
Abstract
Objective:
The purpose of this study is to analyze the radiological and functional outcome of complex proximal humerus fractures treated by open reduction and plate fixation, and how radiological parameters correlate with functional outcome.
Design:
Retrospective study.
Setting:
Level-1 trauma center.
Patients/methods:
One hundred twenty-seven patients were analyzed, with a mean follow-up of 5 (3–7) years.
Outcome measurements:
Radiological parameters studied were neck-shaft angle (NSA), greater tuberosity (GT) to articular surface (AS) distance, medial hinge reduction, and presence (or absence) of calcar screw. Functional outcome evaluated by DASH and Constant–Murley (C-M) score.
Results:
The mean age is 53.8 years. All patients had a union in 14 (12–18) weeks. The mean NSA is 135° (112–155°). One hundred and thirteen patients with an NSA of >120° had a good functional outcome. Fourteen patients with NSA ≤120° had shoulder abduction <90°. The mean GT to AS distance is 7.2 mm (−2 to 16). The superior displacement of GT above AS is associated with abduction of <90° (16 patients). The mean medial gap is 3 mm (0–17). In 14 patients with a medial gap of >4 mm and without calcar screw, varus collapse is observed. All patients had a good outcome on DASH score and 122 patients had good to excellent outcome on C-M score. Five patients with poor outcome on C-M score had NSA <120° and displacement of GT above AS.
Conclusion:
Radiographic indicators for poor outcome are varus angulation with NSA <120°, superior displacement of GT above AS, the presence of medial gap >4 mm, and absence of calcar specific screw. This “terrible triad” of proximal humerus fracture should be avoided during operative fixation.
Introduction
Proximal humerus fractures are relatively common, accounting for 4–5% of all fractures 1 and are the third most common type in people aged more than 75 years. 2 Their incidence increases with age and women are affected up to twice as often as men. 1,3 Most proximal humerus fractures are minimally displaced with stable fracture pattern, which can be treated conservatively with good outcome. 4,5 As per Neer et al.’s criteria, 6 only 20% of fractures are unstable, which requires surgical fixation. 7
Open reduction and internal fixation of three- and four-part proximal humerus fractures have increased in frequency with the development of locking plates, especially in comminuted and osteoporotic fractures. Despite its success, studies have shown high complication rates ranging from 16% to 36%, 8 which include articular screw penetration, subacromial impingement, varus malalignment, nonunion, implant failure, and osteonecrosis of the humeral head which adversely affects the final outcome. Further, most of these complications were attributed to poor surgical technique, improper implant positioning, and failure of accurate intraoperative assessment of reduction and screw length. 9 A recent systematic review had shown that while locking plates are suitable devices for complex proximal humeral fractures, they can be associated with complications like screw penetration into joint, avascular necrosis, and subacromial impingement. 10 Despite high complication rate, the functional and patient-oriented results of the locking plate fixation are satisfactory and good surgical technique is mandatory for further improving functional outcome. 11
Current literature contains conflicting evidence about the functional and radiologic results of three- and four-part proximal humerus fractures. Court-Brown and McQueen reported no association between the varus angulation and the shoulder function 12 especially in elderly patients. Blonna et al. and Südkamp et al. proposed that varus angulation of more than 25–30° results in poor functional outcomes. 13,14
The purpose of this study is to analyze the accuracy of fracture reduction in three- and four-part proximal humerus fractures using radiological parameters and to correlate them with functional outcome.
Materials and methods
A total of 127 (of 216) patients with displaced three- (66 patients with surgical neck and greater tuberosity (GT) fractures) and four-part (61 patients) proximal humerus fractures treated with open reduction and plate fixation from January 2008 to December 2010 were analyzed retrospectively. This study is approved by an institutional review board. All cases are operated upon by a single surgeon (DD). Using Neer et al.’s classification, a fracture is considered displaced if there is angulation of more than 45° or separation of more than 1 cm between fragments. According to the Orthopaedic Trauma Association Classification, all 11-B and 11-C fractures were included in the study. 15 Patients with incomplete follow-up, open fractures, two-part fractures, neglected fractures, pathological fractures, and presence of ipsilateral fractures other than proximal humerus were excluded from the study. Proximal humeral locking plate (Synthes®, Paoli, Pennsylvania, USA) is used in all patients.
Surgical technique: Open reduction and fixation
The fracture is exposed using an anterior deltopectoral approach with a patient positioned in supine on radiolucent table. The tuberosities were identified and tagged using suture or wire and reduced below the level of the articular surface (AS). Beyond the deltopectoral interval, at the fracture site, entire reduction is done using joysticks. Here the key step is maintaining the soft tissue envelop around the head intact and thus maintaining the biology. The spherical head lying medially and inferiorly held with a T-shaped threaded pin as a joystick and levered out into the glenoid cavity. Any varus reduction should be avoided. This can be checked under fluoroscopic image by restoring the following parameters, that is, the inferior margin of glenoid should correspond to the inferior margin of the humeral head AS (restoring Gothic arch); the lateral margin of the acromion should correspond to the humeral head-tuberosity interval and restoring the calcar continuity. The reduced head is temporarily fixed to the shaft with k-wires from anterior to posterior, inserted away from the position of the plate. In patients with fracture dislocation, head is reduced before tuberosity reduction, as shown in Figure 1. The plate is positioned on the lateral surface and below GT and fixed with a minimum of five locking screws into head as recommended by the manufacturer and implant guide, preferably in a divergent fashion. Lateralization of the shaft should be avoided during shaft screws application. Additional tension band sutures passed through the cuff insertion and securing them to small holes in plate neutralizes the pulling forces on the tuberosity fragments. Final reduction is checked under the image intensifier.
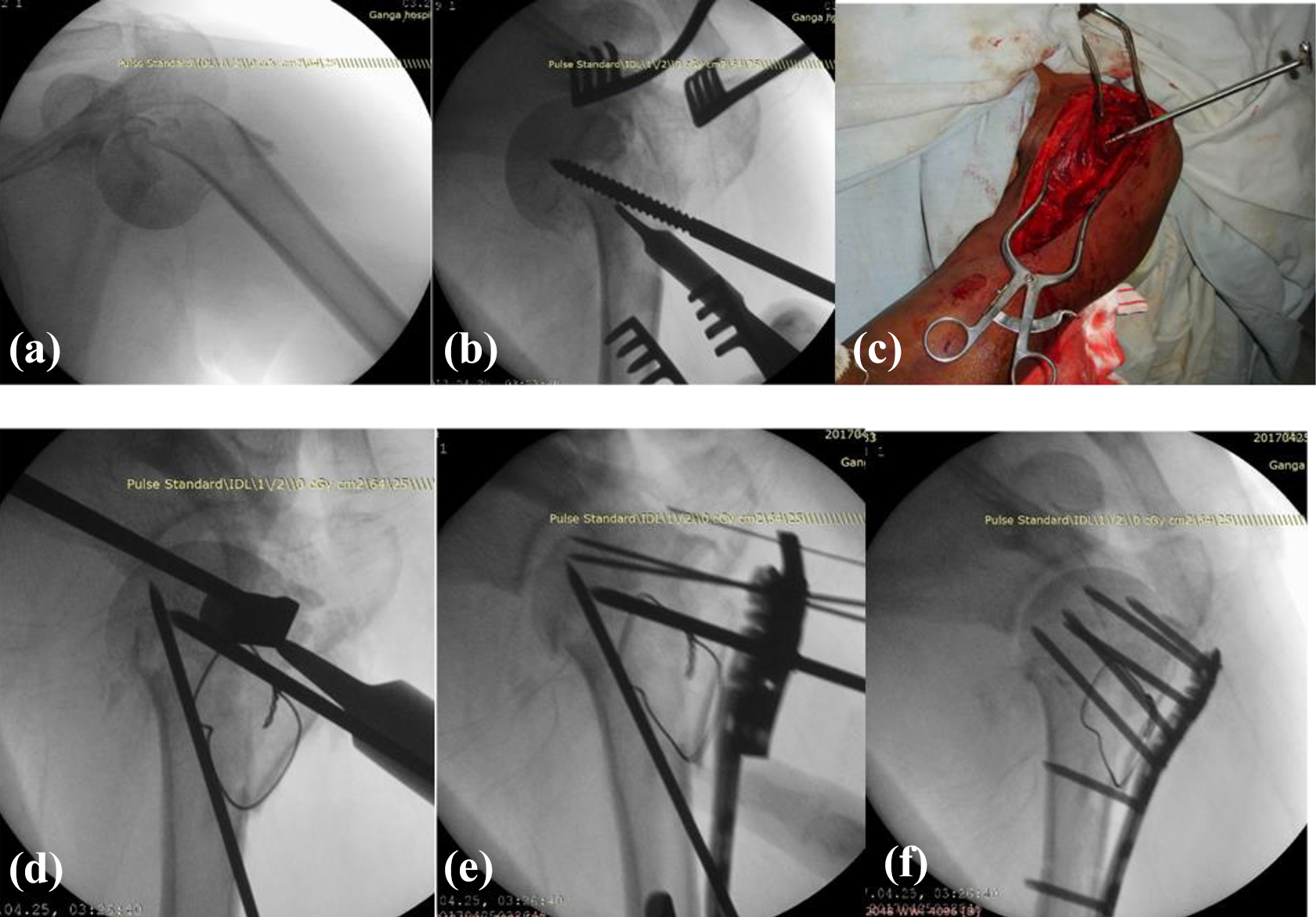
Open reduction and fixation of proximal humerus fracture dislocation. (a) Four-part humerus fracture with axillary extrusion. (b) and (c) Threaded pin with T-attachment inserted into the head through the fracture plane and levered into the glenoid cavity without disturbing the vascularity of the head. (d) Reduction stabilized with k-wires. Tuberosity fragments secured with SS wire. (e) Plate positioned and proximal extent of plate checked by inserting k-wire through the proximal hole, which should rest on the AS. (f) Final fixation with a restoration of NSA, well reduced calcar, and GT below the AS. SS: stainless steel; AS: articular surface; NSA: neck-shaft angle; GT: greater tuberosity.
A standard supervised rehabilitation program is followed. Gentle active pendulum exercises were started on the first postoperative day with the patient leaning forward by 90°. Passive movement of the shoulder was started on the 14th day after the operation, which allowed flexion of up to 90°, external rotation, and abduction as tolerated to the pain limits. Patients were advised to use a sling for 4 weeks. At the end of the fourth week, assisted and free active movements are started in all planes. Strengthening is started at the end of 12 weeks.
Evaluation
Standardized postoperative X-rays including anteroposterior view and axillary view (taken at immediate postoperatively; 1, 3, 6, and 12 months; and at final follow-up) were evaluated for quality of reduction using the neck-shaft angle (NSA), reconstruction of the medial hinge, GT to AS distance, and presence (or absence) of calcar specific screw (Figure 2). Follow-up X-rays were also evaluated for bone healing, avascular necrosis, implant-related issues, penetration of screws into joint, and arthritic changes. All patients were regularly followed for a mean period of 5 years (3–7). Functional outcome is evaluated by the DASH score and Constant–Murley (C-M) score at the final follow-up.

Radiographic parameters. 1. NSA. 2. Medial hinge reduction. 3. (a) GT to AS distance, and arrowhead showing the position of calcar screw. AS: articular surface; NSA: neck-shaft angle; GT: greater tuberosity.
Results
A total of 127 patients were studied (Table 1). The mean age of the patients is 53.8 years (24–78 years) with 97 males and 30 females. The right side involved in 74 and left side in 53 patients. The mode of injury is a road traffic accident in 96 patients and fall in 31 patients. Table 2 shows the distribution of the fracture pattern in the study population.
Demographic details of a study group.

Showing the fracture pattern in study population.

The mean head-shaft angle is 135°, ranging from 112° to 155°. Considering the normal NSA of 135°, acceptable varus deviation up to 120° is described in the literature. 16 In this study, 14 patients had an NSA of ≤120°; in all these patients, shoulder abduction is less than 90°. In three patients with an NSA of >130° and well-reduced GT below AS, the shoulder abduction at the final follow-up is <90° with only fair functional outcome (Figure 3), probably due to associated rotator cuff and soft tissue injury.

Valgus impacted fracture with anatomical reconstruction has poor functional outcome probably due to associated rotator cuff and soft tissue injury.
The distance between the upper limit of the GT and of the AS is evaluated, considering that this area is vital for the abduction of the shoulder and has significance in functional outcome. In this study, mean distance of GT to AS is 7.2 mm (−2 to 16 mm). The superior displacement of GT above the AS is associated with abduction of <90° in all patients (16 patients).
The medial gap is measured as a distance between the inferior articular margin and the proximal medial metaphysis as a result of comminution or inadequate reduction. The mean medial gap measured on the postoperative X-ray is 3 mm (range from no gap to 17 mm). Postoperative varus collapse (loss of NSA of more than 15°) seen in 14 patients. In all these 14 patients, the medial gap is more than 4 mm and the calcar screw is not applied. In patients with a medial gap of less than 4 mm or a medial gap of more than 4 mm with calcar screw, no loss of NSA is noticed.
The range of motion is also calculated at the final follow-up. Seventy patients (55%) had abduction above 90° degrees (Figure 4). Fifty-seven patients (45%) had abduction below 90°. The DASH score is good in all these 57 patients and the C-M score is less than 60 in 5 of these patients (in these patients, the head is in varus and GT to AS distance is less than 8 mm).

Proximal humerus fracture with GT displacement and humeral head in varus in an osteoporotic lady with good functional outcome after fixation with a locking plate. GT: greater tuberosity.
DASH score of less than 40 is considered a good outcome and the C-M score of more than 60 is considered as good outcome. 17,18 All patients had a good outcome based on the DASH score (100%) and 122 patients (96%) had good to excellent outcomes based on the C-M score. The average DASH score is 13 and the C-M score is 82.
Abduction is >90° in patients who had GT below the AS and no varus of the humeral head (p < 0.05). Abduction is limited to <90° in patients with GT above the AS and with varus positioning of the humeral head. Varus collapse/malreduction and superior displacement of GT above the AS has a statistically significant relationship with poor functional outcome. Varus collapse seen in 14 patients; in all these patients, there is a medial gap >4 mm in the immediate postoperative X-ray and the calcar screw is not applied.
Asymptomatic avascular necrosis was seen in two patients with screw penetration into the joint. Both these cases preoperatively showed complete disruption of a medial hinge. All fractures healed in 14 (12–18) weeks. No evidence of infection, screw pull out, and plate breakage were noticed. Tension band wire applied to secure the GT was broken in three cases and is asymptomatic. Results are summarized in Table 3.
Results of a study group.

AS: articular surface; NSA: neck-shaft angle; GT: greater tuberosity; C-M: Constant–Murley.
Discussion
Proximal humeral fractures are common fractures with complex fracture pathoanatomy, and methods of treatment adopted to ensure early functional recovery are of great interest in current orthopedic practice. 3 The technique of reduction and fixation and the experience and skill of the surgeon play an important role. The method described as open reduction and plate fixation seems to be a good technique and achieves anatomical reduction with minimal soft tissue dissection.
In this series, 96 of 127 patients were younger than 60 years, with a mean age of 53.8 years. In addition, 97 of the 127 patients were men, who may be expected to have better overall bone quality. Most other series have reported a much greater proportion of female patients. 19
The NSA represents the angle between the diaphysial axis and the humeral neck axis, drawn as perpendicular to the base of the head. 20,21 The normal value of NSA is approximately 135°. An NSA of 120° or less is a predictor of secondary varus collapse, especially when the medial hinge is not reduced; therefore, it is considered that varus deformities more than 20° were not acceptable especially after surgery. 22,23 In this series, of 127 patients, 14 had an NSA of ≤120°; in all these patients, shoulder abduction is less than 90° and C-M score is ≤60, indicating that failure to reproduce the normal NSA impairs the functional outcome. These results are comparable to the literature, which describes limitations of shoulder mobility, especially of the abduction, due to varus deformation of the humeral head. 24 The loss of reduction and secondary screw perforation in the treatment of proximal humerus fractures with locking plates has already been described. The rigidity of fixed-angle locking device is responsible for screws cutting through osteoporotic bone, leading to humeral head subsidence because of a deficient posteromedial bone buttress or osteonecrosis. Brunner et al. 25 and Badman et al. 26 shown that secondary varus angulation can be prevented by neutralizing traction forces from the rotator cuff using tension band sutures combined with screws supporting the medial calcar, especially when medial support is insufficient. In the current study, all the patients with greater and lesser tuberosity fractures fixation are augmented by either stainless steel wire or nonabsorbable sutures (Ethibond, Ethicon LLC, San Lorenzo, USA).
Restoration of the medial hinge is critical for successful anatomic healing of the proximal humeral fracture. Metaphyseal comminution and lack of medial calcar support for the head may lead to early loss of the reduction, particularly in cases with primary varus displacement. Recent studies have emphasized the importance of stabilizing the medial column for maintaining stable fixation of proximal humerus fractures and to prevent varus malunion, plate failure, screw cutout, and impingement. 27 Anatomic reduction and restoration of the medial calcar allow the medial column to both buttress and reduce the stresses of laterally based plate fixation. Biomechanical studies have shown that medial support increases load to failure, axial stiffness, and shear stiffness, as well as torsional stiffness of proximal humerus fixation constructs. 28 Gardner et al. 27 first emphasized this concept by noting that when mechanical support of the inferomedial region of the proximal humerus is obtained, fracture subsidence is significantly reduced postoperatively. Mechanical support of the medial column may be achieved either with the placement of calcar screws or endosteal fibular allograft strut augmentation when anatomic cortical contact is not possible. 29,30 They reported that lack of medial support led to a 30% screw perforation rate compared to a 6% screw perforation rate for fractures with an intact medial column. Owsley and Gorczyca 31 demonstrated that the incidence of varus deformity is 25% and that screw cutout occurred in 23% of the cases with medial comminution and lack of medial support following fixation. In osteoporotic fractures, slight varus impaction to get medial support is also recommended. 24
In this series, the average medial gap measured on the postoperative X-ray is 3 mm (0–17 mm). Postoperative varus collapse (loss of NSA of more than 15°) seen in 14 patients. In all these 14 patients, the medial gap is more than 4 mm and the calcar screw is not applied. In patients with a medial gap of less than 4 mm (79 patients) or medial gap of more than 4 mm with calcar screw (34 patients), no loss of NSA is noticed. In cases with an intact medial cortex, the medial hinge should be reduced but in cases with medial comminution, calcar-specific screws should be used to augment the medial column. Because of the fixed-angle relationship between the plate and the screws, locked-plate fixation provides a mechanical advantage in fractures with metaphyseal comminution, particularly when there is insufficient cortical contact opposite to the plate. 32
The subacromial space is normally 7–11 mm wide and the GT is positioned so that its upper level is 8–10 mm lower related to the AS. 33 Practically, the intact subacromial space allows full abduction, while it’s narrowing results in a painful limitation of this movement, due to the presence of the rotator cuff. External rotation is also affected by an abnormality in the subacromial space. Thus, restoration of these anatomical landmarks is important to attain a good functional outcome. Impingement secondary to decreased subacromial space due to proximal malpositioning of the plate or inadequate reduction of tuberosity fragments is a frequently observed complication. Schliemann et al. 11 have shown that impingement is both the most frequent complication and the most frequent reason for surgical revision in their series. The plate should be positioned 10–15 mm distal to the GT to limit the risk of impingement. 34 If possible, the shoulder should be gently abducted to confirm that the proximal aspect of the plate does not impinge on the acromion. The proximal humerus locking plate provides an aiming device with a proximal hole, which allows controlling the correct position of the plate using a k-wire. The k-wire passed through this hole should rest on the top of the AS of the humeral head.
The functional outcome is excellent in this method of treatment by open reduction and plate fixation. In this study, all patients had good outcome based on the DASH score (100%) and 122 patients (94%) had good to excellent outcome based on the C-M score. However, it should be noted that 57 patients (45%) had abduction only up to 90°, although they showed little increase in forward elevation and when correlated to functional outcome, all of them showed good results. This signifies that apart from fracture we need to look for the associated cuff and soft tissue integrity in these patients which is a common problem in these fractures. 35 –37
Avascular necrosis is the most feared complication of internal fixation of proximal humerus fractures, which can result from the fracture pattern itself or soft tissue dissection used in operative treatment. Contrary to the common belief, results in this series showed good outcomes even in split heads and fracture-dislocation patterns. Only two patients (1.57%) had avascular necrosis and are asymptomatic but have the restriction of movements. And hence fixation must be the choice in these types of fractures also. The rate of avascular necrosis is less in this series as compared to reported rates of 4–16%. 38 –41 This may be due to minimal soft tissue dissection beyond the deltopectoral interval. The results in our study do not show any problem with fixation failure. Screw penetration is seen only in two patients with avascular necrosis. The limitation of this study is its retrospective nature.
Intraoperative checklist for good radiographic reduction is to get predictable functional outcomes (Table 4). Varus reduction, superior displacement of GT above the AS, and lateralization of a shaft with loss of calcar continuity are considered as “Terrible Triad” of proximal humerus fracture fixation, with consistently poor results.
Intraoperative checklist for good radiographic reduction to get predictable functional outcome.

NSA: neck-shaft angle; GT: greater tuberosity.
Conclusion
Radiographic indicators for poor functional outcome in proximal humerus fractures are postoperative varus angulation with NSA less than 120°, superior displacement of GT above an AS, the presence of medial comminution with a medial gap of more than 4 mm, and the absence of calcar specific screw. This “terrible triad” of proximal humerus fracture should be avoided during operative fixation. Using the intraoperative checklist for fracture reduction along with minimal soft tissue dissection and joystick reduction techniques gives a good radiological and functional outcome in these complex proximal humerus fractures.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.