
Abstract
Background:
The main purposes of this study were to assess the levels of parenting stress in the mothers of children with congenital hand or foot differences and to evaluate the effects of this stress on the preferred roles of mothers in surgical decision-making for their children.
Methods:
This study included 89 mothers of children with polydactyly of the hand, polydactyly of the foot, a hypoplastic thumb, or macrodactyly. The parenting stress level was assessed using the Parenting Stress Index–Short Form (PSI-SF). Additionally, the mothers were requested to indicate their preferred and retrospectively perceived levels of involvement in surgical decision-making for their children using the Control Preferences Scale, which is comprised of five levels ranging from fully active to fully passive.
Results:
The average PSI-SF scores were 73.9, and 15 mothers (17%) had a clinically significant level of stress (PSI-SF ≥ 90). In the mothers of children with polydactyly of the foot, the PSI score was associated with the preferred role in surgical decision-making.
Conclusion:
The assessment of parenting stress levels in the mothers of children with congenital hand or foot differences can play an important role in the screening of candidates who require psychiatric treatment or support. An evaluation of the PSI in mothers of children with congenital hand or foot differences may aid physicians to modify their style of decision-making based on the preferred role of the mother.
Introduction
Parenting an infant with a congenital anomaly can be burdensome and stressful. In addition to the usual caretaking tasks, parents must handle their disrupted expectation of having a healthy baby. 1 Drotar et al. suggested that there are five stages of parental reactions to the birth of a child with a congenital malformation: shock, denial, sadness and anger, adaptation, and reorganization. 2 These authors also pointed out that early crisis counseling during the first months of life may be particularly crucial for parental attachment and adjustment. Several studies have investigated the parenting stress levels in the mothers of children with congenital heart disease, a cleft lip or palate, a urogenital anomaly, or a syndromic disease, 3 –7 but no studies have evaluated parental stress in the mothers of children with congenital hand or foot differences.
Parental stress can be defined as the perceptions of a parent regarding access to available resources to meet the demands of parenthood relative to the perceived demands of the parenting role, that is, when expectations do not match the perceptions of available resources. 8 One of the most common measures used to assess parenting stress levels is the Parenting Stress Index (PSI), which is a 120-item parent-reported questionnaire. 9 To reduce the cumbersome nature of the full-length PSI, the PSI-Short Form (PSI-SF) was developed; this measure consists of 36 items taken from the full PSI, which are categorized into three subscales: Parental Distress (PD), Parent–Child Dysfunctional Interaction (PCDI), and Difficult Child (DC). Each subscale consists of 12 items rated on a five-point scale, with the total stress score ranging from 36 to 180, where higher scores indicate higher stress associated with the parenting role. A total raw stress score >90 (≥90th percentile) indicates a clinically significant level of stress.
Parents of children who receive a new diagnosis of cancer or other life-threatening illness report emotional and psychological stress that interferes with decision-making. 10,11 Similarly, the parenting stress of mothers of children with a congenital hand or foot difference may influence their role in surgical decision-making to varying degrees. There are three styles of decision-making in clinical care: paternalism, shared decision-making, and consumerism (or informed). 12 In the paternalistic approach, the physician assumes the responsibility of the clinical decision with no or very little joint deliberation between the physician and the patient. 13,14 In the consumerist approach, the informed medical decision is made by the patient and others such as family members, after obtaining all necessary medical information pertinent to making an appropriate decision. 15,16 Shared decision-making is a combination of these two styles.
In this study, we evaluated the level of parenting stress among mothers of children with a congenital hand or foot difference using the PSI-SF. We also investigated their preferred and retrospectively perceived levels of involvement during surgical decision-making for their children. The purposes of this study are to evaluate the stress levels of mothers of children with a congenital hand or foot difference and to assess their effects on the surgical decision-making for their children.
Materials and methods
The present study received institutional review board approval. Mothers whose children had congenital hand or foot differences and underwent surgical treatments were recruited between January 2015 and December 2016. The levels of parenting stress in the mothers and their preferred and retrospectively perceived roles in decision-making for the surgical treatment of their children were investigated using standardized questionnaires.
Because parenting stress differs between mothers and fathers, 17 only the parenting stress of the mothers was focused on in the present study. The study inclusion criteria were as follows: (1) mothers whose children had polydactyly of the hand, polydactyly of the foot, a hypoplastic thumb, or macrodactyly and underwent surgical treatments and (2) mothers who agreed to participate in the study. The mothers of children with these four conditions (polydactyly of the hand, polydactyly of the foot, a hypoplastic thumb, or macrodactyly) were assessed for the present study, because they are relatively common diagnoses that require surgical treatment at our institute. The study exclusion criteria were as follows: (1) mothers whose children had congenital hand or foot differences other than the abovementioned four disorders and (2) mothers whose children had more than two comorbid diseases from among the four disorders. Although there are many types of congenital hand and foot differences, the diagnoses of the children were limited to polydactyly of the hand, polydactyly of the foot, a hypoplastic thumb, and macrodactyly. Ultimately, the present study included 89 mothers of children with these conditions (Table 1).
Scores for parenting stress and the proportions of mothers with clinically significant level of parenting stress.
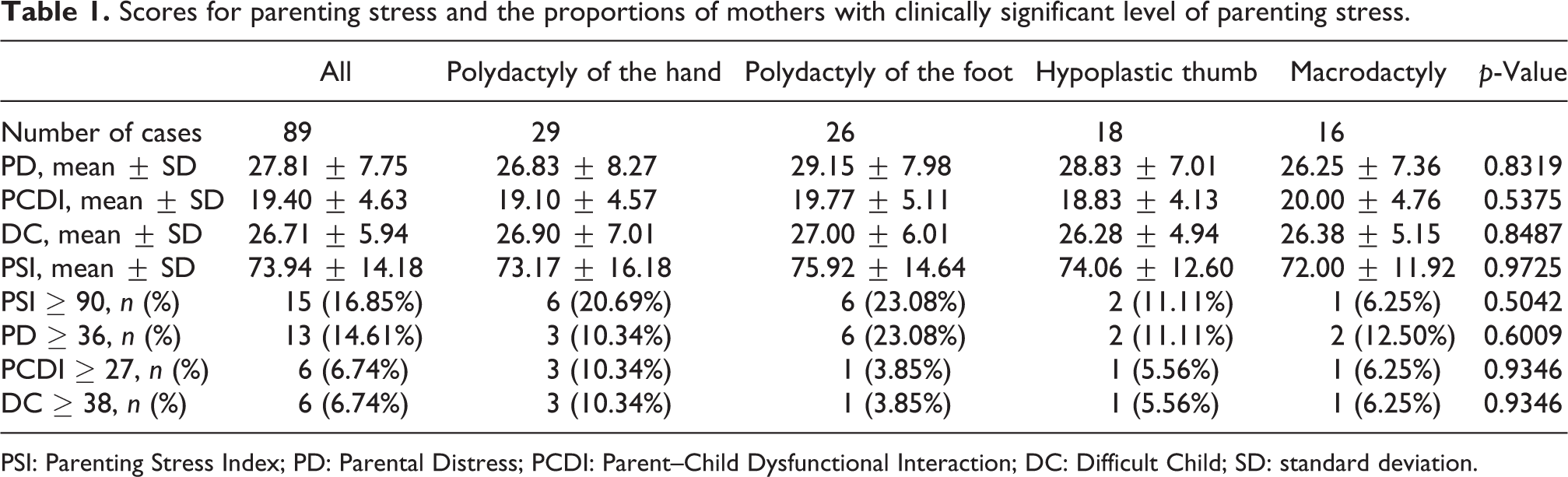
PSI: Parenting Stress Index; PD: Parental Distress; PCDI: Parent–Child Dysfunctional Interaction; DC: Difficult Child; SD: standard deviation.
Following the diagnosis of a congenital hand or foot difference that required surgical treatment, the parents received an explanation about the possible surgical options, surgical procedures, outcomes, and complications of each treatment in an outpatient clinic. Subsequently, the final treatment decision was made together with the parents. Most children were admitted to our hospital 1 day prior to surgery and discharged 2 days after surgery. Following the admission of each child to our hospital, their demographic data were obtained (Table 2). Additionally, 2 weeks after surgery, the mothers’ levels of parenting stress were assessed using the PSI-SF, and their preferred and retrospectively perceived levels of involvement in surgical decision-making were determined using the Control Preference Scale in the outpatient clinic. 18 The Control Preference Scale consists of five items that portray different roles in decision-making, ranging from a fully active to a fully passive role. The demographic data of the mothers, including age, education level, holding private insurance, and fear of burden imposed by medical costs, were also obtained (Table 2).
Demographic data of the children and mothers.

SD: standard deviation.
Statistical analysis
One-way analysis of variance was performed to compare the scores on the PSI-SF and its subscales (PD, PCDI, and DC) among the mothers whose children had polydactyly of the hand, polydactyly of the foot, a hypoplastic thumb, or macrodactyly, and χ 2 test or Fisher’s exact test was conducted to compare the proportions of mothers with significantly high levels of stress among the four subgroups. The degree of agreement between the mothers’ preferred and retrospectively perceived levels of involvement in surgical decision-making was assessed using weighted κ statistic. The influence of the PSI on the preferred role in surgical decision-making was assessed using Spearman’s correlation tests, and these correlations were analyzed according to the four subgroups.
The factors associated with the preferred roles of the mother in surgical decision-making for their children were assessed using logistic regression analyses. Because most mothers in the present study preferred their role to be semi-active or collaborative, the outcome variables were defined as active roles (fully active or semi-active) or non-active roles (collaborative, semi-passive, or fully passive). The factors associated with the level of parenting stress were assessed using logistic regression analyses, with the outcome variable defined as a PSI score >89.
Prediction models for the five levels of involvement of the mothers in surgical decision-making were constructed from the classification and regression tree, which is an easy to interpret nonparametric tree-building technique (based on recursive partitioning) used to stratify study populations, where the Gini index is a measure of impurity of attributes toward class distributions in splits. To prevent overfitting, threefold cross-validation was carried out repeatedly (100 times), and optimal model was chosen with minimum average rates of misclassification error for decision-making. Additionally, prediction models were constructed after defining the mothers’ preferred roles as outcome variables: active (fully active or semi-active) or not active (collaborative, semi-passive, or fully passive).
Results
The average PSI score was 73.9 (range: 50–111), and the average PD, PCDI, and DC scores were 27.8 (range: 13–48), 19.4 (range: 14–38), and 26.7 (range: 18–44), respectively (Table 1). There were no significant differences in the PSI score among mothers whose children had polydactyly of the hand, polydactyly of the foot, a hypoplastic thumb, or macrodactyly. Of the 89 mothers, 15 (16.9%) had clinically significant levels of stress (PSI ≥ 90); however, there were no significant differences in the proportions of mothers with clinically significant stress among the four subgroups of disorders in the children. Additionally, although there was significant consistency between the mothers’ preferred and retrospectively perceived levels of involvement in surgical decision-making (Table 3), the mothers of children with a hypoplastic thumb did not exhibit consistency in this regard.
Congruency between the preferred role and the retrospectively perceived role of mothers of children with congenital hand or foot differences.

Most mothers perceived their roles in surgical decision-making as semi-active or collaborative, and there was no significant correlation between the PSI score and role in surgical decision-making among all mothers in the present study. However, there were significant correlations between the PSI score and the role in surgical decision-making and between the DC score and role in surgical decision-making in mothers whose children had polydactyly of the foot (Figure 1). Additionally, mothers with a higher PSI or DC score preferred a more active role in surgical decision-making.

Associations between the PSI score and its subscales and the role in surgical decision-making in mothers of children with polydactyly of the foot. PSI: Parenting Stress Index.
The PSI score of mothers whose children had polydactyly of the foot was associated with their role in surgical decision-making, and mothers preferred to be more actively involved in decision-making as the PSI score increased (Table 4). In mothers whose children had a hypoplastic thumb, a history of surgery in the child was associated with an active role of the mother in surgical decision-making (Table 5). Among all mothers and the mothers of children with polydactyly of the hand, those who feared the burden of the medical costs had a higher PSI score (Tables 6 and 7).
Logistic regression analysis of the factors associated with the preferred roles in surgical decision-making of mothers of children with polydactyly of the foot.

PSI: Parenting Stress Index; PD: Parental Distress; PCDI: Parent–Child Dysfunctional Interaction; DC: Difficult Child; OR: odds ratio; CI: confidence interval.
The p-value in bold means that the p-value is less than 0.05.
Logistic regression analysis of the factors associated with the preferred roles in surgical decision-making of mothers of children with hypoplastic thumb.

PSI: Parenting Stress Index; PD: Parental Distress; PCDI: Parent–Child Dysfunctional Interaction; DC: Difficult Child; OR: odds ratio; CI: confidence interval.
The p-value in bold means that the p-value is less than 0.05.
Logistic regression analysis of the factors associated with the high stress (PSI score ≥90) of mothers of children with congenital hand or foot differences.
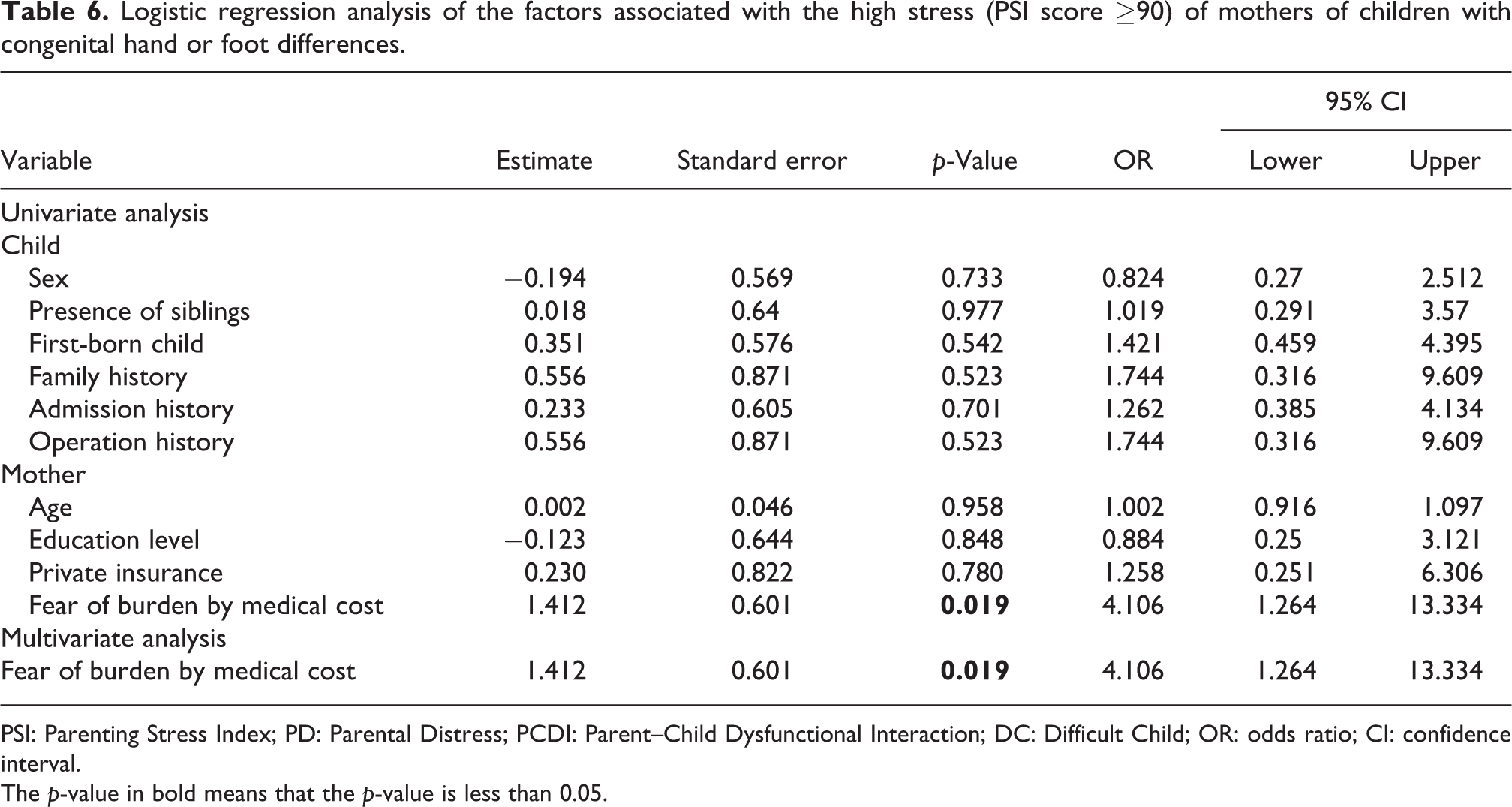
PSI: Parenting Stress Index; PD: Parental Distress; PCDI: Parent–Child Dysfunctional Interaction; DC: Difficult Child; OR: odds ratio; CI: confidence interval.
The p-value in bold means that the p-value is less than 0.05.
Logistic regression analysis of the factors associated with the high stress (PSI score ≥ 90) of mothers of children with polydactyly of the hand.
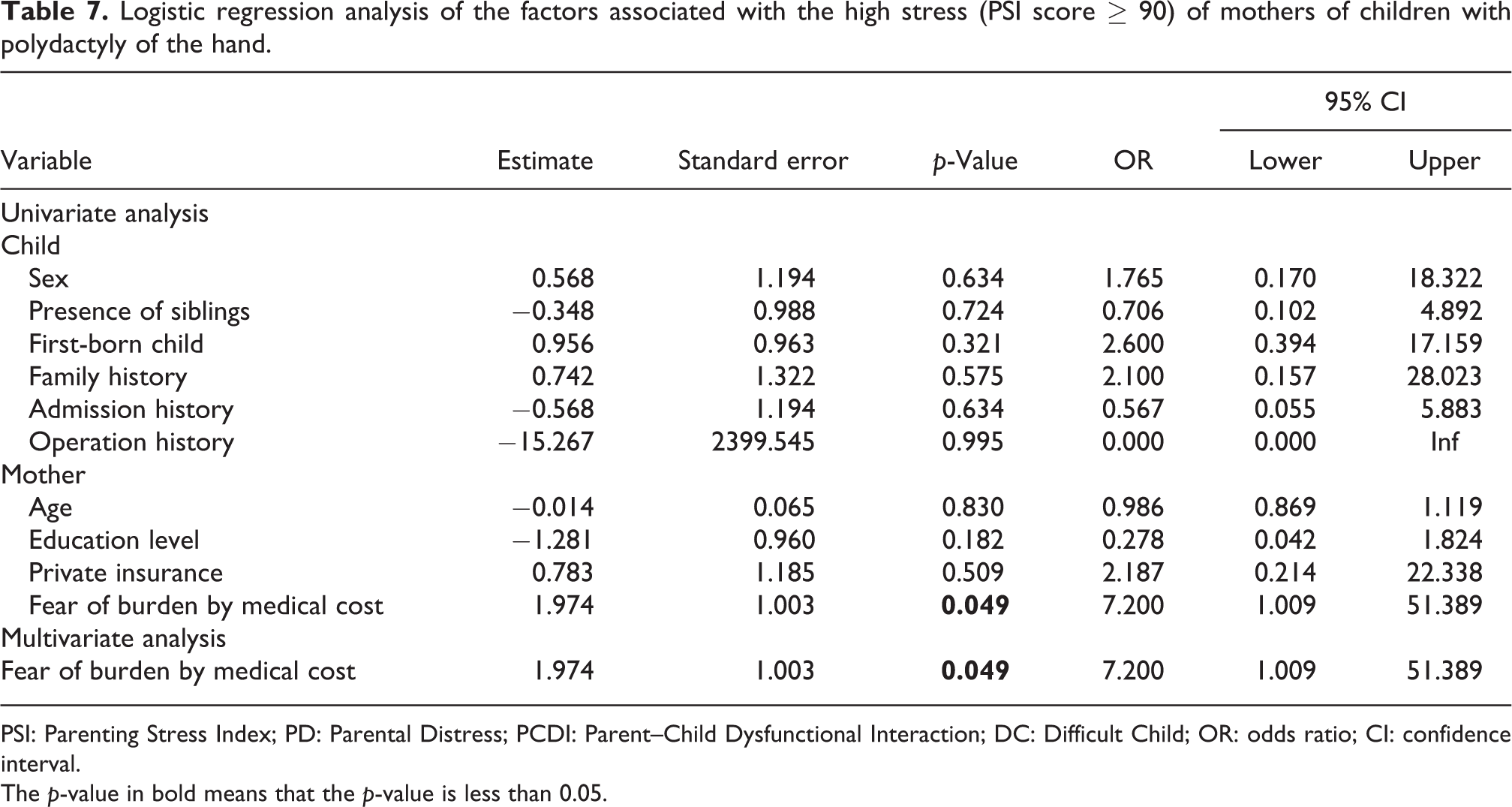
PSI: Parenting Stress Index; PD: Parental Distress; PCDI: Parent–Child Dysfunctional Interaction; DC: Difficult Child; OR: odds ratio; CI: confidence interval.
The p-value in bold means that the p-value is less than 0.05.
Prediction models for the five levels of involvement in surgical decision-making were constructed for all mothers and mothers whose children had polydactyly of the hand and foot (Figure 2). Additionally, prediction models for the levels of involvement in surgical decision-making after defining the level of involvement as active or not active were constructed (Figure 3).
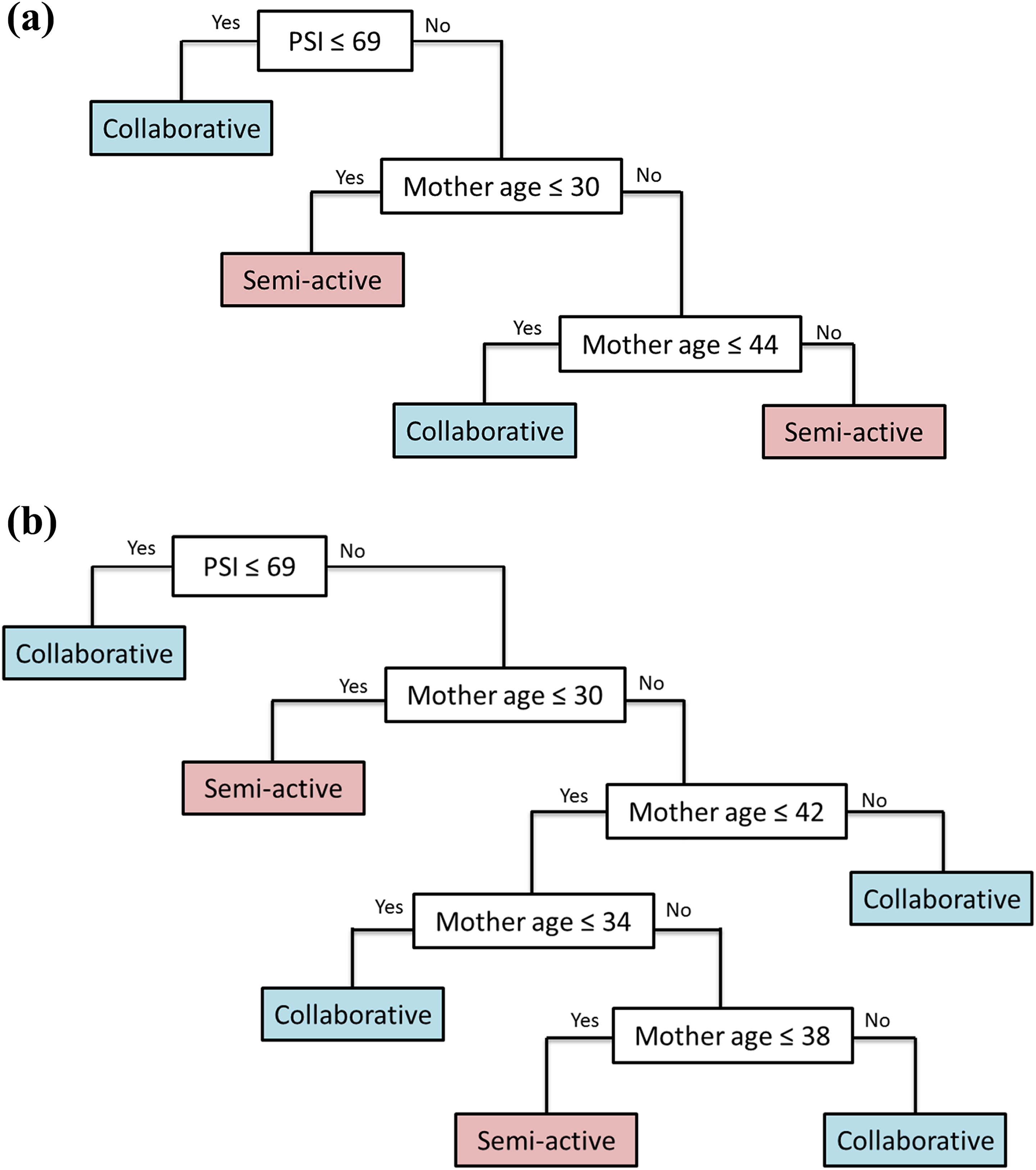
Prediction models for the five levels of involvement of mothers in surgical decision-making. Prediction model for mothers of children with (a) congenital hand or foot differences and (b) polydactyly of the hand and foot.

Prediction models for the style (active or not) of involvement of mothers in surgical decision-making. Prediction model for mothers of children with (a) congenital hand or foot differences and (b) polydactyly of the hand and foot.
Discussion
A total population study conducted in Stockholm, Sweden, reported the incidence of congenital anomalies of the upper limb as 21.5 per 10,000 live births. 19 Although this incidence is higher than those for cleft lip and palate and neural tube defects, 20,21 few studies have investigated the psychological variables associated with the parents of children with congenital hand or foot differences. Jeong et al. evaluated the psychological state and stress levels of Korean mothers with children with cleft lip and palate and concluded that psychological analyses of depression, anxiety, and stress in mothers play a vital role in screening for psychiatric treatment or consultation. 22 Among the mothers of children with spina bifida, single-parent families and the need for clean intermittent catheterization of the bladder were associated with high parenting distress scores. 23 Franzblau et al. reported that children with congenital hand differences often experience emotional stress related to their functional limitations and aesthetic deformities. The authors suggested that clinicians caring for these children should inform families about potential sources of stress and direct them to resources regarding coping strategies and support systems. 24
Uzark and Jones showed that the average PSI score of parents of children with congenital heart disease was 77, and that 17.5% of these parents had a clinically significant level of stress (≥90th percentile).25 These parenting stress levels and proportions of parents with clinically significant stress levels are similar to those observed in the present study. A study on parenting stress in the parents of children with craniofacial anomalies found that the mean PSI-SF score was 77.5 for parents of children from newborn to 24 months of age and 70.2 for parents of children 24–46 months of age. 26 Similarly, the average PSI score of mothers of children with spina bifida was reported as 86.2 by one study23 and as 77.7 by another study. 27 Thus, the PSI score appears to be similar or slightly lower for mothers of children with congenital hand or foot differences compared with parents of children with congenital heart disease, a craniofacial anomaly, or spina bifida.
Madrigal et al. investigated parental decision-making preferences in a pediatric intensive care unit and found that the majority of parents in this population prefer either a shared decision-making role with the doctors (40%) or making the final decision, or at least most of it, on their own (41%). 28 In the present study, most mothers preferred either a semi-active or collaborative role in surgical decision-making for their children. Although there was no significant association between the level of parenting stress and the preferred role in surgical decision-making among all mothers in the present study, there were significant associations between the PSI or DC score and the preferred role in surgical decision-making of mothers of children with polydactyly of the foot. Davison and Breckon evaluated the factors that influence treatment-related decision-making and information preferences among prostate cancer patients on active surveillance and found that patients with higher levels of anxiety want access to more information compared with those with lower levels of anxiety. 29
There are several possible reasons why mothers with higher levels of parenting stress preferred an active role in surgical decision-making in the present study. Women carrying a fetus with a congenital abnormality may feel guilty 30 and, thus, desire to play a more active role in decision-making to compensate for those feelings. Rosenberg et al. reported that visibility of the condition should be considered a risk factor for increased stress in mothers of infants with single-suture craniosynostosis. 31 Similarly, Vermaes et al. reported that the severity of a physical dysfunction in a child is positively associated with parenting stress. 32 Because congenital hand or foot differences are conspicuous, mothers may have a higher level of parenting stress considering the appearance of their child and, therefore, may have a tendency to seek proper treatments more actively. It is also possible that mothers with higher levels of parenting stress have a propensity for active participation in social work rather than household affairs.
Vrijmoet-Wiersma et al. reported that both the fathers and mothers of children with congenital cardiac disease exhibit significantly higher rates of perceived vulnerability than those of the parents of healthy children. 33 These authors concluded that the psychosocial screening of parents of children with congenitally malformed hearts is important for providing appropriate counseling to those parents most in need. Similarly, Uzark and Jones recommended that clinicians should assess parenting stress levels at each health-care visit to provide appropriate support and anticipatory guidance to the families of children with heart disease. 25 In the present study, the level of the mother’s parenting stress and its influence on her role in surgical decision-making were determined. This relationship was particularly important in the mothers of children with polydactyly of the foot, and it was possible to predict a mother’s preferred role according to the level of parenting stress in this subgroup. Therefore, clinicians should alter their decision-making style based on PSI assessments.
The present study has several limitations that should be noted. First, this study included mothers of children with four different congenital hand or foot conditions: polydactyly of the hand, polydactyly of the foot, a hypoplastic thumb, and macrodactyly. Because the number of mothers in each subgroup was small, all mothers were included in the present study. However, the same statistical analyses were also performed for the participants within each subgroup. Second, many other congenital conditions were not included in this study, and therefore, the present findings cannot be generalized to all mothers whose children have congenital hand or foot differences. Third, the parenting stress levels were not assessed in fathers whose children had congenital hand or foot differences.
In conclusion, the levels of parenting stress in mothers of children with congenital hand or foot differences were similar or slightly lower than those of parents of children with other congenital anomalies. Of the mothers of children with polydactyly of the foot, those with higher levels of parenting stress preferred a more active role in surgical decision-making. The present study also showed that PSI assessments can aid in the prediction of a mother’s preferred role in this type of decision-making. Thus, it will be important to pay attention to and screen for stress levels in the mothers of children with congenital hand or foot differences to provide appropriate psychological and emotional support and to develop tailored interventions for this population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.