
Abstract
Background:
Both cruciate retaining (CR) and posterior stabilized (PS) implants are commonly used for primary total knee arthroplasty. There is evidence to support improved range of motion in PS knee replacements, but there is no evidence showing functional superiority. The aim of this study was to compare functional outcomes between CR and PS knee replacements.
Patient and methods:
Prospectively collected regional joint registry data were used to compare preoperative and postoperative one, 5- and 10-year Oxford and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores in 1287 primary total knee replacements. Differences in functional scores between CR and PS knees were calculated.
Results:
The PS group had better functional scores than the CR group at baseline (mean Oxford score 15.59 vs. 14.52 (p = 0.026) and mean WOMAC score 59.51 vs. 62.35 (p = 0.012)), at 1 year postoperatively (mean Oxford score 37.94 vs. 36.63 (p = 0.015) and mean WOMAC score 16.20 vs. 19.73 (p = 0.001)) with a similar trend at 5 years postoperatively (mean Oxford score 39.66 vs. 38.50 (p = 0.054) and mean WOMAC score 16.89 vs. 18.83 (p = 0.131)). There was no difference in the overall functional improvement between the PS and CR groups at 1, 5, or 10 years. WOMAC subcomponent scores showed greater improvement in stiffness; 3.76 versus 3.36 (p = 0.012) in PS knees at 1 year postoperatively. No significant differences were observed at 5 or 10 years.
Conclusions:
PS knee replacements showed greater improvement in stiffness at 1 year postoperatively. There was no difference observed at 5 or 10 years postoperatively. PS knees had better functional outcomes at 1 year with a similar trend at 5 years postoperatively.
Level of evidence:
III.
Keywords
Introduction
Total knee joint replacement is the definitive treatment for end-stage knee arthritis for patients who have exhausted all nonoperative measures. Total knee arthroplasty surgery has been shown to be highly successful in improving functional outcomes. 1
Proponents of cruciate retaining implants argue that preservation of the posterior cruciate ligament (PCL) provides improved proprioception, superior knee stability, and replicates normal knee kinematics. On the other hand, proponents of PCL sacrificing implants argue that a more controlled replication of the femoral rollback mechanism can be created resulting in reduced sliding sheer stress on the polyethylene liner and providing superior range of motion in terminal knee flexion. 2,3
Multiple studies have addressed differences in knee range of motion following cruciate retaining and posterior stabilized primary knee replacements. Most studies have shown a small gain in terminal flexion with posterior stabilized designs. 4 –9 A number of studies have also reported on short- and medium-term functional results comparing these two implant designs. 4 –7,10 –13 The current literature has not demonstrated any significant difference in early functional outcome between posterior stabilized and cruciate retaining knee replacements. This discrepancy between biomechanical and clinical results suggests that the differences in function between PS and CR knees are either nonexistent or that they are not detected with current outcome tools.
The primary objective of this study was to compare function in patients who underwent primary total knee arthroplasty surgery using posterior stabilized and cruciate retaining implants. We hypothesized that increased range of motion in PS implants would correlate with superior patient perceived range of motion and physical function.
Method
After obtaining Ethical Review Board approval, data covering the period from January 1, 2005 to December 31, 2009 were collected from our regional joint registry records. The registry was established in 2004 by a group of orthopedic surgeons who serve a population of approximately 250,000 people. Our regional joint registry is distinct from, but complementary to the New Zealand National Joint Registry, prospectively recording preoperative functional scores, baseline demographics, operative characteristics, and postoperative outcome measures for all patients undergoing arthroplasty surgery throughout the region. The registry assesses preoperative and postoperative patient function using self-administered disease specific (Oxford and WOMAC) and general health (SF-12 PH and SF-12 MH) questionnaires completed by patients at their preoperative clinic appointment as well as at 1, 5, and 10 years postoperatively.
Registry records of all patients who underwent primary total knee arthroplasty surgery during this period were reviewed.
Baseline demographics (age at time of surgery, gender, American society of anesthesiologists (ASA) score, operative side, preoperative diagnosis) were recorded, and all patients were classified as either having had a posterior stabilized or having cruciate retaining prosthesis implanted.
The two groups were then compared using disease specific functional scores, Oxford and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), both preoperatively and at 1, 5, and 10 years postoperatively. Absolute scores as well as change in scores from preoperative to 1, 5, and 10 years postoperative were compared.
Statistical analyses
Data were tabulated using a spreadsheet. Standard descriptive statistics including means and standard errors were used to summarize the continuous measures and frequencies and percentages for the categorical measures for posterior stabilized and cruciate retaining groups. Continuous measures at each time point were compared between posterior stabilized and cruciate retaining groups using analysis of variance (ANOVA) and changes from baseline compared using analysis of covariance with the baseline level as the covariate. Preoperative ASA scores were compared using a Mann–Whitney U test. Multivariate analysis was then used to adjust for baseline differences between groups, and a two-tailed ANOVA analysis was performed on the adjusted data. A two-tailed p-value of <0.05 was taken to indicate statistical significance.
Results
From our regional joint registry records covering the 10-year study period, we identified 493 patients who underwent primary total knee arthroplasty using posterior stabilized implants and 794 using cruciate retaining implants with a minimum of 1 year follow-up. Not all measures were available for all patients at each time point, and mean levels and sample sizes for each measure at each time point are presented in Table 1.
Comparison of baseline patient demographics, Oxford and WOMAC scores between posterior stabilized and cruciate retaining total knee arthroplasties preoperatively and at 1, 5, and 10 years postoperatively.a
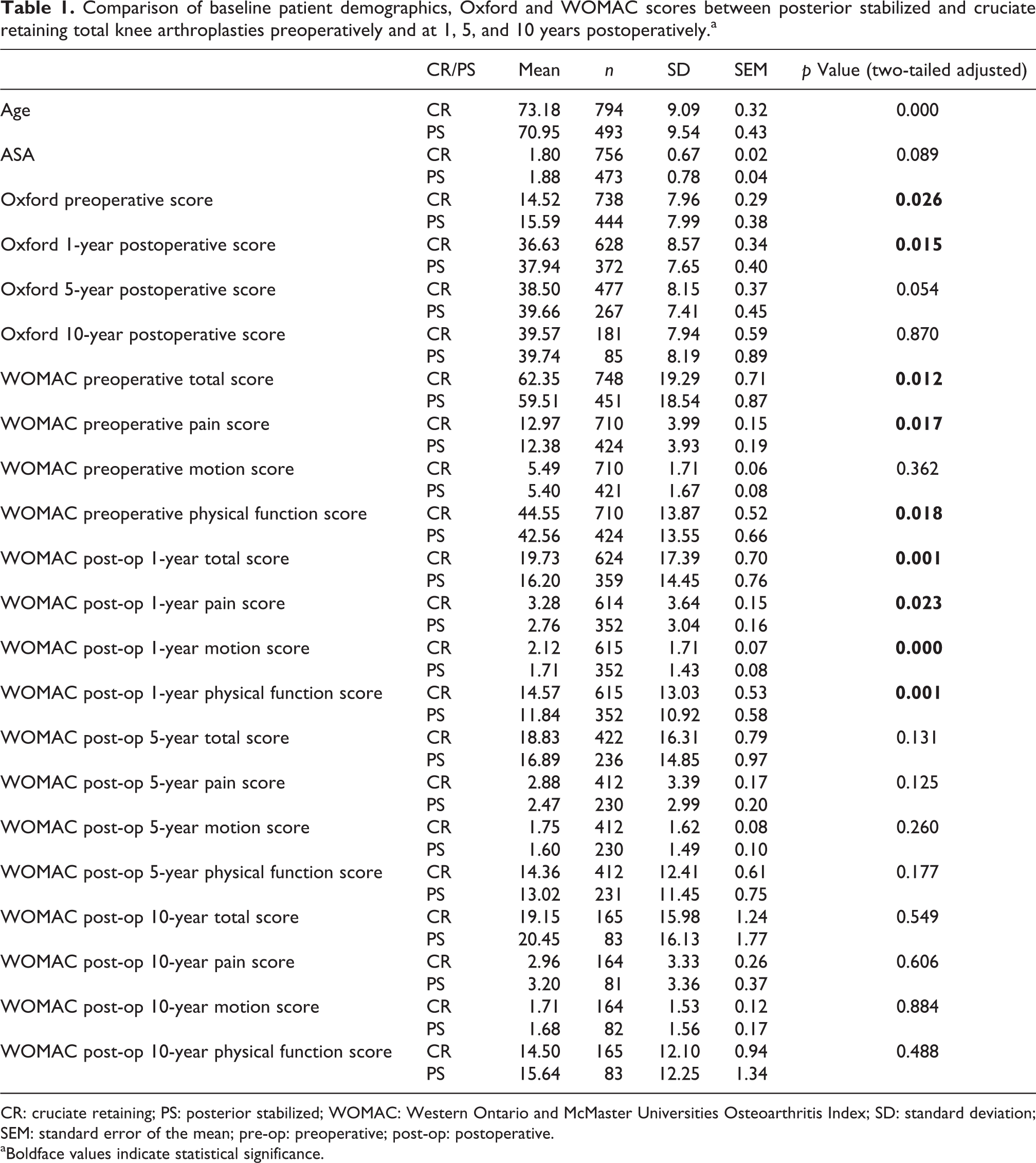
CR: cruciate retaining; PS: posterior stabilized; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; SD: standard deviation; SEM: standard error of the mean; pre-op: preoperative; post-op: postoperative.
aBoldface values indicate statistical significance.
Baseline demographics
At the time of surgery, patients in the posterior stabilized group were significantly younger than the cruciate retaining patients, mean 70.95 years versus 73.18 years (p < 0.001). There was no significant difference in their ASA scores, mean 1.88 versus 1.80 (p = 0.089).
Primary outcome
The posterior stabilized group had better preoperative function than the cruciate retaining group; mean Oxford score 15.59 versus 14.52 (p = 0.026), mean WOMAC score 59.51 versus 62.35 (p = 0.012). The posterior stabilized group had better functional outcomes at 1 year, mean Oxford score 37.94 versus 36.63 (p = 0.015), mean WOMAC score 16.20 versus 19.73 (p = 0.001), with a similar trend at 5 years postoperatively, mean Oxford score 39.66 versus 38.50 (p = 0.054), mean WOMAC score 16.89 versus 18.83 (p = 0.131). At 10 years, this trend was no longer evident, mean Oxford score 39.74 versus 39.57 (p = 0.870), mean WOMAC score 20.45 versus 19.15 (p = 0.549). After adjustment for baseline differences between groups, there was no difference in the overall functional improvement preoperatively to 1 year postoperatively between the posterior stabilized and cruciate retaining groups; mean change in Oxford score 22.45 versus 22.16 (p = 0.675), mean change in WOMAC score 44.00 versus 43.14 (p = 0.582), nor at 5 years, mean change in Oxford score 22.84 versus 23.47 (p = 0.43), mean change in WOMAC score 42.19 versus 43.35 (p = 0.538) or 10 years, mean change in Oxford score 23.66 versus 24.54 (p = 0.520), mean change in WOMAC score 39.42 versus 43.95 (p = 0.122). The change in WOMAC scores were subanalyzed based on the three components (pain, stiffness, and physical function). The posterior stabilized group had greater improvements in stiffness at 1 year following surgery; mean improvement in stiffness score 3.76 versus 3.36 (p = 0.012); although this was not evident at 5(3.68 vs. 3.71, p = 0.862) or 10 years (3.65 vs. 3.99, p = 0.247) postoperatively. No significant difference was seen in pain or physical function scores at any time postoperatively. Table 1 summarizes baseline patient demographics as well as pre- and postoperative scores. Figure 1 highlights pre- and postoperative Oxford scores and Figure 2 pre- and postoperative WOMAC scores. Table 2 summarizes the change in scores from pre- to postoperative.
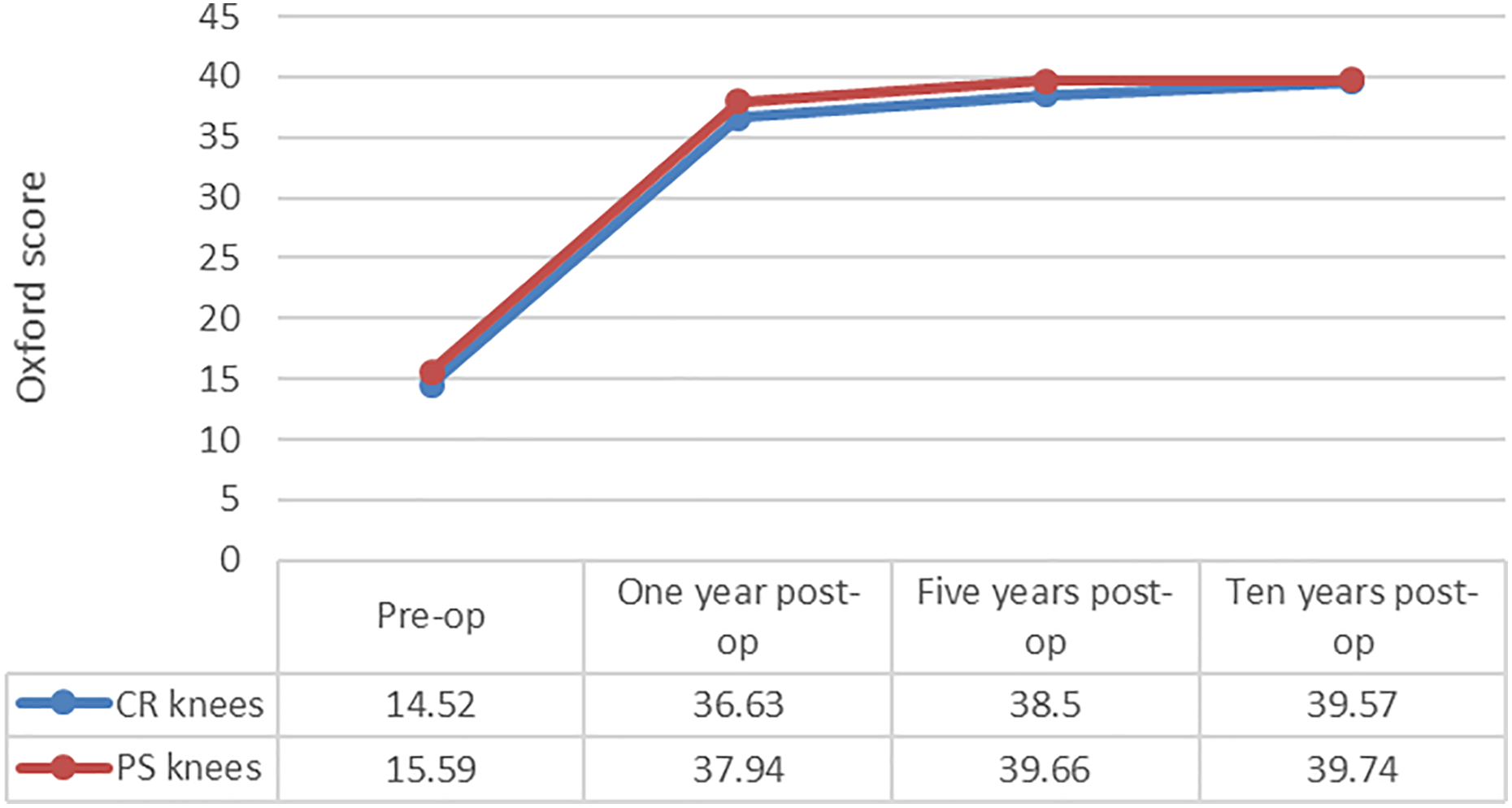
Comparison of PS and CR knees preoperative and 1-, 5-, and 10-year postoperative Oxford scores. CR: cruciate retaining; PS: posterior stabilized.
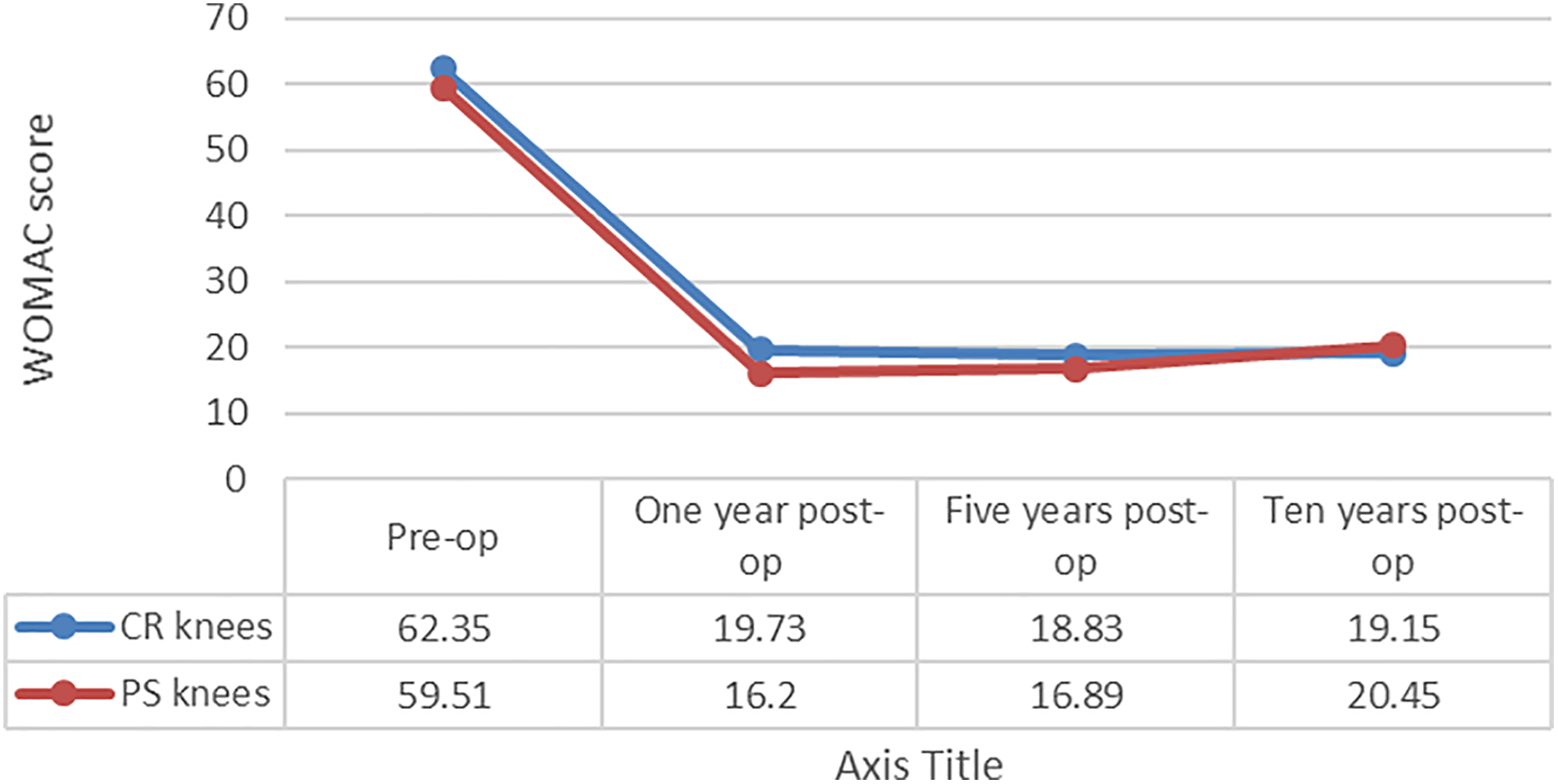
Comparison of PS and CR knees preoperative and 1-, 5-, and 10-year postoperative WOMAC scores. CR: cruciate retaining; PS: posterior stabilized; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Change in Oxford and WOMAC scores following adjustment for baseline differences between groups.a

CR: cruciate retaining; PS: posterior stabilized; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; SD: standard deviation; SEM: standard error of the mean; pre-op: preoperative; post-op: postoperative.
aBoldface values indicate statistical significance.
Discussion
There are multiple studies comparing posterior stabilized and cruciate retaining prostheses for primary total knee arthroplasty surgery. The majority of these studies are small series focused on kinematic, radiological, and early functional analysis. The goals of successful knee arthroplasty are the alleviation of pain and the restoration of knee function with long-term survival of implants. As patient expectations following knee arthroplasty increase, knee arthroplasty research is increasingly focused on clinically important differences in patient functional outcomes.
Theoretically there is a causal link between improved knee range of motion and patient function. In particular, certain important daily activities such as rising from a low chair rely on terminal knee flexion. Therefore, it is important to consider the kinematic differences between cruciate retaining and posterior stabilized implants in determining functional differences.
Cruciate retaining implants rely on the intact PCL, which becomes taut in deep flexion, preventing anterior femoral translation and producing femoral rollback. This is achieved by a combination of sliding and rolling movement creating a posterior shift in the femoro-tibial contact point and allowing the knee to flex without the posterior femur impinging on the posterior aspect of the tibia. However, recent kinematic studies have thrown doubt over this mechanism and have shown paradoxical anterior movement of the femoral condyles during high-flexion with higher peak femoro-tibial contact stress. 3,14 This may be a result of difficulty in adequately balancing the PCL or of pathological PCL function, as it may be involved in the degenerative disease process and no longer functions like a “normal” PCL, following knee replacement.
In contrast, cruciate substituting knee replacement relies on replacement of the PCL with a tibial polyethylene post, which articulates with a CAM between the femoral condyles. This CAM/post articulation in deep flexion prevents anterior femoral translation and mechanically reproduces femoral rollback. Kinematic studies have demonstrated that this mechanical rollback creates a smoother flexion arc and also a superior range of deep flexion. 3,14,15
The kinematic differences between CR and PS knee replacement designs have generally been borne out in the literature when knee range of motion is the primary outcome measure. Multiple studies have proved a small but statistically significant improvement in deep flexion in posterior stabilized knee replacements in both conventional and high-flexion design implants. 4 –9 A Cochrane review meta-analysis of trails complied by Jacobs et al in 2004 showed the mean gain in flexion to be 8.1° when posterior stabilized and cruciate retaining implants were compared. 6
The question of function in posterior stabilized knee replacements has been addressed in several studies, but these data are generally from small studies with only short- to medium-term outcomes recorded. To the best of our knowledge, no study to date has reported a significant functional advantage from PS knee replacements, despite superior range of motion. Kim et al. reported no functional difference in a series of predominantly female Korean patients who all achieved a knee range of motion exceeding that commonly seen in western patients. 10 Maruyama et al., 5 Yagishita et al., 4 and Seon et al. 7 also showed no significant differences between cruciate retaining and posterior stabilized prostheses in smaller series of Japanese patients. However, given the higher range of knee flexion reported in Asian patients, the generalizability of the results to Caucasian patients is questionable.
A meta-analysis conducted by Berick et al., which included 1265 knees from 12 randomized controlled trials reported significantly improved knee flexion and range of motion in PS knees with no difference in complication rates. 16 Ritter et al. reported that greater knee range of motion tended to result in improved functional outcome scores. 17 However, what remains uncertain is whether these small increases in knee motion in PS prostheses represent clinically relevant improvements that are recognized by patients.
Harato et al. reported 5-year functional results in a series of Canadian patients and found no significant difference between the CR and PS groups with regard to functional assessment. 8 Studies by Chaudary et al. 12 and Clark et al. 11 also showed no significant functional differences between CR and PS groups at an average of 2 years postoperatively. In the largest published series of 740 patients comparing function in PS and CR knee replacements Lozano-Calderón et al. demonstrated no significant differences in range of motion or function at 2 years postoperatively. 13
The question of long-term survivorship also remains largely unanswered. Of concern to proponents of posterior stabilized design, Abdel et al. have recently reported superior long-term survivorship at 15 years in CR total knee replacement when compared with PS knees. 18
Our study is the largest reported series, to the best of our knowledge, with 1287 patients comparing function between CR and PS knee replacements.
Baseline information
In our study, patients in the posterior stabilized group were significantly younger than patients in the cruciate retaining group. This would suggest a trend among the surgeons in this region toward using posterior stabilized implants in younger patients. We cannot account for this difference other than individual surgeon preference. In our area, some surgeons exclusively implant PS knees and some are occasional users. Among the occasional users, PS knees are often used in more difficult cases in which correction of significant deformity is needed. As such we could reasonably expect that the PS group would have worse pre- and postoperative scores. In fact, the posterior stabilized group had better preoperative scores than the cruciate retaining group. This likely relates to the fact that they were younger at the time of surgery, with superior baseline functional capacity. Furthermore, nearly double the number of CR knee replacements were implanted than PS knees more than this 10-year period, indicating a selection bias favoring CR knees in our area.
Primary outcome
The posterior stabilized group had better functional outcomes at 1 and 5 years postoperatively, although the difference did not reach statistical significance at 5 years. This may be a consequence of their better preoperative function as it is known that a major predictor of postoperative functional outcome is preoperative function. 19,20 However, it may also relate to a better restoration of normal knee kinematics as has been previously reported. 3,15
The change between preoperative and postoperative scores at 1, 5, and 10 years was used to determine the overall functional improvement following surgery. Our study found no difference in overall functional improvement between CR and PS groups, which suggests that either implant is equally efficacious in restoring function or that preoperative function is the most important determinant in functional status postoperatively.
Subanalysis of the three components of the WOMAC score (pain, stiffness, and physical function) showed superior overall improvement in stiffness in the posterior stabilized group at 1 year. Physical function scores were also improved although this did not reach statistical significance. This result suggests that the use of a PS implant confers a significant advantage to overall patient perceived range of motion and functional improvement following knee replacement surgery. This may be as a result of important kinematic differences between PS and CR implants. The same difference was not seen for change in pain scores. However, relief of pain is not likely to be influenced by an alteration in knee kinematics, provided that implants are well fixed and aligned. Similarly, these differences were not seen at 5 or 10 years postoperatively. It could be postulated that the small improvements in knee range of motion conferred by the PS design results in improved functional outcomes and patient satisfaction in the short-term, but as time passes patients become more accepting of their knee motion and, therefore, this difference disappears.
Methodological considerations
The choice of knee score used to determine clinical function in this study is important to consider when interpreting the study results. The Oxford knee score is a validated score, comprising of 12 questions which assess knee pain and function. 21 The WOMAC score is a validated scoring system specific to locomotor capability that is widely used to evaluate patients undergoing total knee arthroplasty surgery. 22 The WOMAC is composed of three sections: pain, stiffness, and physical function, with a higher score corresponding to poorer function. Numerous studies have reported on the minimally clinical important difference (MCID), which is the smallest change in score that patients perceive as meaningful. The MCID has been reported as 5.2 for the Oxford knee score and 0.51–1.33 per component of the WOMAC score (i.e., pain, stiffness, and physical function). 23 Therefore, the differences in WOMAC stiffness and physical function scores between the PS and CR groups are not only statistically significant but may also be sufficient to represent functionally perceivable differences. 23 However, there are some intrinsic limitations to the use of the Oxford and WOMAC scores, which may not be able to detect subtle changes in function. The fact the MCID for these scores are small indicates that even a small change in score may represent a clinically important change in function. Studies have also demonstrated a significant ceiling effect with the WOMAC and Oxford knee scores. 24 The use of a more sensitive score may be required to detect small changes in function. A score such as the HAAS may be more useful for use in younger patients who have higher functional expectations following arthroplasty, while traditional scores remain useful in lower demand patients. 25
Our study has certain limitations. Not all scores were available for all patients at all time points. Specifically, 10-year follow-up was only available for a small number of patients, those who had undergone surgery in 2005 and 2006. Longer follow-up is necessary to determine whether the trends seen in the early postoperative period would be evident in the long-term. Our study has a number of strengths. It is the largest single series in the literature, which includes long-term follow-up (1, 5, and 10 years), and all data were collected prospectively with baseline scores used to calculate the actual change in function from preoperatively to postoperatively.
Previous studies have reported that the WOMAC and Oxford scores at 6 months are predictive of later scores. 26 However, our study has shown improved early postoperative range of motion in the PS group which was not evident at 5 or 10 years postoperatively.
The groups were heterogeneous in terms of implants used (based purely on individual surgeon’s preference and experience). The posterior stabilized group contained the PFC (Johnson & Johnson Orthopaedics, Norderstedt, Germany), Genesis (Smith & Nephew, Memphis, Tennessee), Triathlon (Stryker, Kalamazoo, MI), and Optetrak (Orthotech, Gainesville, Florida) prostheses. The cruciate retaining group included the LCS (DePuy Orthopaedics, Warsaw, Indiana), PFC (Johnson & Johnson Orthopaedics), Genesis (Smith & Nephew), and Optetrak (Orthotech) prostheses. This diversity in implants is a potential source of bias due to subtle kinematic differences between different implant designs. However, this more accurately reflects real-life practice and makes our results generalizable to the wide range of knee replacement implants currently in clinical use. In this regard, this perceived weakness is actually a strength of the study. A subgroup analysis based on implant type has not been performed, given the sample size of the studies, but it is potentially an area for further investigation.
Conclusions
This study has a number of important clinical findings. Similar to previous studies reporting a more accurate reflection of normal knee kinematics and superior range of motion with the use posterior stabilized prostheses our study has shown better short-term functional outcomes with posterior stabilized prostheses, specifically with regard to stiffness and to a lesser extent physical function also. This was not, however, sustained at 5 and 10 years postoperatively. The findings of this study are potentially important and should guide surgeons when selecting which prosthesis to implant in their patients. However, further research into this field is necessary and only through a large prospective randomized controlled trial would it be possible to truly determine which implant is superior in terms of long-term functional outcome.
Footnotes
Acknowledgments
We thank Dr Chris Frampton, Statistician, University of Otago for his support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.