bearing is acceptable after repair. 16 The use of a hinged knee brace, in addition to providing rotational and flexion–extension arc control, protects the healing meniscus. It also provides support to compensate for the initial quadriceps weakness due to postoperative pain or effusion. 14
Hence, more investigators have advocated an accelerated rehabilitation protocol. Lin et al. compared the impact of a “more aggressive” versus a “restricted” rehabilitation regime in a prospective randomized trial. 8 The “more aggressive” regime allows an immediate knee ROM of 0–90° while maintaining touchdown weight-bearing for 2 weeks and weight-bearing as tolerated afterward. The patients were allowed to return to sports as early as 4 months. The “restricted” group was immobilized in extension braces for 6 weeks, and the ROM was gradually increased to 90°. The patients were allowed touchdown weight-bearing for 6 weeks and eventually returned to sports at 6 months. The authors identified no difference in the healing rate and functional outcome scores at 2 years. O'Shea and Shelbourne have also reported favorable outcomes after unrestricted ROM and weight-bearing as early as 3 days after the operation. 17
There have been concerns regarding accelerated rehabilitation in the case of a radial meniscal tear. Radially torn menisci experience more distraction forces and increased strain with axial loading. A more conservative approach for rehabilitation after the repair might reduce the re-tear rate and improve the outcomes. Choi et al. and Haklar et al. adopted a weight and range restriction protocol, respectively, with satisfactory results.18,19 Kocabey et al. reported excellent results using a rehabilitation protocol specific to the tear characteristics. 20 For complex and radial tears, they put patients in braces with weight-bearing as tolerated and flexion ranging from 0° to 125° for 6–8 weeks. For patients with small longitudinal tears, they were allowed to bear weight as tolerated without a brace.
Generally, there is no consensus on the rehabilitation protocol after meniscal surgery. The rehabilitation protocol used in this study was based on various recommendations and had modifications. This protocol allows not only early mobilization by immediate ROM and weight-bearing but also the protection of the repair site by a gradual increase in the flexion range to avoid deep flexion and partial weight-bearing exercise. Advanced physical training, such as quadricep open kinetic chain exercises and agility training, was started at 3–4 months postoperatively.
The IKDC score was used as a subjective tool to evaluate the clinical outcome as it demonstrated acceptable psychometric parameters. Irrgang et al. recorded an intraclass correlation coefficient of 0.94 for the IKDC score. 21 This high level of test–retest reliability implies that repeating the assessment of a patient over time would be consistent, assuming no change in the patient's status.
Most patients (78%) in our study had a concomitant ACL injury, and hence, ACL reconstruction was performed in the same operative session. Accelerated rehabilitation is important following ACL reconstruction to improve the ROM. Although the risk of a failed repair might be a concern if these patients are subjected to a “less restricted” rehabilitation protocol, evidence has revealed that accelerated rehabilitation is safe following ACL reconstruction with meniscal repair. 22 The hemarthrosis associated with ACL reconstruction may provide chemostatic and growth factors to the repaired meniscus. 23 The debris from the femoral and tibial tunnel placement and notchplasty may induce an inflammatory healing response not observed in unreconstructed knees. 22 Moreover, repair of the meniscus in conjunction with reconstruction of the ACL has demonstrated excellent results.24,25 Hence, we did not modify the rehabilitation protocol even if ACL reconstruction was performed in the same session with meniscal repair.
Limitations
This study had some limitations which should be considered in the interpretation of its results. First, the sample size was small, the follow-up period (mean: 8.8 months) was relatively short and this was a retrospective study with no control arm. Most patients who participated in the rehabilitation program had longitudinal type of meniscal tear (82%) and most had concomitant ACL injury (78%). To reduce the confounding factors and to evaluate whether the program could be applied to all meniscal tear types including radial and complex tears or patients with isolated meniscal injury, further prospective clinical study with a larger sample size, longer follow-up period, and control arms with more conservative and more aggressive rehabilitation should be conducted to evaluate and review the efficacy of our rehabilitation protocol for patients with meniscal repair. Secondly, the results of a successful repair were based on the clinical evaluation of patients’ signs and symptoms. A second-look arthroscopy would be indicated only if the patients reported knee pain and locking or if there is a positive McMurray result. Performing routine follow-up arthroscopy would raise ethical issues and pose increased costs to the healthcare system, so it is not feasible. Asymptomatic patients with a failed repair might be overlooked for this reason. MRI would be a useful tool to assess possible repair failure. However, in a study by Nicolas Pujoi et al., MRI was not suitable in sensing meniscal healing, even up to a 10-year follow-up. 26 The actual failure rate might be higher than that being reported. Thirdly, the postoperative clinical follow-up was conducted by one of the surgeons performing the operation. This might induce bias in the clinical assessment, although objective clinical outcome tools (e.g. IKDC scores) were used.
Conclusion
This study demonstrated satisfactory outcomes and an early return to sports in patients participating in the rehabilitation protocol that allows early mobilization and protected weight-bearing without jeopardizing the repair site. Further investigation should be conducted with a larger study population and a longer follow-up period.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Research Ethics Committee of Kowloon Central/Kowloon East approved this study [Reference number: KC/KE-21-0277/ER-4].
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.