
Abstract
Purpose:
This study aimed to investigate the effect of knee joint structural destruction on frontal plane hip and ankle joint kinematics and kinetics during the stance phase of walking in patients with differing severities of knee osteoarthritis (KOA).
Methods:
An early KOA group consisted of eight subjects with bilateral knee Kellgren–Lawrence (KL) scale scores of 1 or 2. An established KOA group comprised nine subjects (18 knees) with KL scores of 3 or 4. To measure walking, the data were obtained using the motion analysis system and force plates. From the ground reaction force data, the stance phase of gait was divided into five periods.
Results:
In the established KOA group, the hip joint was significantly abducted, and the knee joint had significantly greater varus positioning during the stance phase. In addition, in the established KOA group, a significant knee abductor moment was observed during the stance phase. In contrast, in the early KOA group, the ankle joint showed a significant inversion moment during the stance phase, but in the established KOA group, the ankle joint moment was very small.
Conclusions:
The structural destruction of the knee joint in the frontal plane in patients with the established KOA changes the movement of the hip and the moment of the ankle.
Introduction
An increase in external knee adduction moment is considered a characteristic of the gait of patients with medial knee osteoarthritis (KOA) 1 –3 and causes cartilage degeneration and disability. 4,5 It has been reported that some compensatory methods of walking may reduce medial load of the knee joint in patients with medial KOA. 6,7 Therefore, it is believed that the gait of the patients with medial KOA influences not only the knee joint but also the functions of the hip and ankle joint.
The frontal plane of the hip joint acts to stabilize the pelvis and trunk and controls the movement of the hip joint. 8 In patients with medial KOA, the abductor and adductor muscular strength of the hip joint is important for decreasing the external knee adduction moment, 9,10 and the decreased strength of the hip abductor muscle is accompanied by the progression of KOA. 11 Furthermore, the function of the hip joint surrounding muscle does not reduce the load on the medial part of the knee joint, but its involvement has been reported in the alleviation of KOA symptoms. 12 It has been reported that strengthening of the hip joint muscles is crucial for decreasing pain and the external knee adduction moment during the stance phase of walking in medial KOA patients, 10 –12 but the effect on the hip joint due to the difference in severity of KOA is not completely understood.
In contrast, several problems related to the foot, such as flatfoot and pronated foot, have been reported in KOA. 13,14 The change in the shape of the foot in KOA may cause pain, restriction of the daily activities, and damage to the articular cartilage. 14 –16 Since the movement of the foot has a close relationship with the tibia, the effect on the knee joint is marked, 17 and it is reported that the pronated moment of the subtalar joint during walking simulation increases due to the varus deformity of the knee joint. 18 In a past study, it was reported that patients with KOA found it difficult to demonstrate the plantar-flexor moment of the ankle joint that contributes toward forward progression during the terminal stance (TS) phase, 19 and the decrease of the ankle moment caused the mechanical load on the knee joint. 20 However, the influence on the movement of the frontal plane of the ankle joint due to the difference in severity of KOA is not fully understood.
This study aimed to investigate the effect of knee joint structural destruction on frontal plane hip and ankle joint kinematics and kinetics during the stance phase of walking in patients with differing severities of KOA. In this study, we hypothesized that the magnitude of the varus deformity in the knee joint influences the movement of the hip joint and ankle joint as well as the moment of the lower limb joint.
Materials and methods
Subjects
In this study, 17 subjects, who were orthopedic patients visiting the hospital for outpatient treatment of knee joint pain during activities of daily living, were enrolled. The subjects underwent bilateral, anteroposterior knee joint radiography, and the Rosenberg view, a load-bearing 45° flexion view, was also obtained by a radiology technician. To describe the knees, the Kellgren–Lawrence (KL) scale was used (1 = doubtful narrowing of the joint space, possible osteophyte development; 2 = definite osteophytes without definite joint space narrowing; 3 = presence of moderate (multiple) osteophytes or a definite narrowing of the joint space; and 4 = presence of large osteophytes or marked narrowing of the joint space). 21 An orthopedic surgeon examined the X-ray radiographs of the patients. The exclusion criteria were prior knee replacement surgery, rheumatoid arthritis, or unresolved injuries to any joint of the lower extremities. Additionally, those who could not walk independently, without any aids, or due to knee pain were excluded. Sixteen knees from eight subjects (three men and five women) recorded a KL scale score of 1–2, and the subjects had the following characteristics (mean ± SD): 73.38 ± 9.54 years of age, 1.54 ± 0.09 m height, 56.00 ± 9.77 kg weight, and 23.57 ± 3.21 kg/m2 body mass index (BMI). Eighteen knees from nine subjects (three men and six women) recorded a KL scale score of 3–4, and the subjects showed the following characteristics (mean ± SD): 75.25 ± 5.51 years of age, 1.52 ± 0.06 m height, 61.81 ± 7.69 kg weight, and 26.80 ± 3.05 kg/m2 BMI. Patients were then further categorized into two groups: patients with a KL scale of 1–2 were classified as early KOA (four knees did not undergo radiography but we classified them as early KOA group because they had pain and disability in performing daily life activities), and those with a KL scale score of 3–4 were classified as established KOA. An orthopedic surgeon measured the femorotibial angle (FTA) on the radiographs. Varus deformity was defined as FTA > 180°. FTA determined from radiography was 176.8° ± 1.3° and 185.3° ± 6.6° in the early and established KOA groups, respectively. All participants provided written informed consent, and the study was approved by our institution. The ethical approval for this study was obtained from the Ibaraki Prefectural University of Health Sciences Ethics Committee (Reference No. 559).
Gait analysis and data acquisition
To measure walking, kinematics and kinetics data were obtained at 200 Hz using an eight-camera motion analysis system (Vicon Nexus, Vicon, Oxford, UK). The ground reaction force data were recorded at 1200 Hz using two floor-mounted force plates (Kistler Instruments, Winterthur, Switzerland), and the data were synchronized with the motion capture data. The subjects walked barefoot along a level walkway at their habitual speed, and an average of three gait trials was collected for each subject and used for analysis. According to a lower extremity model of the Plug-In-Gait marker set, 22 a widely standardized marker arrangement for three-dimensional motion analysis, reflective markers of 9.5-mm diameter were placed directly over bilateral anatomical landmarks: the anterior and posterior superior iliac spines, lateral thighs, lateral femoral epicondyles, lateral shanks, lateral malleoli, calcanei and the tops of the feet at the base of the second metatarsals. After attaching the reflective markers, each subject was instructed to stand barefoot for a single static calibration in the standing position before the gait analysis. The gait parameters during stance phase, as determined by the force plate data, were normalized to the values at 100% during stance phase (foot-strike to toe-off = 100%) using spline interpolation. The stance phase of the gait was divided into five periods 23 : initial contact (0% of the stance: IC), loading response (16% of the stance: LR), midstance (50% of the stance: MS), TS (83% of the stance), and pre-swing (100% of the stance: PS).
The raw data were smoothed using a low-pass filter. The calculation of the joint moments was conducted in the same way as that described in a previous report. 24 Body segment parameter coefficients specific to the Japanese population were used, as reported previously. 25 Joint moment data were normalized to body weight. In this study, the motion of the foot in the frontal plane was defined as inversion (in which the sole faces inward)–eversion (in which the sole faces outward), according to the guidelines of the International Society of Biomechanics. 26
Statistical analysis
The independent Student’s t-tests were performed on the lower limb joint angles and the moments of the frontal plane in each period of established and early KOA. The values p < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS software version 19.0 (SPSS Inc., Tokyo, Japan).
Results
Joint kinematics of the lower extremities during the stance periods
The joint kinematics of the lower extremities for each stance period are shown in Figure 1 and Table 1. In the established KOA group, the hip joint was significantly abducted, and the knee joint was significantly in the varus position during the IC. Significantly greater knee joint varus was found during the LR in the established KOA group. In addition, during the MS, the adduction angle of the hip joint angle was significantly small, and the knee joint continued to exhibit the varus position from the initial stance in the established KOA group. During the TS, the hip joint was significantly in the abduction position, and the knee joint was significantly in the varus position in the established KOA group. During the PS, the knee joint exhibited a significant varus alignment in the established KOA group. There was no significant difference between the two groups in the inversion–eversion angle of the ankle in each phase.

Longitudinal data for the joint angles of the lower extremities during the stance phase of early and established KOA: (a) hip joint, (b) knee joint, and (c) ankle joint. The black line is the early KOA group, and the gray line is the established KOA group. The vertical lines indicate the standard deviations. KOA: knee osteoarthritis.
Joint kinematics in lower extremities during each stance period.
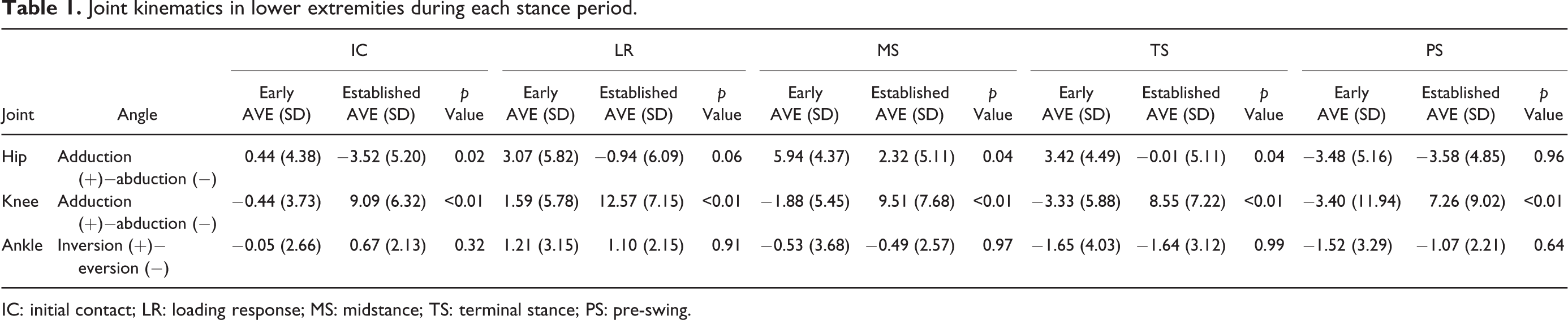
IC: initial contact; LR: loading response; MS: midstance; TS: terminal stance; PS: pre-swing.
Joint moments of the lower extremities during the stance periods
The joint moments in the lower extremities for each stance period are shown in Figure 2 and Table 2. In the established KOA group, the knee abductor moment was observed significantly during the LR, MS, and TS periods. In the early KOA group, the ankle joint showed a significant inversion moment during the MS and TS, but in the established KOA group, the ankle joint moment was very small during the stance phase. No significant difference was observed in the hip joint moment.
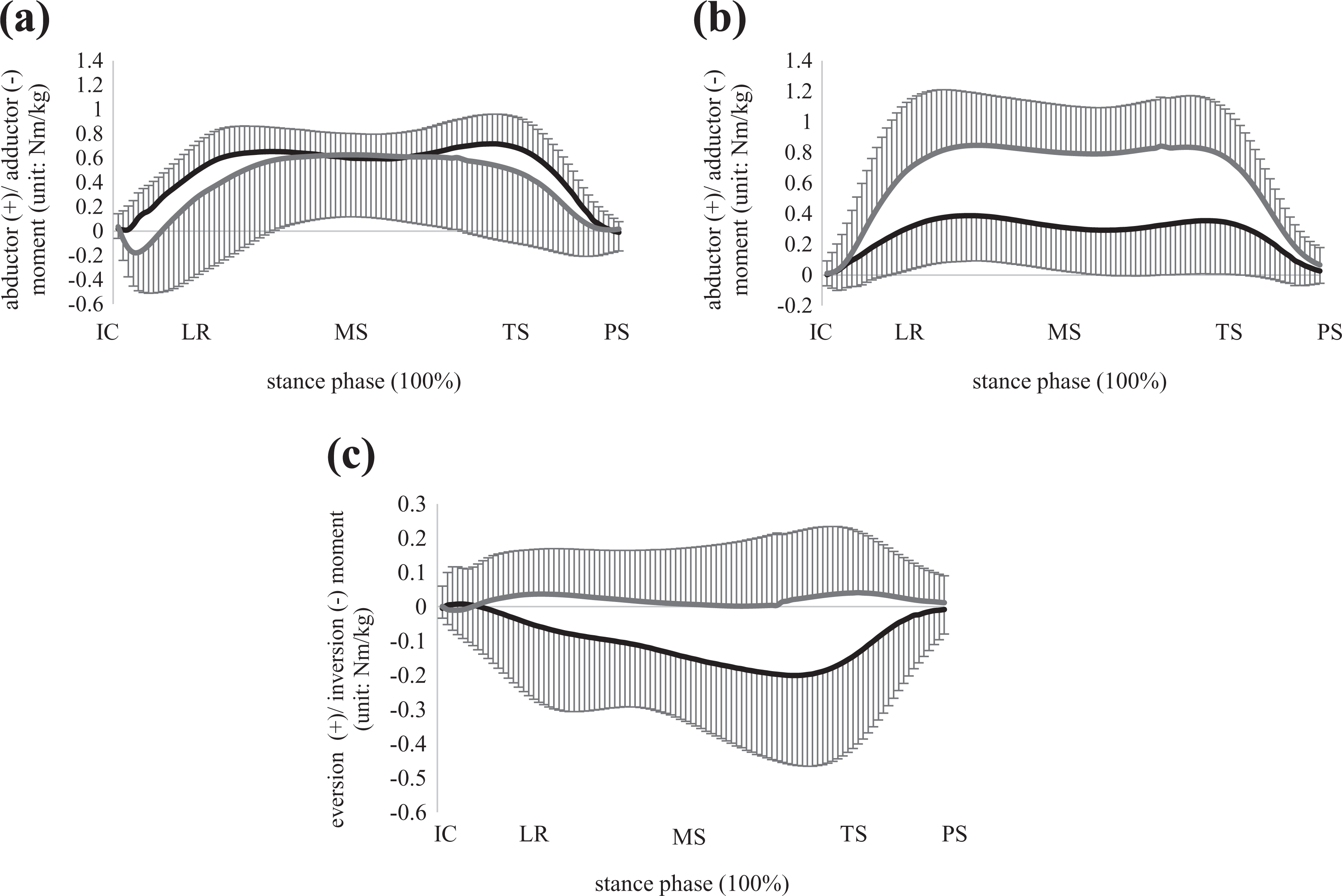
Longitudinal data for the joint moments of the lower extremities during the stance phase of early and established KOA: (a) hip joint, (b) knee joint, and (c) ankle joint. The black line is the early KOA group, and the gray line is the established KOA group. The vertical lines indicate the standard deviations. KOA: knee osteoarthritis.
Joint moments in lower extremities during each stance period.
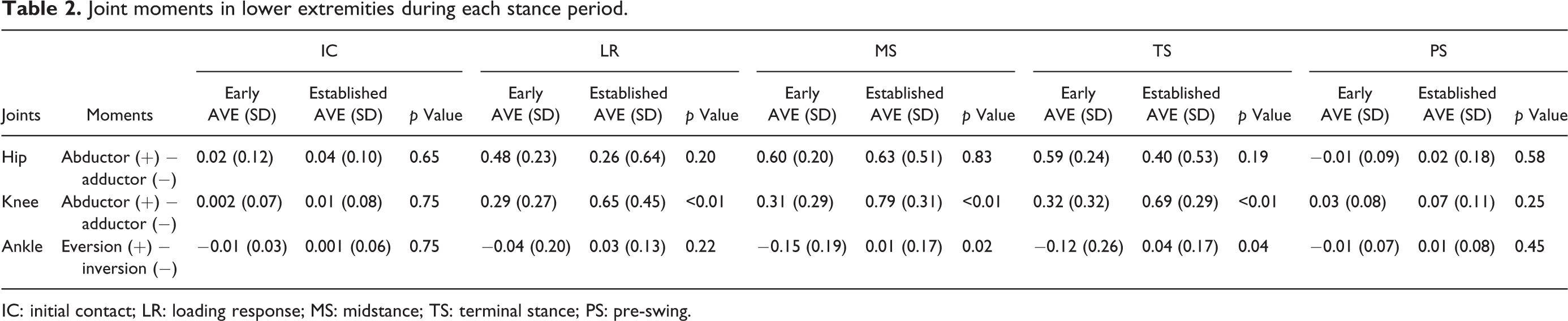
IC: initial contact; LR: loading response; MS: midstance; TS: terminal stance; PS: pre-swing.
Discussion
Since the joint load in medial KOA is represented by the external knee adduction moment, it is very important to evaluate the influence of the lower limb joint on KOA in the frontal plane. The results of this study showed a difference in the range of motion of the hip and the knee joints in the frontal plane. The hip joint moment was not significantly different between the two groups, but the established KOA group exerted the knee abductor moment. The ankle joint moment was significantly different at MS and TS during the stance phase.
Originally, in the one-leg supporting period during the stance phase, the pelvis is slightly depressed, and the hip joint retains the adduction position. 23 In contrast, our study showed that when the severity of KOA was increased, the tendency to bring the hip joint to an abduction position also increased. Although there was no significant difference, the abductor moment of the hip joint tended to decrease at the first peak and the second peak of the stance phase in the established KOA group. Compared to the early KOA group, the established KOA group held the knee joint in a varus position during the stance phase, and experienced difficulty to simultaneously hold the hip joint in an adducted position. The abduction position of the hip joint induces a large abductor moment on the knee joint. As this moment needs to exert a larger force to keep the balance against the knee adduction moment, tightness may be experienced in the lateral aspects of the knee joint.
Previous studies have shown that the range of movements of the ankle joint in the frontal plane clearly suggests a pronated foot in the medial KOA patients compared to normal individuals. 27,28 In the medial KOA, increasing the eversion of the foot decreased the external knee adduction moment by moving the center of pressure in the outward direction while inserting the lateral wedge to the sole. 29 In addition, in patients with medial KOA, it is reported that walking with the toe outward leads to biomechanical improvement, and the external knee adduction moment is decreased by moving the center of pressure in the outward direction. 30,31 In current study, even in patients with established KOA, there was no significant difference in the ankle joint movement in the frontal plane. In contrast, there was a significant difference in the ankle joint moment from MS to TS. In a previous study, the authors reported that the lateral translocation of the center of pressure during the stance phase in severe KOA affected the knee joint movement. 24 The results for the exerted moment of the ankle joint in the frontal plane, in this study, suggested that the decrease in the inversion moment in the ankle joint may affect the medial load on the knee joint in the established KOA group.
In the current study, focusing on the stance phase of walking in the patients with different degrees of severity of KOA, the changes in the movement and the moment of the lower limb joint in the frontal plane due to the structural failure of the knee joint were examined. As the varus angle of the knee joint during the stance phase increased in the established KOA group, the abduction angle of the hip joint also increased. The abducted position of the hip joint induces a large knee abductor moment to the knee joint. An excessive knee abductor moment causes tightness of the lateral part of the thigh and is a factor in lowering the function of the knee joint. Moreover, the movement of the ankle joint was not significantly different, but the inversion moment of the ankle joint in the established KOA group decreased significantly during the stance phase and the decrease in the inversion moment of the ankle joint affected the mechanical load on the medial part of the knee joint during the late stance phase. According to the results of our study, the mechanical load in the frontal plane of the knee joint was influenced by the movement of the hip joint and the moment of the ankle joint. It was thought that the strength of the hip joint adductor muscles and insertion of the lateral wedge to the sole needed to decrease the mechanical load of the frontal plane in established KOA.
This study has several limitations. It measures both lower limbs of all subjects, and the possibility that one joint motion may affect the motion of the other joint is undeniable. However, although the severity of KOA may be different, it is often that both knee joints suffer from disturbance. Furthermore, the number of subjects was not sufficient to generalize the results for all KOA cases. Thus, the future studies need to enroll an adequate number of subjects and consider longitudinal changes from the initial stage of KOA to validate these results.
Conclusion
The structural destruction of the knee joint in the frontal plane in patients with medial KOA was found to alter the movement of the hip joint and the moment of the ankle joint. As a therapeutic strategy for patients with KOA, interventions that regulate the movement in the frontal plane of the lower limb joint, in addition to the approach to the knee joint, are suggested to be of importance.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Grant-in-Aid for Project Research (1450-1) from the Ibaraki Prefectural University of Health Sciences.