
Abstract
A 20-year-old patient came to the sport medicine clinic for bilateral forefoot pain during sport activities (running) progressing for the last 3 months. Thanks to a positive measurement of the compartment pressure during a running test reproducing the symptomatology and exclusion of classical differential diagnosis, a bilateral chronic compartment syndrome of the lateral forefoot was confirmed. Three months after a surgical fasciotomy, the patient fully recovered. No previous study described this specific compartment of the forefoot.
Introduction
Compartment syndrome refers to all symptoms linked to an elevation of intra-compartmental pressure in a closed non-elastic muscle compartment surrounded by fascia and bone.
Common aetiologies of compartment syndromes are classified into two categories: acute (fractures, direct traumas, vascular problems, burnings, casts) or chronic (exertion induced).
Even if compartment syndrome can occur in all compartments of the body, it is mainly famous after fracture of the lower leg (1.2% after closed tibial diaphyseal fracture) and the forearm. 1,2 Concerning the forefoot, acute syndromes are largely unrecognized but some authors 3 reported a rate of 25% in Chopart dislocations and 34% in Lisfranc dislocations. Chronic syndromes seem to be far more infrequent with only few case reports in the literature. 4 –10
The anatomy and the number of compartments have been discussed for a long, but a most recent publication described nine compartments in the forefoot. 11 This case report is dealing with a non-previous described location of chronic bilateral lateral compartment syndrome of the forefoot induced by exertion.
Case report
A 20-year-old man studying in Sport Science and Physical Activity, without any past medical history of trauma or disease, came to the sport medicine clinic for focused pain of the lateral part of the forefeet occurring with exertion especially after 10 to 20 min of running. His symptoms lasted for 3 months despite the use of ice and non-steroidal anti-inflammatory drugs and avoiding his regular sport training. The patient is a well-fit young man practising lots of sports including rugby and cycling at a non-competitive level. No recent changes in activities and sports devices have been reported by the patient during the previous months.
Clinical examination only showed a bulge aspect of the lateral part of the feet (Figure 1).

Aspect of the feet (bulge aspect of the lateral part) on clinical examination.
X-rays (Figure 2) and MRI (Figure 3) were carried out to eliminate frequent diagnoses like stress fracture and periostitis or less usual conditions like tenosynovitis, vascular and neurological entrapment syndrome, primary muscular disorders, and tumours.

X-rays (antero-posterior view) of the feet, showing soft tissue swilling at the lateral aspect of the forefeet.

MRI imaging (axial and coronal views) of the right foot with a bulge aspect of the soft tissues in the lateral compartment.
A running test on a treadmill reproducing the symptomatology was undertaken to measure the compartment pressures of the painful location. Bilateral pain of the lateral part of the forefeet occurred after 10 min running and was evaluated with Visual Analog Scale (VAS) 8/10. Compartment pressure measurements (using the Stryker Pressure Monitor) exhibited a major increase of pressure for both forefeet lateral compartment (Figure 4) from 12 mmHg at rest to 58 mmHg after 10 min of running. The diagnosis of chronic bilateral lateral compartment syndrome of the forefoot induced by exertion was asserted.

Compartment pressure measurements (in mmHg) for both forefeet lateral compartment before surgery. At rest (T0), at maximum pain (T1), 1 min (T2) to 3 min (T3) and 20 min (T4) after running stop.
After general information, patient’s consent was obtained and surgery was performed 1 month later.
Following an ultrasound-guided locoregional anaesthesia, the procedure was performed on both sides. Tourniquet on the legs was insufflated (for 25 min on the right side and 20 min on the left one), and the procedure was carried out through a dorsolateral approach of the lateral compartment. Firstly, the fascia of the Abductor digiti quint and Flexor digiti minimi muscles was completely split (Figure 5), and secondly these muscles were retracted to perform the fasciotomy of the lateral intermuscular septum. Finally, skin was directly sutured.
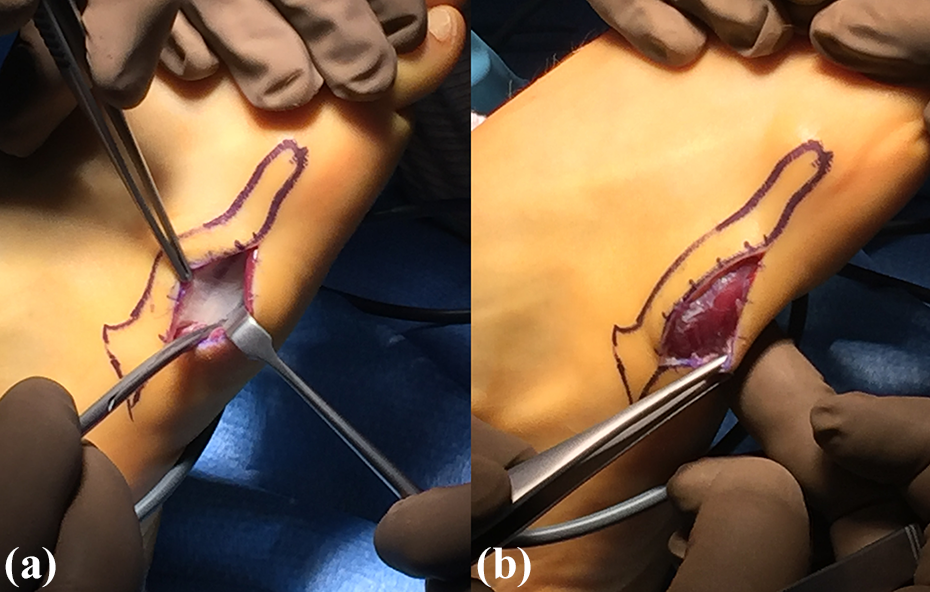
Peroperative views: (a) before and (b) splitting of the fascia of the abductor digiti quint and flexor digiti minimi muscles.
Postoperative care consisted in standard dressings, full-weight bearing, and rest. Exertion was prohibited for 1 month.
No complication occurred in the postoperative period. One month later, the patient started non micro-trauma activities and at 3 months, was able to run for nearly 1 hour without pain. At 6 months, he fully recovered and new compartment pressure measurements exhibited a decrease of more than 60% compared to preoperative measurements (around 22 mmHg after 10 min of running; Figure 6).
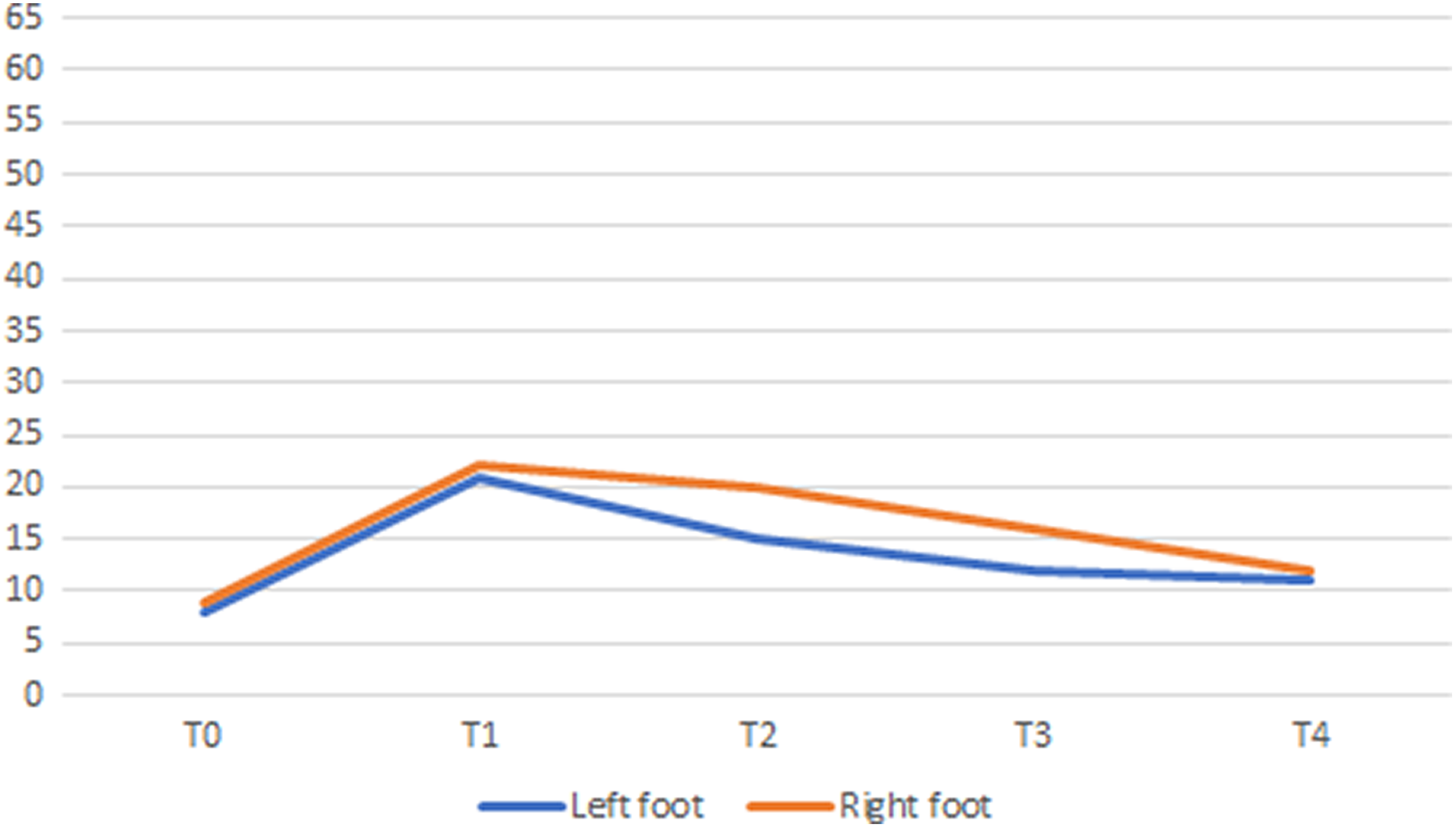
Compartment pressure measurements (in mmHg) for both forefeet lateral compartment after surgery. At rest (T0), at maximum pain (T1), 1 min (T2) to 3 min (T3) and 20 min (T4) after running stop.
Discussion
The clinical entity of chronic exertional compartment syndrome has been described for a long, but the pathophysiology remains unclear. 12 Different phenomena seem to be involved: increased muscle bulk, fascia thickness and stiffness, stimulation of fascial sensory stretch-receptors, poor venous return, micromuscular injuries, and small clinical myopathic abnormalities. The most affected compartment is the anterior compartment of the lower leg, 13,14 but there are also case reports and case series describing a chronic exertional compartment syndrome of the foot. 4 –9
The positive diagnosis is asserted on a body of evidence including: – systematic and reproducible exertion-related pain; – presence of risks factor such as sex (male), young age (20–25 years), active wealthy person (athlete), and microtrauma activities (running); – elimination of classic differential diagnosis like stress fracture (at least with X-rays); and – positive compartment pressure measurements during an exertional test. This method is considered as the gold standard, even if, since its first description in 1975,
15
no consensual criterion for interpretation have been established.
4
Medical treatment consisting in rest, ice, non-steroidal anti-inflammatory drugs and physiotherapy is known. Nevertheless, results are inconstant and usually inferior to surgical fasciotomy. Moreover, surgical treatment must be recommended if symptoms are recurrent because some cases of progression to acute syndrome leading to urgent surgery have been described. Today, the indication for fasciotomy should rely on either clinical symptoms or risk factors because no cut-off is known for pressure measurement in chronic syndrome. In acute syndrome, a differential pressure between compartment pressure and diastolic pressure of less than 30 mmHg is frequently chosen. 4,16
Conclusion
Chronic compartment syndrome is an underestimate aetiology for exertion-related pain in athletes. It must be evoked each time other diagnosis such as stress fracture is eliminated even if the location is uncommon. Compartment pressure measurements could be helpful to strengthen this diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.