
Abstract
We evaluated the long-term functional and cosmetic results of homodigital neurovascular island flap (NIF) used to reconstruct extensive pulp defects with bone exposure in children. Twenty-three children (mean age 4.8 years, range 1–10 years) with fingertip injuries were reconstructed with a pedicled homodigital NIF and evaluated in terms of sensation quality, cold intolerance, scar formation, nail deformity, range of motion and overall finger length at a mean follow up of 7.8 years (range 2–13). Eleven patients reported cold sensitivity in the operated fingertip, and 15 presented with hook nail deformities at the final follow-up. The total active motion of the injured finger was significantly lower than that of the uninjured side (p < 0.001). NIFs is a safe, reliable reconstructive treatment for fingertip loss in children, but commonly encountered issues in the long term include an extension lag of the interphalangeal joints, hook nail deformities and cold intolerance.
Introduction
Fingertip injuries are extremely common in children (Kubus et al., 2011; Macgregor and Hiscox, 1999). The majority of these can be treated conservatively by conventional semi-occlusive dressings or silicone finger caps with excellent results (Georgoulis et al., 2021; Hoigne et al., 2014; Schultz et al., 2018). However, about 25% of these injuries are reported to be more severe and necessitate surgical treatment (Macgregor and Hiscox, 1999; Schultz et al., 2018). These are usually characterized by severe soft tissue loss with exposed bone, requiring soft tissue coverage in order to provide reliable wound healing and the prevention of osteomyelitis. Distal fingertip replantation may confer the best results in more proximal amputations if technically possible but if not, composite grafting may be considered (Dubert et al., 1997). When the distal part is missing, flap reconstruction with a V-Y advancement flap can be an option for limited soft tissue loss, however, a pedicled flap may be necessary in more extensive defects (Haehnel et al., 2019; Usami et al., 2015).
The homodigital neurovascular island flap (NIF) is an established local flap used especially for volar oblique pulp loss exceeding 1 cm in diameter with exposed bone (Kayalar et al., 2011). It is relatively simple to harvest with several theoretical advantages, including reconstruction of lost pulp using similar tissues, retained sensibility and minimal donor-site morbidity (Adani et al., 1997; Varitimidis et al., 2005; Venkataswami and Subramanian, 1980). Although its application and long-term results in adults have previously been reported in several articles, the outcomes of this flap in children have not been studied extensively, with only a single article in the literature favouring its use in pulp defects (Wang et al., 2011).
The aim of this study was to evaluate the long-term functional and cosmetic results of homodigital direct flow NIF used to reconstruct extensive pulp defects with exposed bone in children.
Methods
Patient assessment
This is a retrospective case series involving children whose fingertip loss was reconstructed with a pedicled homodigital NIF. The study was approved by the institutional review board of the hospital, where all the patients were treated. Exclusion criteria included patients older than 12 years of age at the time of operation, patients with multiple finger injuries, cases with less than 2 years follow-up and those who had an injury or operation of the same finger on the contralateral hand.
A standardized evaluation protocol was applied to all patients during the last follow-up. Demographic data, including age at the time of operation, sex, operated finger and follow-up time of the patients, were recorded. The initial and current radiographs and operative pictures were reviewed in order to classify injuries according to Ishikawa’s classification of subzones and to determine the exact flap size (Evans and Bernardis, 2000). An independent observer (T.Y.), who is an orthopaedic surgeon with 4 years of experience in hand surgery and not part of the operative team, assessed the aesthetic and functional results of the operated fingers. The reconstructed pulp was evaluated for atrophy, sensation quality, cold intolerance, scar formation, nail deformity and overall aesthetic appearance. The sensitivity of the reconstructed pulp was assessed using Weber’s static two-point discrimination test (s-2PD) (Baseline Dellon 2-Point Disk-Criminator, NY, USA) and the Semmes–Weinstein monofilament (SWM) test (Baseline Tactile monofilament, 6-piece Set, NY, USA). Hook nail deformity was classified using the Lim classification (Lim et al., 2008) (Figure 1). An 11-point rating scale (0 = extremely dissatisfied, 10 = extremely satisfied) was used to evaluate overall patient satisfaction (Arsalan-Werner et al., 2019).
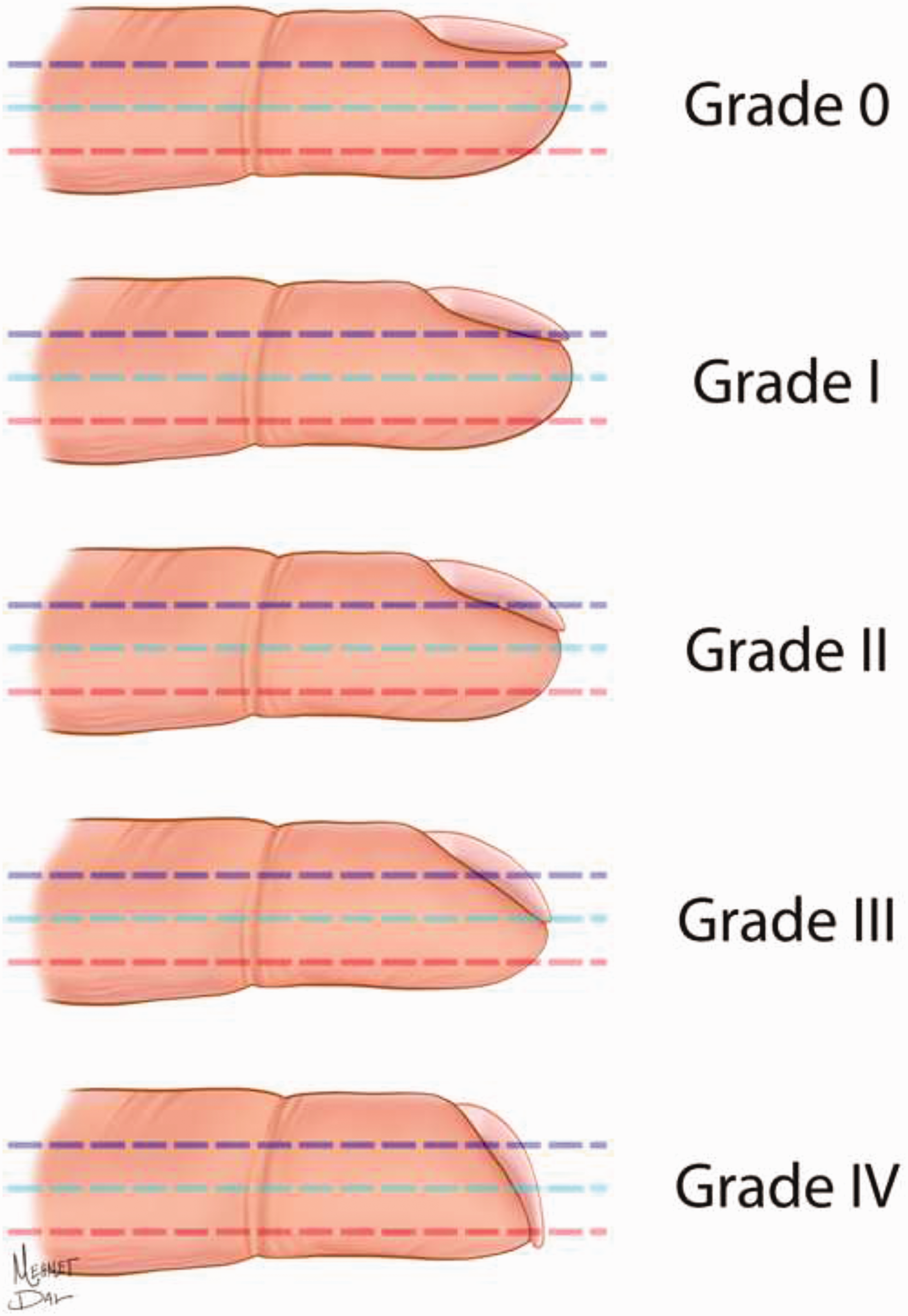
Lim’s classification for degree of hook nail deformity (Lim et al., 2008).
The operated finger was also evaluated for general atrophy, sensation quality on the donor half and active range of motion of the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints of the fingers, as well as the MCP and interphalangeal (IP) joints of the thumbs, which were measured with a handheld goniometer (Jamar Stainless Steel Finger Goniometer, Pakistan). The total active motion (TAM) of the operated fingers was then calculated using Strickland’s method, in which TAM equals the combined active flexion minus the combined extension deficit of the joints (Strickland and Glogovac, 1980). The distal phalanx length of the operated side was measured radiologically and compared with the same finger on the opposite hand in order to detect any initial bone loss effects on the hook nail deformity formation. The middle and proximal phalanx lengths of the operated fingers and proximal phalanx length of the operated thumbs were also measured radiologically and compared with the uninjured contralateral finger and thumb, respectively, to detect any general finger atrophy due to the sacrifice of one of the two neurovascular bundles during flap elevation.
Surgical technique
All operations were performed under general anaesthesia, with a pneumatic tourniquet and loupe magnification. Following debridement of the wound, the size of the flap was determined and marked on the donor site, which was located just proximal to the defect. Visualization of the integrity and quality of the neurovascular bundle were always performed prior to flap elevation. A volar lateral zig-zag incision was preferred for preserving postoperative joint motion. The flap was designed in a triangular shape with the tip facing proximally, never extending beyond the proximal IP joint crease (Figure 2(a)). Distally, the dimensions of the flap were extended to the entire width of the defect (Ventakaswarmi and Subramanian, 1980). The neurovascular bundle was freed up to the MCP joint crease with a cuff of soft tissues around it in order to preserve the venous inflow (Figure 2(b)). After dissection, the elevated flap was advanced distally to cover the exposed bone, and the distal end of the flap was sutured to the nail matrix (Figure 2(c)). Care was taken to limit excessive traction of the pedicle, and the finger was brought to full extension before suturing the distal end of the flap to the nail matrix in order to ensure there was no limitation on finger extension. The donor site was primarily closed in all cases.
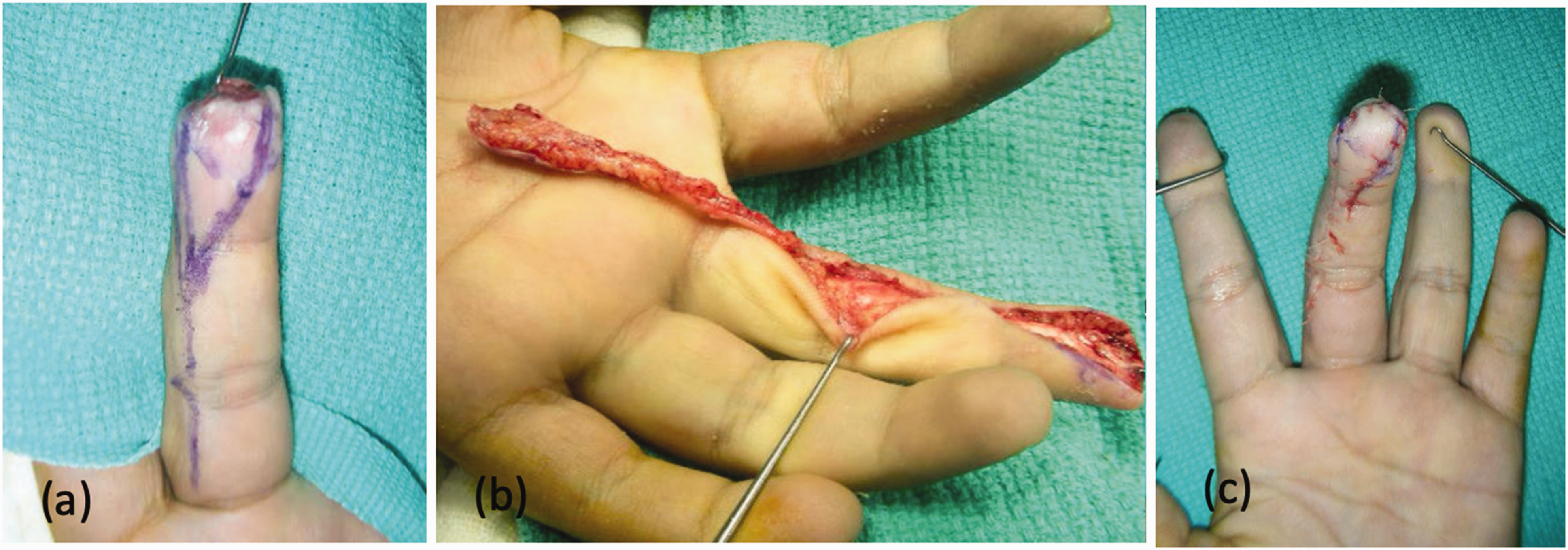
The preoperative (a), intraoperative (b) and early postoperative (c) pictures of a patient with a fingertip injury with exposed distal phalanx and intact nail matrix.
Statistical analysis
Shapiro–Wilk test was used to assess normality assumptions of continuous variables. For continuous variables, bivariate analysis was performed using the Mann–Whitney U test and Wilcoxon signed-rank test depending on the normality of distribution. Software was used for analysis, and p-values of less than 0.05 were considered significant.
Results
Between 2005 and 2018, 36 children received the NIF for fingertip reconstruction in our hospital and 28 met the above-mentioned evaluation criteria. Among these, 23 patients consented to participate in this study and were seen in the hospital for a final evaluation. The patients were operated on by a team of hand surgeons with Level 4 expertise (Tang and Giddins, 2016). All patients were evaluated at a mean follow-up time of 7.8 years (range 2–13) postoperatively (Supplementary Table S1). The mean age at the time of operation was 4.8 years (range 1–10). The index finger was the most frequently affected, followed by the middle finger, the thumb, the ring finger and the little finger. The most commonly injured zone was Ishikawa Subzone II.
Partial or total flap necrosis, infection at the exposed distal phalanx or evident atrophy of the flap were not observed in any patient (Figure 3(a)). Three patients were able to feel the 3.61 monofilament (diminished light touch), and 20 patients were able to feel the 2.83 monofilament (normal) at the reconstructed fingertip. Two-point discrimination was less than 3 mm in 17 patients and between 3–6 mm in six patients. Eleven patients reported cold sensitivity at the operated fingertip. Additionally, another 11 patients experienced scar formation at the surgical site, which did not cause pain or functional limitations to the operated finger.
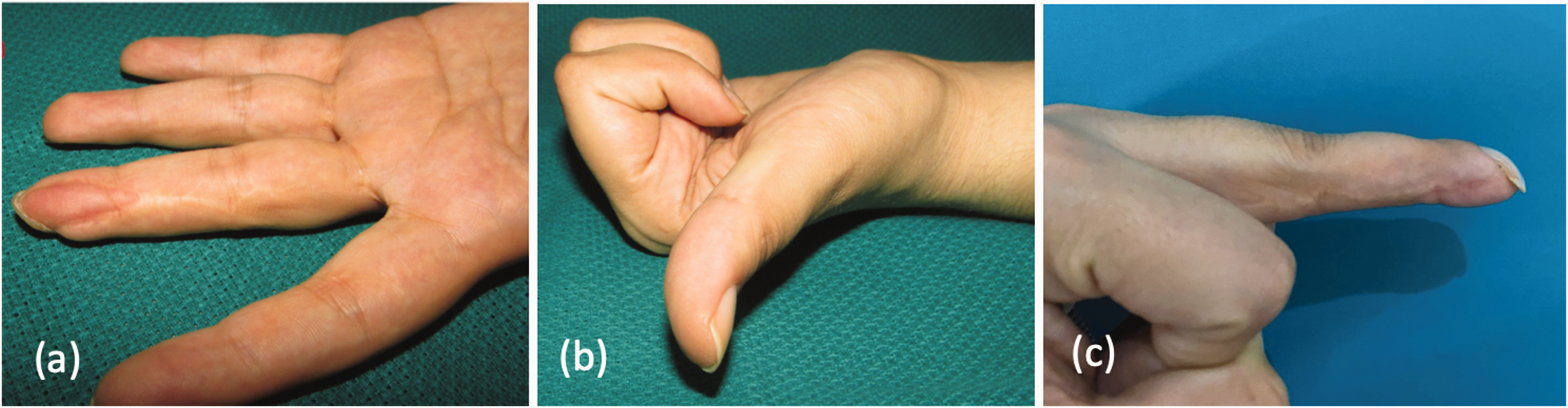
Photographs taken in the third postoperative year showed no atrophy at the reconstructed pulp (a), no limitation of flexion and extension (b) but a hook nail deformity of the fingernail (c).
In total, 15 of 23 fingers showed a hook nail deformity at final follow-up; according to the Lim classification: three fingers showed Grade 4 beaking, four fingers showed Grade 3 beaking, three fingers showed Grade 2 beaking and five fingers showed Grade 1 beaking. The appearance of the reconstructed pulp was rated as normal in 17 children and flat and atrophic in six children. The average patient satisfaction was found to be 6.7 (range 3–9) on an 11-point rating scale.
There was no reduced sensation in the donor half of the finger at the last follow-up, and no visible atrophy was detected on the operated finger in any of the patients when assessed radiologically. The mean distal phalangeal lengths of the operated and uninjured contralateral hand were 10.1 mm (range 3–18) and 13.5 mm (range 11–20), respectively. There was no significant correlation between the amount of shortening of the distal phalanx and the grade of hook nail deformity (p > 0.05). Also, the final length of the middle and proximal phalanges of the operated and contralateral fingers/thumbs did not demonstrate any significant difference (p > 0.05).
Thirteen patients exhibited minor flexion contractures of the involved finger joints, which did not limit hand function. None of the patients exhibited limitations of flexion in any joints of the operated fingers (Figure 3(b) and (c)). There was no statistically significant correlation between scar formation at the operation site and the TAM results for the operated finger (p > 0.05). However, the Wilcoxon signed-rank test revealed that the TAM of the injured finger was significantly lower than that of the uninjured hand in all patients (p < 0.001).
Discussion
In this study, we demonstrated that the NIF is a safe, reliable flap for children with fingertip defects where cover of exposed bone is necessary. We experienced no partial/total necrosis or any distinct atrophy of the flap in the longer term. Near normal sensation was achieved in all reconstructed fingertips, which is rated as ‘excellent’ according to the modified American Society for Surgery of the Hand guidelines for the stratification of 2PD (Mermans et al., 2012). A long-segment neurovascular pedicle dissection and NIF harvesting in paediatric patients did not cause an adverse effect on the growth of the operated fingers and phalangeal bones. Harvesting one of the two main arteries of a growing finger with the flap did not cause any apparent soft tissue atrophy and stripping one of the two digital nerves also does not seem to diminish the quality of sensation on the donor side of the finger. However, 47% of our patients reported cold intolerance, revealing that nerve healing may be incomplete even in young children.
Surgeons may differ in their indications for flap reconstruction of fingertip injuries. It has been shown that when treated with semi-occlusive dressings, human fingertips are able to regenerate soft tissue and skin following amputation injuries with excellent cosmetic and functional results with no reported joint stiffness (Georgoulis et al., 2021; Hoigne et al., 2014; Schultz et al., 2018). As a result, conservative treatment should be the first choice in the majority of fingertip amputations in children and even in adults (Allen, 1980; Krauss and Lalonde, 2014). However, when the defect is extensive and bone is exposed, a local flap may be an alternative for covering up the exposed bone end without shortening. This practice not only preserves the length of the bone and nail bed, but also shortens healing time, restores fingertip sensation and lessens the risk of osteomyelitis (Kayalar et al., 2011).
It has been reported that fingertip injury reconstruction in children with an extensive soft tissue defect remains a challenge for surgeons due to the smaller size of the fingers, making pedicle dissection and flap elevation more difficult and demanding (Das and Brown, 1978; Ljungberg et al., 2003). Among the numerous flap options for coverage of fingertip injuries, the best surgical results are reported from V-Y advancement flaps (Ma et al., 1982). When the defect is large and beyond the reach of this flap, a homodigital pedicled advancement flap becomes a better option. While reverse flow variants of homodigital flaps have been reported with excellent results in adults, these flaps necessitate a more detailed dissection and are harder to perform in children (Niranjan and Armstrong, 1994). Finally, although there are more straightforward procedures, such as thenar flap or cross finger flap, that avoid microdissection, these require longer immobilization time of the hand and the need for multiple surgeries, thereby decreasing their popularity for use in small children (Barr et al., 2014; Fitoussi et al., 2004).
The NIF remains a good option for reconstructing large pulp defects with exposed bone in children as a one-stage operation and does not necessitate prolonged immobilization of the injured finger. Wang et al. (2011) reported satisfactory results with the use of NIF in children, stating that normal sensation and motion were achieved in all patients, with no reported cold intolerance. The authors attributed these superior results, when compared with adult reconstructions, to children’s increased capacity for healing and regeneration. However, their patient group was limited to 11 cases, and follow-up time was only 15 months on average, meaning that evaluation was performed prior to finger maturation in all of their cases. We aimed to evaluate a larger group of patients with a longer follow-up period of 7.8 years on average, where finger growth had ceased in most patients. This may be a reason for the difference in results that were reported in this study.
Hook nail deformity seems to be a frequently encountered complication, impairing the aesthetic results of paediatric fingertip reconstructions (Varitimidis et al., 2005), with an incidence of 7–50% in adults (Arsalan-Werner et al., 2019; Kayalar et al., 2011). Our study revealed that this problem is more common in paediatric patients, which does not seem to be related to the amount of bone loss supporting the nail bed. Lim et al. (2008) suggested that nail beaking in reconstructed fingertips might worsen over time due to chronic flap contraction and the remodelling of soft tissues, even if the initial results were satisfactory. Also, as the finger grows longitudinally in children, the flap pedicle may not elongate as much and becomes tethered, pulling the flap and nail bed in a palmar and proximal direction, and this tethering may explain the increased incidence of beaking of the nail bed in children. Since the main complaint of patients enrolled in this study was the deformity of their nails, aesthetic results of this flap in children may not satisfy the majority of patients in the long term.
Restoration of unrestricted motion without contractures is essential in the treatment of fingertip injuries at all ages. While 13 out of 23 cases (56%) in this series showed an extension loss (10°–20°) of the involved finger joints, active and passive flexion was full in all cases. The extensor lag may again be related to the tethering effect of the flap pedicle and the surrounding scar tissues in a growing finger, resulting in impending soft tissue contracture on the palmar aspect of the digit. If a decision is made to reconstruct a finger with a NIF in children, parents should be informed about the long-term complications of this flap preoperatively.
The major limitations of our study were its retrospective design and small sample size. Additionally, we did not perform a comparison of flap coverage with conservative treatment of fingertip loss, which have been considered a reliable option in children. Further large-scale, prospective, randomized studies are needed to define the most appropriate treatment for these injuries.
In conclusion, NIFs is a safe and reliable flap for reconstruction of fingertip loss in children, although there are long-term complications a slight loss of terminal extension, formation of a hook nail deformity and cold intolerance.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934221108470 - Supplemental material for Long-term outcomes of homodigital neurovascular island flap reconstruction of fingertip injuries in children
Supplemental material, sj-pdf-1-jhs-10.1177_17531934221108470 for Long-term outcomes of homodigital neurovascular island flap reconstruction of fingertip injuries in children by Tugrul Yildirim, Ozgun Baris Gunturk, Kubilay Erol and Tulgar Toros in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the representatives of patients for their anonymized information to be published in this article.
Ethical approval
Ethical approval to report these cases was obtained from Hand Microsurgery Orthopedics Traumatology Hospital Ethics Committee (2021/02).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.