
Abstract
Purpose:
The purpose of the present study was to follow up Japanese patients with deep vein thrombosis (DVT) after total knee arthroplasty (TKA) and also to examine factors associated with residual thrombus within the sixth postoperative month.
Methods:
DVT evaluation was performed by noninvasive venous ultrasonography. We retrospectively reviewed 88 Japanese patients (88 knees) receiving primary unilateral TKA, who had no preoperative DVT. We examined the influence of the following four factors on postoperative DVT: (1) patient factors (age, sex, body height, body weight, and body mass index), (2) surgical factors (operation time, bleeding amount, avascularization time, and anesthesia method), (3) postoperative factors (bleeding amount, period to ambulation, period of venous foot pump use, and ratio of graduated compression stocking use), and (4) DVT conditional factors (location, length, number of vein branches, and the presence of >5 mm vasodilatation).
Results:
The total prevalence of venous thromboembolism (VTE) was 62.5% (55 of the 88 patients). Among the 55 VTE patients, the rates of distal and proximal DVT were 96.4% and 3.6%, respectively. Bilateral DVT was found in 34.5%, while unilateral DVT on the surgical and nonsurgical sides were 52.7% and 12.7%, respectively. Asymptomatic pulmonary embolism was 1.8%. DVT was exacerbated in five patients (11.9%), of whom three showed additional thrombus formation. The remaining two patients had thrombus elongation or propagation from distal to proximal veins. In comparisons between thrombus-unresolved and -resolved groups within the sixth postoperative month, statistical significances were found in the incidence of bilateral DVT (50.0% vs. 15.4%, p = 0.02) and unilateral DVT (43.8% vs. 76.9%, p = 0.02). On the other hand, operation time (107.0 ± 17.3 min vs. 94.5 ± 11.9 min, p = 0.01) and avascularization time (99.8 ± 17.6 min vs. 88.0 ± 11.5 min, p = 0.01) in bilateral DVT patients were significantly longer than in unilateral ones.
Conclusion:
Our results suggest that an extended operation and avascularization time may be a risk factor for bilateral DVT and residual thrombus over 6 months.
Introduction
Total knee arthroplasty (TKA) may entail a substantial risk of postoperative deep vein thrombosis (DVT). According to the American College of Chest Physicians (ACCP) Evidence-Based Clinical Practice Guidelines (eighth edition), 1 surgery for DVT is classified as a high-risk procedure due to the possible occurrence of venous thromboembolism (VTE). Pulmonary embolism (PE) is also of concern during postoperative ambulation and defecation/urination, possibly leading to fatal complications. 2 According to the ACCP Guidelines, without thromboprophylaxis, the rates of proximal and total (including proximal and distal) DVT were 5–22% and 41–85%, respectively. 1 On the other hand, guidelines for VTE prevention proposed by the Japanese Orthopaedic Association (JOA) showed that when no thromboprophylaxis was given, the incidences of proximal and total VTE were 9–16% and 50–60%, respectively. 3 A typical thromboprophylaxis includes drug therapy (e.g. usage of a low-molecular-weight heparin and factor Xa inhibitor) and physical therapy (e.g. usage of graduated compression stocking (GCS) and intermittent pneumatic compression (IPC)). However, even when such therapies are properly applied, some patients might develop postoperative VTE. To date, reports on detailed follow-ups of Japanese patients with DVT after joint replacement surgery are quite limited.
The purpose of the present study is to follow up Japanese patients with postoperative DVT after TKA and to examine factors associated with residual (unresolved) thrombus within the sixth postoperative month. DVT evaluation was carried out based on noninvasive lower extremity venous ultrasonography (US).
Patients and methods
This study was approved by the Institutional Review Board of Tokyo Medical University, and written approval statements were collected from all patients before surgery. Between January 2011 and March 2013, 146 primary TKAs were performed in 132 patients. All operations were performed by five surgeons (TT, TI, TM, TS, and KY) at a single center. Of these 132 patients, we retrospectively reviewed 88 Japanese patients (88 knees) receiving primary unilateral TKA, who had shown no preoperative DVT according to US examination (44 patients with preoperative DVT were excluded). The patients consisted of 12 males and 76 females with underlying diseases including osteoarthritis (74 knees), rheumatoid arthritis (11 knees), and femoral condyle necrosis (3 knees). Their mean age at surgery and body mass index (BMI) were 73.5 years (range, 50–87 years) and 25.7 kg/m2 (range, 16.9–34.7 kg/m2). General and spinal anesthesia were performed in 81 and 7 patients, respectively.
Scorpio® cruciate retaining, posterior-stabilized, and total stabilizer design knees (Stryker Orthopaedics, Mahwah, New Jersey, USA) were used in 82, 5, and 1 patients, respectively. Cemented TKAs were performed in all patients via mid-vastus approach using a tourniquet, and GCS or IPC device was used for the nonsurgical leg. A venous foot pump (VFP) (AV-Impulse Foot Pumps Model 6000, Covidien, Ireland) was attached to both feet postoperatively, and an indwelling drain was used for 2 days.
Within the seventh postoperative day, US examination was conducted by a clinical vascular technologist (AO) using cold flow duplex scanners (Xario™ XG SSA-680A; Toshiba Medical Systems, Tochigi, Japan) with 3.5-MHz convex and 7.5-MHz linear transducers. Diagnosis of DVT was made by pulsed Doppler, color Doppler, and compression method, and the detection criteria were observation of an intravenous thrombus, lack of venous compressibility, and blood flow deficiencies. According to past reports, 4 –8 US examination can offer 79–100% sensitivity, 90–100% specificity, and 94–100% accuracy for detecting proximal DVT, and 83–92% sensitivity, 98–100% specificity, and 97–98% accuracy for detecting distal DVT. Nevertheless, it is well known that US is largely operator-dependent and that major variations can be seen in the superficial femoral vein (SFV) and popliteal vein. 9 Therefore, all the examinations were performed by a single experienced sonographer (AO), who looked for two vessels in the popliteal fossa and for a duplicated SFV. The examination was conducted in three different directions (medial, posterior, and lateral), and small thrombi were also diagnosed in the lower legs. Although such examination is quite time-consuming (approximately 45 min), a potential venous thrombus will not go undetected.
After drain removal, continuous passive motion therapy and gait training with a walker were started. VFP was discontinued when walker-supported ambulation became stable, and all patients were managed with GCS for 2 weeks. Administration of enoxaparin 4000 IU/day was started within the 48th postoperative hour and continued up to day 7. According to the DVT treatment protocol shown in Figure 1, IPC was discontinued when DVT was detected by US. For patients with distal DVT, warfarin was administered in addition to enoxaparin and was continued until thrombus resolution or the third postoperative month, with a target range of the international normalized ratio of prothrombin time of 1.5–2.5. On the other hand, enoxaparin was discontinued for patients with proximal DVT. Continuous venous injection of unfractionated heparin and warfarin administration were begun. PE was monitored carefully by contrast computed tomography.

Treatment protocol for DVT patients adopted into this study. DVT: deep vein thrombosis.
We recorded the following four factors in DVT patients: (1) patient factors (age, sex, body height, body weight, and BMI), (2) surgical factors (operation time, bleeding amount, avascularization time, and anesthesia method), (3) postoperative factors (bleeding amount, period to ambulation, period of VFP use, and ratio of GCS use), and (4) DVT conditional factors (location, length, number of vein branches, and the presence of >5 mm vasodilatation).
Two-tailed Student’s t-test and χ2-test were performed with the aid of commercial software (JMP® 11; SAS Institute Inc., Cary, North Carolina, USA) to test for statistically significant differences in the above factors between thrombus-unresolved and -resolved patients, and between patients with bilateral and unilateral DVT. Statistical differences in these comparisons were considered significant at p < 0.05.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
US scan was conducted on average postoperative day 4.1, and the VTE/DVT prevalence was summarized in Table 1. The total prevalence of VTE was 62.5% (55 of the 88 patients (knees)). Among the 55 VTE patients, the rates of distal and proximal DVT were 96.4% (53 patients) and 3.6% (2 patients), respectively. Bilateral DVT was found in 34.5% (19 patients), while unilateral DVT on the surgical and nonsurgical sides occurred in 52.7% (29 patients) and 12.7% (7 patients), respectively. Asymptomatic PE was seen in one patient (1.8%). The initial locations and postoperative DVT formation rates of all patients and the unresolved group were summarized in Table 2.
Prevalence and location of VTE.

VTE: venous thromboembolism; PE: pulmonary embolism; DVT: deep vein thrombosis.
Initial locations and postoperative DVT formation rates in all patients and unresolved group.

Sol v: soleus vein; G v: gastrocnemius vein; Pt v: posterior tibial vein; Pe v: peroneal vein; Pop v: popliteal vein; Sf v: superficial vein; DVT: deep vein thrombosis.
A total of 13 VTE patients dropped out or were excluded due to incomplete follow-up. Of the remaining 42 DVT patients who had undergone a routine US examination, thrombus resolution were observed in 26 (61.9%). The presence of residual thrombus over the sixth postoperative month was confirmed in 38.1% (16 patients), and DVT was exacerbated in five patients (11.9%), three of whom showed additional thrombus formation. The remaining two patients had thrombus elongation or propagation from distal to proximal veins. DVT was exacerbated within the third postoperative month in four of the five patients, two of whom had diabetes mellitus and two had varicose veins of lower extremities. Each examined factor was compared between the thrombus-unresolved and -resolved patients and summarized in Table 3. The statistical significance was found in the incidence of unilateral DVT (50.0% vs. 84.6%, p = 0.02) and bilateral DVT (50.0% vs. 15.4%, p = 0.02). Although initial DVT formation, resolved, and unresolved rates after TKA were compared between groups with thrombus length of more or less than 5 cm, no significances were found in these rates (Table 4). Operation time (107.0 ± 17.3 min vs. 94.5 ± 11.9 min, p = 0.01) and avascularization time (99.8 ± 17.6 min vs. 88.0 ± 11.5 min, p = 0.01) for patients with bilateral DVT were significantly longer than those with unilateral DVT (Table 5).
Comparisons of each examined factor in the thrombus-unresolved and -resolved patients within the sixth postoperative month.a

BMI: body mass index; DVT: deep vein thrombosis; VFP: venous foot pump; GCS: graduated compression stocking.
aNA: not available due to the small number of patients
b p < 0.05.
Comparisons of initial DVT formation, resolved, and unresolved rates after TKA between patient groups with thrombus length of more than or less than 5 cm.a

DVT: deep vein thrombosis; SD: standard deviation; TKA: total knee arthroplasty.
aNote that no significances were found in these rates between the groups.
Comparisons of each examined factor between the patient groups with bilateral and unilateral DVT.a
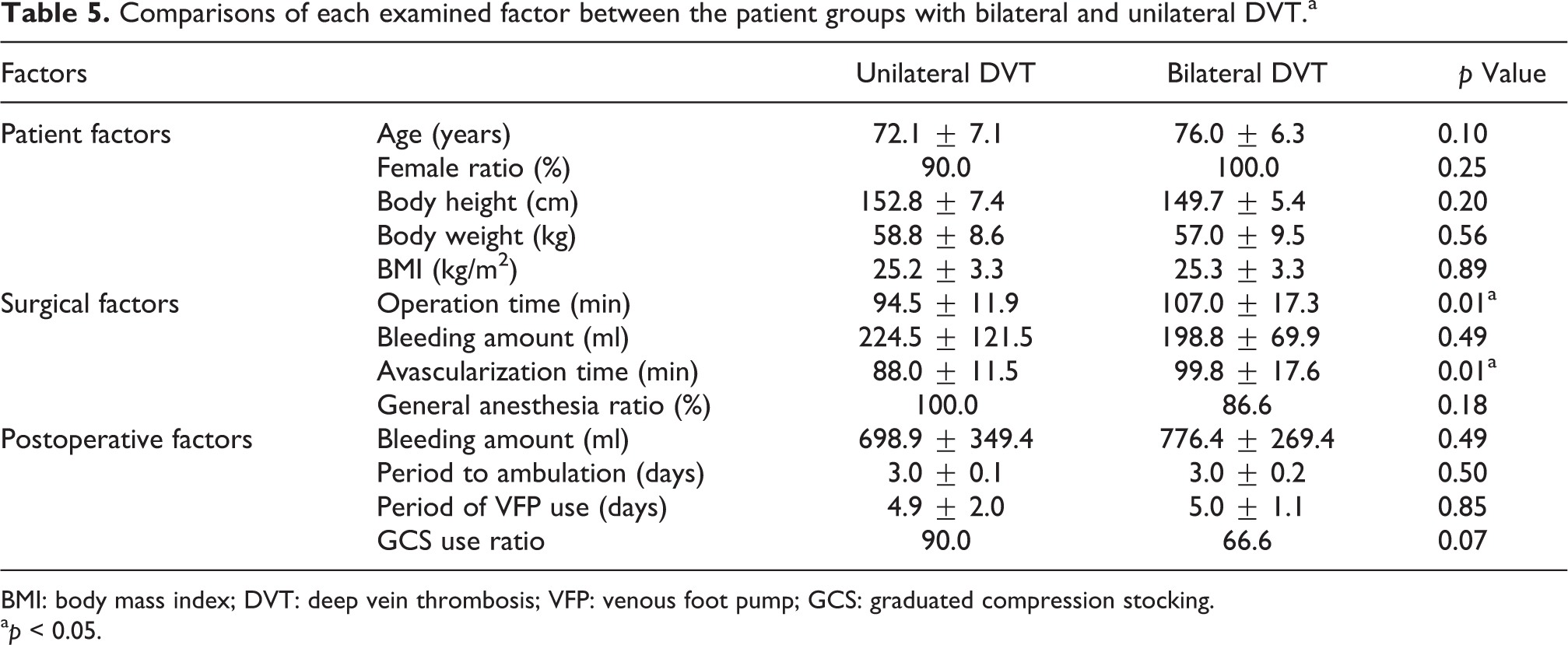
BMI: body mass index; DVT: deep vein thrombosis; VFP: venous foot pump; GCS: graduated compression stocking.
a p < 0.05.
Discussion
Although several authors have reported the incidence of DVT after TKA, limited data are available on the detailed clinical course of postoperative DVT, especially in Japanese patients. In one study, Maynard et al. 10 followed 76 knees after TKA and reported the prevalence of DVT as 58% (44 knees), including 12% that had thrombi proximal to the deep veins of the calf. However, no limbs with thrombi less than 9 cm in length at early venography demonstrated thrombosis in or proximal to the popliteal vein at late venography. Oishi et al. 11 followed 117 knees after TKA and reported a DVT prevalence of 23% (27 knees), including 19% (5 knees) with proximal propagation at the 14th postoperative day. Although Kim et al. 12 reported a DVT rate after TKA of 42% (143 of the 343 knees), all calf thrombi resolved spontaneously within the sixth postoperative month. Yamaguchi et al. 13 followed 24 patients after TKA and reported a DVT rate of 4% on the day after surgery, 50.0% at day 1, 58.3% at day 4, and 20.8% at day 14 in patients who received fondaparinux during the 14th postoperative day.
As for the postoperative course of distal DVT formed in veins of the lower extremities, Lohr et al. 14 followed 75 DVT patients and reported that 24 (32%) of them propagated, and that 11 (46%) of these 24 spread into the popliteal or larger veins of the thigh. MacDonald et al. 15 reported that, of 135 limbs with isolated gastrocnemius and soleal vein thrombosis (IGSVT), thrombi propagated to the level of the popliteal vein in only 3%, and no IGSVT propagated to the level of the popliteal vein beyond 2 weeks from the time of DVT diagnosis by US. Furthermore, in a review of 1355 DVTs formed in lower extremity veins, Righini et al. 16 observed that 58 (9.5%) of the 610 untreated DVT patients presented with propagation into proximal vein, and 31 (4.2%) of the 745 DVT patients receiving anticoagulation therapy also showed proliferation into proximal vein. Our present study showed that postoperative DVT was found in 62.5% (55 of the 88 patients), and, among these 55 patients, the distal type was observed in 96.4% (53 of the 55 patients) (Table 1). Of the 42 patients who had undergone a routine US examination, DVT remained in 38.1% (16 patients) over 6 months and became exacerbated in 11.9% (5 patients). According to the past literature, 17 primary risk factors for postoperative DVT have been identified as follows: previous PE or DVT, malignant tumor, congestive heart failure, chronic obstructive pulmonary disease, diabetes mellitus, inflammatory bowel disease, antipsychotic drug use, chronic indwelling central venous catheter, permanent pacemaker, internal cardiac defibrillator, stroke with limb paresis, nursing home confinement or current or repeated hospital admission, and varicose veins. In our study, among 16 patients with residual thrombus, 1 had malignant tumor, 3 had diabetes mellitus, and 3 had varicose veins of lower extremities, while among 5 patients with DVT exacerbation, 2 had diabetes mellitus and 2 had varicose veins of lower extremities. Nevertheless, since 9 of the 16 patients showed no obvious risk factor, their actual influence on DVT is unknown. It should be noted that operation time and avascularization time were significantly longer in patients with bilateral DVT than those with unilateral DVT of the surgical side (Table 5). Thrombi remained significantly longer in patients with bilateral DVT as compared to unilateral DVT of the surgical side. These results suggest that extended operation and avascularization time may be a risk factor for bilateral DVT as well as residual thrombus over 6 months.
We found DVT in 75% (9 of the 12) of patients who had received physical therapy only, while the rate was 60.5% (46 of the 76) in patients who had received both physical and drug therapy; the difference in their DVT rates was not significant (p = 0.34). In one study on the treatment of lower extremity DVT, Lautz et al. 18 observed that thrombi resolved in 61.2% of the patients treated by anticoagulation therapy, while they resolved in 40% of untreated patients. Their results emphasize the importance of anticoagulation therapy for patients with lower extremity DVT. Nevertheless, Sales et al. 19 reported that there were no significant differences in the IGSVT resolution rates between patients with and without anticoagulation therapy. Tsuda et al. 8 reported that, in an Asian population, asymptomatic distal DVT had a benign course regardless of DVT size after total hip arthroplasty and the patients did not require anticoagulation. Furthermore, Righini et al. 16 pointed out that the systematic use of distal US may increase the prevalence of diagnosed DVT, leading to a risk of overtreatment. In the above contexts, no consensus has yet been achieved regarding the necessity of treatment for asymptomatic DVT. All our patients with lower extremity thrombi were asymptomatic DVT or PE, and no occurrence of adverse events due to VTE was observed. Although effectiveness of chemotherapy for asymptomatic DVT remains to be fully elucidated, the resulting outcomes are still incomplete and must rely on future studies.
This study had limitations. First, this study included only Japanese patients whose unmatched numbers between men and women were examined (12 males and 76 women). Second, all DVTs were diagnosed by noninvasive US, and the results may not be directly comparable to other studies using other imaging modalities (e.g. invasive venography). Third, since small thrombi were also detected in the lower legs over a relatively longer time period, our results may lead to higher detection rates as compared to other US studies. Fourth, a routine US examination was not performed for subjects without postoperative DVT, and therefore diagnosis of any new thrombus formation was not possible. However, no incidence of adverse events was observed during the study period. Despite the above limitations, our results suggest that an extended operation and avascularization time may be a risk factor for bilateral DVT and residual thrombus over 6 months.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.