
Abstract
Purpose:
Arthroplasty-related infection has grown worldwide. Revision procedures for infection are associated with longer operating time, superior amounts of blood loss, and substantial economic encumbrance. To overcome cost, many surgeons opt for hand-mixed vancomycin into the bone cement. The objective of this research was to assess the biomechanical strength and antibacterial properties of hand-mixed vancomycin bone cement at different concentrations with commonly used industrial preblended antibiotic bone cement and plain cement. The target was to determine the ideal concentration of antibiotics that can be used in the preparation of hand-mixed vancomycin cement that delivers maximum antibiotics concentration without compromising its biomechanical properties.
Materials and Methods:
Vancomycin-impregnated polymethyl methacrylate (PMMA) specimen was hand prepared in varying concentrations (1–4 g). The authors tested three-point bending strength to determine ‘maximum bending load’ and stiffness and its antibacterial activity by looking into the zone of inhibition on methicillin-resistant Staphylococcus aureus-impregnated agar plate. These were compared with the industrial preblended Simplex™ P with 1 g tobramycin.
Results:
This study exhibited that vancomycin-PMMA disk that contained higher concentration of antibiotics had significantly higher antibacterial activity. The control group (plain cement) and industrial PMMA with preblended antibiotic (tobramycin) showed stable mechanical strength, while the hand-mixed antibiotic cement (HMAC) had variable mechanical strength varying on the concentration of antibiotics used.
Conclusion:
It was effectively concluded that HMAC is advantageous as a cement spacer; however, it is not recommended for primary arthroplasty and second-stage revision arthroplasty. The recommended maximum concentration of vancomycin based on this study is 2 g/pack (40 g) of cement. Industrial preblended antibiotic cement is superior to hand-mixed cement.
Introduction
Arthroplasty-related infection (ARI) in orthopedic surgery is a solemn complication. Although its incidence over the years has dwindled due to modern theater facilities and aseptic measures, nonetheless, its prevalence remains high in developing countries. These infections impose detrimental morbidity to the patients, both financially and psychologically. Implant-related infections are among the most devastating complications for both the patient and the surgeon. 1
The economical impact accompanied by treating ARIs is substantial. Revision procedures in cases of infection are associated with longer operating time, greater blood loss, and frequent complications, along with prolonged duration of hospitalization, multiple operations, increased hospital costs, and outpatient visits and charges. 1
The most common microorganisms involved in ARI are coagulase-negative Staphylococcus and penicillin-sensitive Staphylococcus aureus. However, due to mishandling of antibiotics, these organisms have developed resistance. Pseudomonas aeroginosa and methicillin-resistant Staphylococcus aureus (MRSA) now impose as the principal hindrance in ARIs. 2 Thus, the practice of parenteral administration of vancomycin to treat ARI has gained acknowledgment. However, the systemic use of aminoglycoside is associated with various systemic adverse effects, such as ototoxicity, nephrotoxicity, and neuromuscular blockage.
In 1969, Buchholz et al. introduced a technique that used polymethyl methacrylate (PMMA) bone cement. Incorporated with gentamicin, it behaves as a local vehicle to deliver higher local concentration of antibiotic, therefore effectively eradicating infection in orthopedic surgery. 1 Palacos bone cement containing gentamicin powder was introduced as a commercial product in 1970. CMW® bone cement containing gentamicin was introduced in 1990. Surgical Simplex P, which contains tobramycin (Howmedical, UK), was commercially released in 2002.
The rationale behind antibiotic-loaded cement is the delivery of antibiotics to the local tissues at higher concentrations without instigating systemic toxicity and maintaining an elution profile that provides a constant level of antibiotics for an extended period of time. Studies with antibiotic-loaded PMMA have shown to provide 20 times the concentration of antibiotics locally compared with systemic administration. 3
The advantages of using antibiotic-loaded cement for patients with established prosthetic infection have been well sought into and documented in the literature. There can be a significant diminution in recurrent infection (from 28% to 5% of patients) and an improvement in outcome with the use of antibiotic cement for a one-stage exchange in cases of infected total knee 4 and revision hip arthroplasty. 5 However, adding antibiotics makes the biomechanical properties of PMMA weaker, but there are conflicting results on the optimum concentration that can be added. In one study, the addition of 2 g gentamicin, oxacillin, and cefazolin to 60 g of PMMA produced no statistically significant difference in terms of compressive and tensile strength. 5 Another study found a significant decrease in mechanical strength between 250 mg and 500 mg of gentamicin added to PMMA. 6 A need to investigate the optimum concentration of vancomycin to PMMA deems crucial.
Commercially available antibiotic cements are costly; therefore, hand-mixed antibiotic cement (HMAC) is commonly used especially with vancomycin, but the effectiveness and adequacy of the active antibiotic concentration and its biomechanical properties have always been a concern. The best antibiotic laden cement is one that provides eluted concentrations of the active drug well above the minimum inhibitory concentration (MIC) of the microorganisms involved in prosthetic joint infections and yet does not alter the mechanical properties of the bone cement. This article was aimed at determining the effectiveness of manually increasing the concentration of an active antibiotic (vancomycin) into PMMA bone cement, with regard to its biomechanical stability and antibacterial properties in cases of ARI and revision arthroplasty.
Materials and methods
The choice of PMMA bone cement in this study was Simplex P. It is relatively inexpensive and easily available. As for the choice of premixed antibiotic cement, we used Simplex™ P with tobramycin (containing 1 g of tobramycin). For the purpose of this study, we used vancomycin for the HMAC, as it is the most commonly used antibiotic in our institution against MRSA bone and soft tissue infections. To preclude discrepancy, the antibiotic adapted for this study was manufactured by the same company (Actavis™) and belonged to the same manufacturing batch.
Antibiotic cement preparation
All samples were prepared in the operating theater with temperature ranging from 18°C to 22°C and at atmospheric pressure. The primary investigator prepared all test specimens with the assistance of a nursing staff. The preparation was carried out in full sterile conditions. The aforementioned environment was chosen to emulate the actual surgical scenario as precisely as possible. An assistant maintaining sterility poured the relevant amount of crystallized vancomycin hydrochloride powder into the polyethylene mixing bowl. It was then stirred with polyethylene spatula to obtain uniformity of the antibiotic powder. The cement powder (40 g) was then poured into the same mixing bowl. The powder mixture was subsequently stirred to assure that both the cement powder and the antibiotic powder are mixed homogeneously. Lastly, 20 ml of liquid monomer was added and blended manually with a sturdy polyethylene spatula, for about 2 min in a polyethylene bowl. The concentrations of HMAC prepared were 1, 2, 3, and 4 g of vancomycin.
Preparation of the antibiotic pellets and cylinders
The resulting dough was then poured into a 50-cm3 medical syringe within the time frame of 3–8 min and then extruded into the mold. The molds for pellets were prepared from 5 cm3 medical-grade disposable hypodermic syringe barrel made from polypropylene (B Braun Omnifix® Solo, (B. Braun Melsungen AG)). The inner diameter of the syringe barrel was 12 mm (measured with a digital caliper). The syringe barrel was cut with a band saw cutting machine at the thickness of 5 mm (Figure 1). The ring-shaped molds were then fixed to a polyethylene plate, which served as the base for the mold. The final dimension of the mold was 12 mm in diameter and 5 mm in height. The cement was left inside the mold for 20 min. Upon hardening, the test specimens were gently pushed out using a plunger.
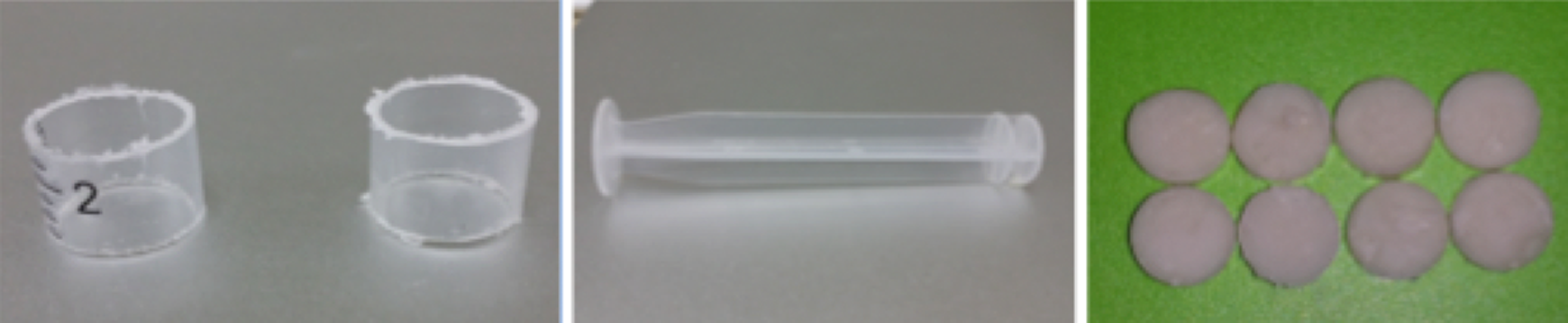
The molds used to make the PMMA disk, the syringe pusher used to deliver the cement disk out of the mold, and the final resulting cement disc are shown.
The molds for mechanical testing were prepared from 10 cm3 medical-grade disposable hypodermic syringe barrel that are made from polypropylene (B Braun Omnifix Solo; Figure 2). The inner diameter of the barrel was approximately 14.75 mm. The barrel was cut with a band saw cutting machine, which was adjusted to cut a cylindrical shape with a length of 50 mm (Figure 2). The cylindrical molds were then fixed to the polyethylene plate to serve as the base for the final specimen. The final dimension of the cylindrical mold was 14.75 mm in diameter and 50 mm in height. The plunger from the syringe was used as the pusher to dispense the test specimen out of the mold.

(Right) 10 cm3 syringe cut at both ends was used to make the molds for the biomechanical testing. (Left) The resulting PMMA specimens ready for biomechanical testing.
Polypropylene was utilized, as it is stable under conditions of shock, vibration, pressure, and temperature. The melting range of polypropylene is 130–167°C, which is above the maximum temperature recorded during PMMA polymerization, that is 110.2°C. 7
Plain Simplex P (SP0 V) and industrial preblended Simplex P with tobramycin (Stryker®, 1 g; SP1 T) were prepared in a similar fashion for comparison as control samples.
To ensure uniformity, all the samples prepared were weighted with a digital scale and those with a difference of more than 5% were discarded.
Mechanical testing
Static mechanical properties of PMMA bone cement were tested. The tests conducted with slowly loading weight onto the bone cement can derive static mechanical properties of the bone cement. These generally include ultimate strength, elastic limit in tension, compression, shear, torsion, and bending. For the purpose of this study, three-point bending was conducted. This test also indirectly measures shear force and stiffness (brittle).
Twelve sets of PMMA cylinder-shaped specimen for each group were prepared for three-point bending test, which were labeled accordingly (Figure 2). All mechanical testing were performed with the Instron® 3365 machine (Biomechanics Lab. National Orthopaedic Centre of Excellence for Research & Learning (NOCERAL), Department of Orthopaedic Surgery, University Malaya, Kuala Lumpur, Malaysia). The specimen was secured onto a jig attached at the base of the machine. The pointer jig was assembled to the 5-kN load cell (Figure 3). This process and sequence of measurements were done for a total of three cycles. The process was repeated with a gradual load increment until the specimen fractured (Figure 3). The load required to fracture the specimen was labeled as the “maximum bending load,” and stiffness was calculated with the Bluehill® 3 material testing software (Bluehill® 3 Universal. INSTRON © Illinois Tool Works Inc.). The dimensions of the testing segment were defined as the distance between two points on the holding jig. The measurement was 30 mm in length and 14.75 mm in diameter. A preload of 5 kN was applied to the specimen prior to formal loading with a crosshead rate of 5 mm min−1. Successively, the maximum three-point bending force that was exerted was 5 kN. The machine recorded the displacements detected on progressive load. Subsequently, the load to the specimen was released, and recalibration was done prior to the next loading with the same force.

(Right) The cylinder-shaped PMMA specimen was placed on the holding jig. Pointer jig was slowly loaded onto the specimen at crosshead rate of 5 mm min−1. (Left) Shows the resultant fractured cement cylinder.
Antibacterial activity
Bacterial strains used in this experiment were cultured from tissue samples taken from patients who had been admitted for MRSA implant infection in our institution. The following strains were studied: MRSA 0408-33 and 0702-10. The cement pellets were sterilized with ethylene oxide according to ISO 11135:1994 for medical devices. The zone of inhibition was tested with modified Kirby–Bauer test, also called disk diffusion test. In this test, MRSA was swabbed uniformly across a culture plate. PMMA disk (dimension: 5 mm in height and 12 mm in diameter) containing various concentrations of active vancomycin hydrochloride was placed on a Mueller-Hinton plate. The vancomycin-PMMA pellet, which contained a specified concentration of active vancomycin hydrochloride, was placed onto the inoculated plate and incubated at 35 ± 2°C. After 16–18 h of incubation, the plates were removed, and the zone of inhibition was measured. The results were interpreted according to the CLSI2013 guidelines.
The clear area surrounding the pellet demarcated the zone of inhibition of antibiotic-loaded PMMA, which represented the antibacterial activity. Scan® 500 inhibition zone reader (Interscience, France) was used to measure the zone of inhibition of the respective PMMA disks. The findings were recorded in millimeter (Figure 4).

Showing the zone of inhibition (right and left).
Statistical analysis
Using the analysis of variance, the mean maximum bending load, the stiffness of these PMMA specimen, and the zone of inhibition were analyzed and compared, where a p value of <0.05 was considered significant. The comparison of vancomycin concentration between the specimens was analyzed using Scheffe’s post hoc test. We also examined the relationship between the mechanical strength and the zone of inhibition with Pearson’s correlation test.
Results
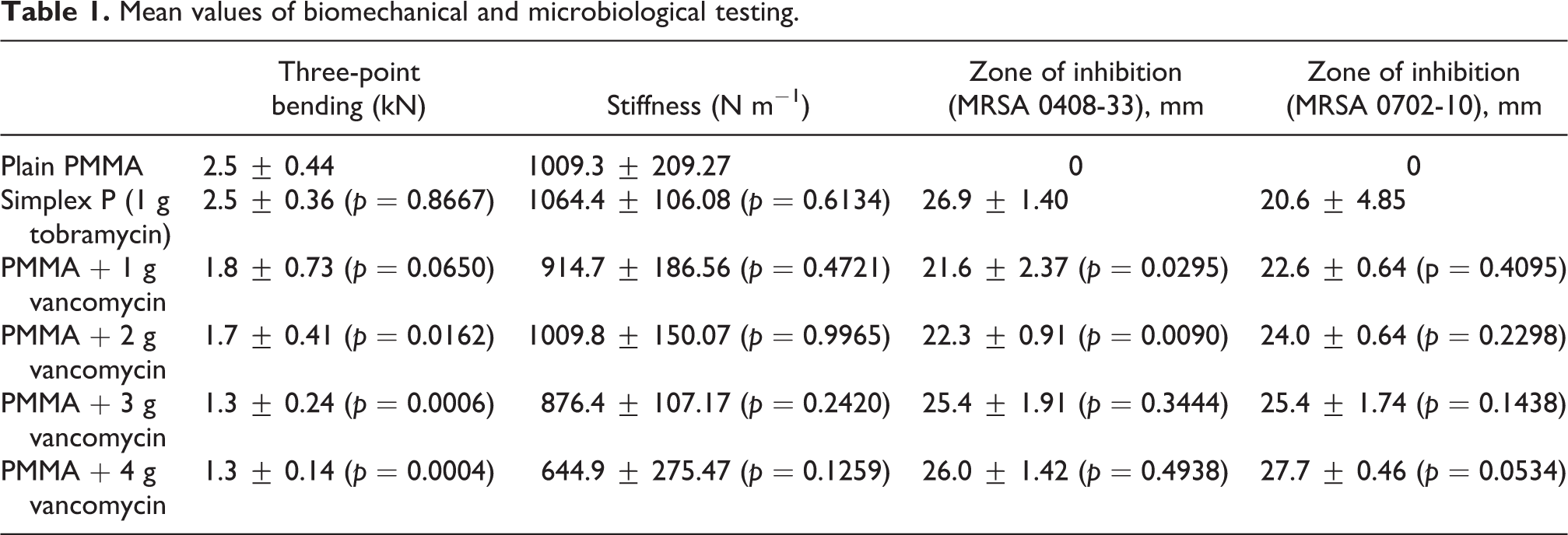
The results are summarized in Table 1.
Mean values of biomechanical and microbiological testing.
Three-point bending
The mean three-point bending of plain PMMA, vancomycin-PMMA, and tobramycin-PMMA is shown in Figure 5. There was no significant difference between the control group and Simplex P preblended with tobramycin (2.48 kN ± 0.36; p = 0.867). There was no significant difference between the control group and 1 g vancomycin (1.750 kN ± 0.73; p = 0.065). There was a significant difference with 2 g vancomycin (1.71 kN ± 0.41; p = 0.016), 3 g vancomycin (1.30 kN ± 0.30; p = 0.0006), and 4 g vancomycin (1.27 kN ± 0.14; p = 0.0004).

Mean three-point bending of plain PMMA, tobramycin-PMMA, and vancomycin-PMMA.
The significance of Simplex P with vancomycin is summarized in Table 2.
Significant difference between Simplex P® and different concentrations of vancomycin-PMMA.

Stiffness
There was no significant difference between the plain PMMA with Simplex P (1064.42 ± 106.08 N m−1; p = 0.6134), 1 g vancomycin (914.65 ± 186.56 N m−1; p = 0.472), 2 g vancomycin (1009.79 ± 150.07 N m−1; p = 0.997), 3 g vancomycin (876.41 ± 107.17 N m−1; p = 0.242), and 4 g vancomycin (744.93 ± 275.47 N m−1; p = 0.126), as shown in Figure 6.

Mean stiffness of plain PMMA, tobramycin-PMMA, and vancomycin-PMMA.
The significance of Simplex P with vancomycin is summarized in Table 3.
Significant difference between Simplex P® and different concentrations of vancomycin-PMMA.

Zone of inhibition
The zone of inhibition increased with increasing the amount of vancomycin added into PMMA, but they were smaller and irregular compared to the tobramycin-PMMA (Figure 7). Details of the result are summarized in Table 1.

Comparison of the mean zone of inhibition at plain PMMA, industrial premixed antibiotic PMMA, and increasing concentration of manual hand-mixed vancomycin-PMMA.
Discussion
Antibiotic-impregnated PMMA functions as a vehicle to deliver high local concentration of active antibiotic at the site of infection without increasing the risk of unwanted systemic adverse reactions. However, only heat-stable antibiotics such as glycopeptides, aminoglycosides, penicillin G, and cephalosporins are suitable for antibiotic cement spacers. 7
We hypothesized that the addition of antibiotics will significantly reduce the biomechanical strengh of the cement compared to plain Simplex P and commercially available Simplex P with preblended tobramycin. The comparison was made at different concentrations of vancomycin, and it showed that the addition of 3 g or more of vancomycin significantly weakens the three-point bending strength of PMMA. Similar results were reported in literature. 8,9
Stiffness of the control group and Simplex P preblended with tobramycin was comparable to 5% differences. With the addition of 1 g of vancomycin, its stiffness is reduced by 10%. With the addition of 4 g of vancomycin, it lost approximately one-third (36.1%) of its stiffness as compared to the control group. This was similarly observed in maximum three-point bending test. In fact, different antibiotics may have different effects on the bone cement behaviors, as there is a difference in terms of molecular weight. Vancomycin has a higher molecular weight compared to other aminoglycosides, such as gentamicin and tobramycin, 9 and its particles are much larger than other commonly used antibiotics. 10 Hence, the antibiotic powder could exist as an inclusion in the cement and might act as a stress riser to weaken the biomechanical properties of bone cement. 11
Our findings confirm that the addition of antibiotic affects the mechanical behavior of bone cements. Having said the aforementioned, we discovered no statistically significant reduction in the mechanical component of cement added with 1 g of vancomycin as compared to the plain cement. However, the addition of 2 g of vancomycin showed significant reduction of bending strength compared to plain cement and tobramycin cement. This is coherent with other published studies 9,12 showing that the addition of 5% vancomycin is safe. 13 –15
Both vancomycin HMAC and commercially manufactured tobramycin cement showed acceptable zone of inhibition against MRSA. The diameter of the zone of inhibition depended upon the sensitivity of the bacteria to the antibiotic-PMMA pellets and the point at which MIC was achieved. 16
In this study, we observed that the zone of inhibition produced by HMAC with vancomycin was smaller and irregular as compared to tobramycin cement. This observation was similar to what was published by Ferraris et al. 17 The mean zone of inhibition of tobramycin cement was higher than most of the HMAC with vancomycin and comparable to the HMAC with 4 g of vancomycin for MRSA Strain 0408-33. This difference may be due to higher susceptibility of this strain toward tobramycin and smaller molecular weight of tobramycin that eluted at a faster rate compared to vancomycin. For MRSA Strain 0702-10, the zone of inhibition of tobramycin cement was actually lower than HMAC with 1 g of vancomycin. Based on this observation, it can be concluded that different antibiotics may be more bactericidal toward certain strains of MRSA.
There are three major factors that should be considered when using antibiotic-loaded PMMA in patients: first, whether the purpose of using antibiotic-PMMA is serving as an antibiotic spacer or part of a definitive implant fixation; Second is the commercially preblended antibiotic-PMMA available for the isolated organism; and third is the amount of antibiotic that can be added into the plain cement without significantly lowering biomechanical properties.
In this study, we found that higher the concentration of antibiotic loaded into PMMA, higher the degree of antibacterial activity. However, the mechanical strength of this PMMA was inconsistent and unpredictable, despite the meticulous preparation of the cement to minimize variability. There was variability even within the same group of HMAC. Thus, the use of HMAC with the purpose of providing mechanical strength in cases of primary and revision arthroplasty can give rise to an unpredictable outcome and therefore should be avoided.
It should be limited for cases of infected arthroplasty requiring an antibiotic cement spacer, such as stage 1 revision arthroplasty for a two-staged revision process. Based on the results of this study, the maximum amount of vancomycin that can be added into each pack of cement was 2 g. An addition of 3 g or more considerably weakens the mechanical strength of the cement without a significant improvement in the antibacterial activity. Our current recommendation on dosage and type of antibiotic was based on in vitro study, which coincides with other published data. 18
The industrial preblended antibiotic bone cement (PMMA with tobramycin), exhibited analogous mechanical strength with plain PMMA while maintaining a significant antibacterial activity. In cases where both optimum mechanical strength and antibacterial property are required, industrial preblended antibiotic PMMA is recommended, such as in primary and stage 2 of the two-staged revision arthroplasty.
We recommend the use of HMAC with vancomycin as local antibiotic therapy in the case of ARI, where mechanical strength is not required, for example, cement spacer or cement beads at the site of infection to deliver higher concentration of antibiotics locally. This technique would definitely be effective for local delivery of antibiotics and is economical. It can also be used in other cases of orthopedic infection, where transitory mechanical support is necessitated, for example, antibiotic cement rod insertion for cases of infected intramedullary devices in long bones.
The limitations of this study were as follows: The study did not address other biomechanical properties such as compression and fatigue strength due to the limitation of facilities available and financial constraints. The elution properties of HMAC combinations were not tested. A more accurate method of quality control was adapted by Lewis and Janna, where all the specimen in their study was subjected to radiological testing for internal and external flaws and discarded all those with porosity greater than 0.5 mm. 19 Again because of budget, this study only weighed the test specimens and discarded those with 5% and more difference to ensure standardization. This may elucidate the outliers and inconsistency in data.
Conclusion
Hand-mixing vancomycin to PMMA significantly alters the biomechanical property compared to industrially blended antibiotic-PMMA. Therefore, it is not recommended for use in cases of primary and secondary stage of two-staged revision arthroplasty. It can be utilized as a temporary cement spacer for infective cases to deliver higher concentrations of local antibiotic.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.