
Abstract
The presence of anatomical anomalies such as absence of C1 posterior arch and presence of C2 high-riding vertebral artery may not allow a conventional C1–C2 fusion, and this patient will require occipitocervical fusion. A 62-year-old lady presented with cervical myelopathy. CT scan demonstrated an os odontoideum with C1–C2 dislocation. The posterior arch of atlas on right C1 vertebra was absent, and there was high-riding vertebral artery on left C2. MRI revealed severe cord compression with cord oedema. The chronic atlantoaxial dislocation was reduced successfully with skeletal traction. Hybrid C1–C2 fusion augmented with autogenous local bone graft with corticocancellous iliac crest bone graft was performed to avoid an unnecessary occipitocervical fusion. She was stable throughout surgery and discharged 6 days later. CT scan 6 months post-operation showed a solid posterior fusion mass. Hybrid C1–C2 fusion can be performed to avoid occipitocervical fusion despite presence of abnormal anatomy at C1 and C2 vertebrae.
Keywords
Introduction
Atlantoaxial dislocation (AAD) is defined by the loss of stability of atlas in relation to the axis. 1 The presence of anatomical anomalies of the C1 and C2 such as absence of the C1 posterior arch and high-riding vertebral artery of C2 had been described. 2,3 These anomalies posed a higher risk of complications during fixation of the C1–C2 vertebrae. We present a case of a chronic AAD secondary to os odontoideum with the absence of right C1 posterior arch and the presence of left high-riding vertebral vessel in C2 vertebra that prevented the use of conventional Harms, Magerl, Gallie or Brooks fusion technique.
Case presentation
A 62-year-old lady presented to our institution with a complaint of worsening neck pain for the past 2 years. She denied gait disturbance, weakness and numbness of the trunk and limbs. Past history revealed a whiplash injury in her 30s. On examination, she was able to stand up without assistance and had normal gait. Extension of the cervical spine was limited to 5° before she experienced pain over the occipital region of the head. There was hyperreflexia of both upper and lower limbs, positive Hoffman’s sign and positive scapulohumeral reflex.
Cervical spine radiography showed a lucency at the level of neck of dens with anterior displacement of atlas (Figure 1(a)). Computed tomography (CT) scan of cervical spine demonstrated the presence of an os odontoideum with a dislocated C1–C2 vertebrae resulting an increased C1–C2 interspinous distance (Figure 1(b)). A high-riding vertebral artery on the left C2 vertebra with an isthmus height of 2 mm and an absent posterior arch of the C1 vertebra on the right were noted (Figure 2). Magnetic resonance imaging (MRI) showed severe stenosis of 5.3 mm with spinal cord oedema (Figure 1(c)).

(a) Lateral view of cervical radiograph showed dislocated C1–C2 vertebrae; (b) sagittal view of cervical computed tomography scan demonstrated anterior dislocation of the atlas; (c) sagittal view of MRI scan of cervical spine demonstrated severe cervical stenosis with high signal within the spinal cord in T2-weighted image. MRI: magnetic resonance imaging.
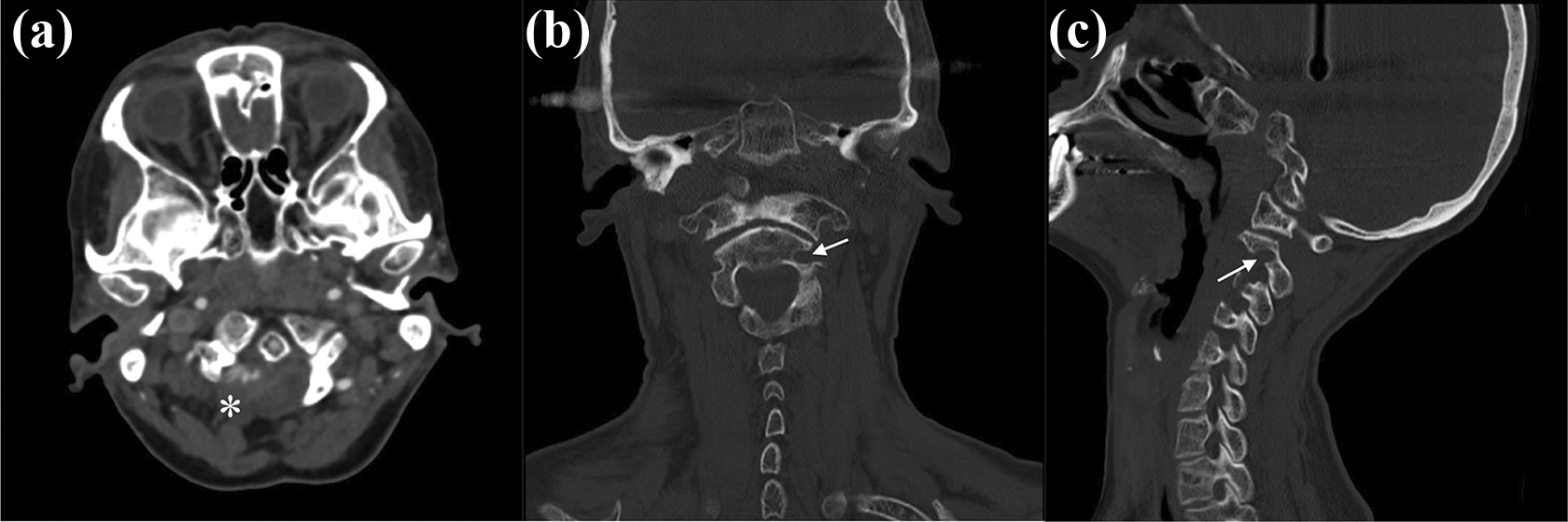
Axial view (a) of CT scan of cervical spine showed absence of right posterior arch of the C1 vertebra (white asterisk). Coronal view (b) and sagittal view (c) of CT scan revealed high-riding left C2 vertebral artery (white arrow). CT: computed tomography.
Skeletal traction was initiated with gradual increment, that is, 5–8 kg over 52 days. The chronic AAD was reduced without any complication and confirmed with a CT scan (Figure 3).

Sagittal view of CT scan of cervical spine demonstrated reduced chronic atlantoaxial dislocation with the use of skeletal traction. (a) Pre-traction; (b) Post-traction. CT: computed tomography.
Hybrid C1–C2 fusion was performed using a posterior approach. On the left side, C1 lateral mass screw was inserted. The entry point was created by drilling the lower half of the posterior arc before advancing into the lateral mass. Left C2 laminar screw was used instead of C2 pedicle screw to avoid injury to the high-riding vertebral artery. On the right side, a transarticular C1–C2 screw was inserted, as placement of C1 lateral mass screw was not possible due to the absence of posterior arch. Intraoperatively, the placement of screws was confirmed using image intensifier. A single oblique rod was used to connect all the screws to increase its stability (Figure 4 (a), (b), (e) and (f)). Fusion was augmented with local autogenous bone graft and corticocancellous bone graft, harvested from the right iliac crest. There were no complications intraoperatively. She was stable throughout the surgery and was discharged 6 days later. She wore a cervical collar for 6-month duration. CT scan performed 6 months following the surgery confirmed good bony fusion between C1–C2 vertebrae (Figure 4 (c), (d) and (g)).
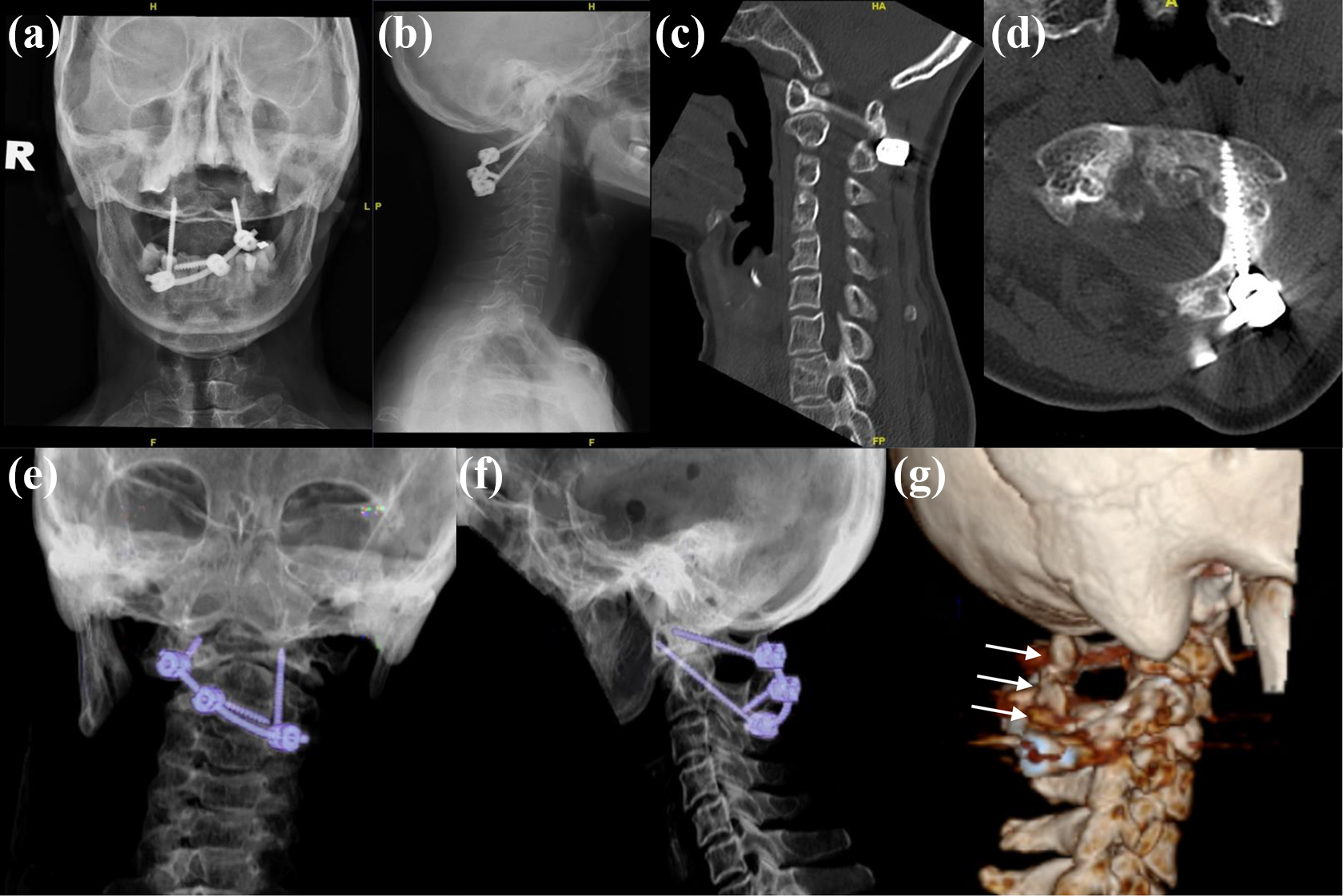
Post-operative radiographs (a, b) and CT scan (c to g) showed restoration of alignment of C1 and C2 vertebrae with transarticular screw on the right side and C1 lateral mass screw with C2 lamina screw on the left side, connected by an oblique rod. CT scan (c, d) and lateral view of coloured 3D (g) of the cervical spine 6 months post-operation demonstrated a solid C1–C2 fusion (white arrows). CT: computed tomography.
Discussion
AAD can be classified as reducible or irreducible. 4 To our knowledge, there was no standard guideline on reducing AAD. In an irreducible AAD, anterior decompression using transoral odontoidectomy may be needed; however, this procedure carries complications such as dysphagia, nasal phonation, cerebrospinal fluid leakage, incomplete decompression, pharyngeal wound sepsis, velopharyngeal insufficiency, haemorrhage, neurological deterioration and death. 5 –7 Alternatively, skeletal traction can be used to reduce the chronic AAD prior to posterior fixation of the C1–C2 vertebrae. Gerald et al. reported successful reduction and relief of anterior compression in most patients with irreducible AAD. 7
Surgical fixation of C1–C2 vertebrae in the presence of anatomical anomalies of the C1 and C2 vertebrae such as absence of C1 posterior arch and high-riding vertebral artery of C2 vertebra can be challenging. Conventional methods such as posterior wire stabilization described by Gallie et al., 8 transarticular screws fixation described by Magerl et al. 9 and polyaxial screws and rods fixation by Harms et al. 10 were commonly used methods to fix the C1–C2 vertebrae. However, these methods may not be possible or may pose a higher risk of complications in the presence of these anomalies mentioned above. Another option of treatment for this case was to perform posterior occipitocervical fusion.
In this case, C2 laminar screw was inserted instead of C2 pedicle screw on the left side due to the presence of high-riding vertebral vessels. On the right side, a transarticular C1–C2 screw was inserted instead of C1 lateral mass screw and C2 pedicle screw because of the absence of C1 posterior arch that did not allow screw or wire fixations. The construct was further stabilized using a single oblique rod to provide a better biomechanical strength. With the use of the local autogenous bone graft and cortico-cancellous bone graft, harvested from the right iliac crest, solid fusion between left C1 posterior arc and C2 lamina was achieved at 6 months post-operation.
Conclusion
Hybrid C1–C2 fusion can be performed in chronic AAD secondary to os odontoideum, with the absence of right C1 posterior arch and the presence of left high-riding vertebral vessel in C2 vertebra, to avoid unnecessary occipitocervical fusion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.