
Abstract
Background:
Large resection and reconstruction of the malignant tumors of the shoulder girdle are used to provide maximum protection of the soft tissues with sufficient surgical margin. However, these have their own difficulties. The goals of this study were to review demographic data of 187 patients diagnosed with the malignant tumors located around shoulder between 2001 and 2016 in our clinic, to evaluate the functional outcomes and surgical outcomes, and to classify the resection methods according to new classification systems.
Methods:
There were 187 patients (108 male and 79 female) and the mean age at surgery was 47.9 (range 2–87). Fifty-one of these patients underwent biopsy only: 8 partial/total claviculectomy, 10 partial/total scapulectomy, 80 proximal humeral resection, 5 total humeral resection, 6 shoulder girdle resection, and 13 amputations. Eighty-six had prosthetic implants, five had fibula transpositions, and one had a massive homologous bone graft. Seventy-one of the 136 patients were followed for an average of 40.3 months.
Results:
When the bone resections were evaluated, the best results were obtained while the rotator cuff function is preserved in glenoid preserving partial scapulectomy, partial/total claviculectomy, and proximal humerus intercalary resection. In total, scapulectomy and proximal/total humeral resection operations’ results were moderate because of partial or total injury of the abductor mechanism.
Conclusions:
As a result, malignant tumors of the shoulder girdle and soft tissue can be treated with limb-sparing surgery procedures. Reconstructive procedures and reconstructive methods such as prosthetic replacement, auto-allograft, and soft tissue reconstructions should be specified in each case. These resection and reconstruction methods are reliable and applicable procedures for local tumor control, pain control, and functional outcomes. More rarely, amputation/disarticulation can be performed.
Background
In the surgical treatment of malign tumors of the shoulder girdle, disarticulation forequarter amputations were performed until the middle of the 20th century. Interestingly, Tikoff-Limberg procedure was applied to only patients who had low-grade tumour. Limb-sparing surgery was done through extensive preoperative evaluation, advanced imaging techniques, efficacy of adjuvant chemotherapy, and developed surgical reconstruction techniques. 1 –5
We analyzed the demographic data, treatment planning, surgical procedures, complications, and oncologic and functional outcomes of 187 patients with malignant bone and soft tissue tumors of the shoulder girdle. We described a modified classification, including a recent popular procedure, a partial scapulectomy procedure with resection of glenoid, and some other bone resection procedures.
One of the purposes of this study was to obtain demographic data of malignant bone and soft tissue tumors of the shoulder girdle region by analyzing all malignant tumors of shoulder girdle in patients who underwent biopsy. These were done using limb-sparing surgery and were amputated. The other purpose was to describe a classification system to include all types of bone resection that can be applied to malignant tumors of the shoulder girdle. It was also aimed to guide orthopedic surgeons in preoperative planning by identifying specific functional outcomes and complications for each resection method described in the classification.
Method
One hundred eighty-seven patients (79 female (42%), 108 male (58%)) with malignant tumor of shoulder girdle that were operated on in our clinic between 2001 and 2016 were examined retrospectively. A total of 105 patients had primary tumor and 82 patients had metastatic disease. The histopathological diagnoses of the patients are summarized in Table 1. The mean age at surgery was 47.9 (range 2–87) and the mean age was 39.7 (range 2–87) in the group that had primary tumors and 58.5 (range 6–87) in the group that had metastatic tumors.
Distribution of histopathological diagnoses.

Fifty-one of the patients were transferred to other related sections after diagnosis histopathologically by biopsy (inoperable patients or patients who had just chemotherapy/radiotherapy planned, etc.).
A new classification system for resection of malignant bone and soft tissue tumors around the shoulder girdle was described (Figure 1). Only 51 patients underwent biopsy, 13 patients with amputation/disarticulation, 14 patients with soft tissue resection, and 5 patients with total humeral prosthesis were excluded from the classification. Accordingly, they were classified as type 1: claviculectomy (partial/total) or partial scapulectomy (partial resection of the scapular body at any localization/total resection of the body); type 2: partial scapulectomy with resection of glenoid and preservation of medial scapula; type 3: proximal humeral resection; type 4: intercalary resection of the proximal humerus; type 5: total scapulectomy; type 6: total scapulectomy + humeral head resection; type 7: partial scapulectomy + proximal humerus resection; and type 8: extraarticular proximal humerus + total scapula resection. All types were categorized as “Type A: abductor mechanism is preserved” and “Type B: abductor mechanism partial/total is resected.”

Resections of shoulder girdle (see the text).
In our study, 15 patients were treated with type 1 (Figure 2(a) and (b)), 1 patient with type 2, 74 patients with type 3, 6 patients with type 4, 1 patient with type 5 (Figure 3), 1 patient with type 7, and 6 patients with type 8. The type 6 resection was not performed on any patient.
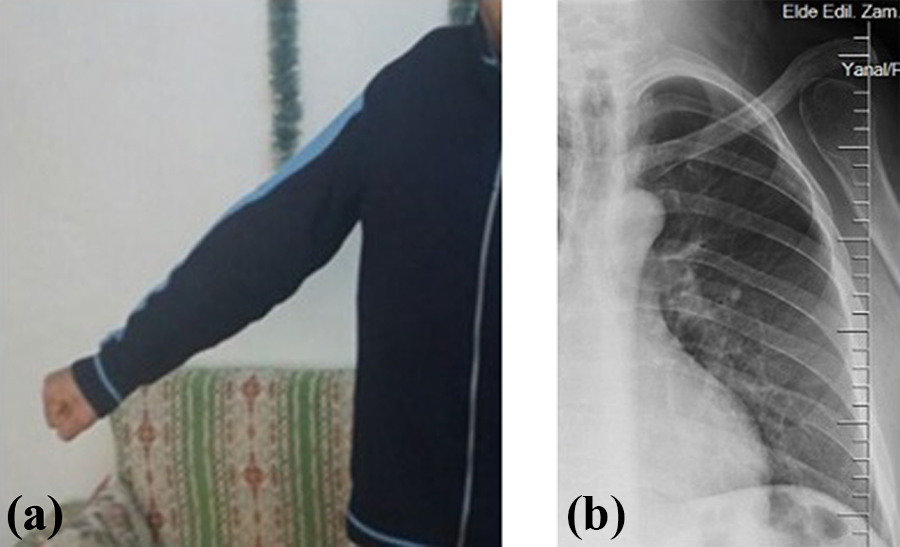
(a) Functional appearance after partial scapulectomy with only glenoid and acromion is preserved. (b) Direct radiography which is 5 years postoperative after type 5 resection.

Clinical presentation which is 4 years postoperative after total claviclectomy.
Fibular grafting was performed in two of the six patients who were received partial claviculectomy. Fresh frozen osteoarticular allograft was performed on one patient who underwent type 2 resection (Figure 4(a) and (b)).

(a) Chondrosarcoma in glenoid. (b) Reconstruction with fresh frozen allograft scapula after resection with wide margin; the lateral half of the preserved clavicle was stabilized to the acromion and medial clavicle.
At the time of reconstruction after type 3 resection performed in 74 cases, a tumor endoprosthesis (71 proximal humerus resection prosthesis, 2 inverse tumor prosthesis, and 1 total shoulder tumor prosthesis) was performed in all.
In six cases of reconstruction after type 4 resection, fibular graft was applied in three patients and cement spacer + intramedullary nail in three patients (Figure 5(a) to (c)). In five cases of reconstruction after total humeral resection, total humeral protheses were performed.

(a) and (b) Postoperative antero-posterior and lateral radiographs after intramedullary nail and cement spacer application after intercalary resection because of pleomorphic sarcoma in the right proximal humerus. (c) Postoperative good function.
In four of six patients with type 8 resection, a custom-made total scapular prosthesis + proximal humerus tumor endoprosthesis was performed (Figure 6(a) to (c)). Proximal humerus tumor endoprosthesis was performed in the other two patients, and one patient underwent type 7 resection (Figure 7(a) and (b)).

(a) Scapula + proximal humeral tumor. (b) Appearance of resection material after extra-articular resection. (c) Postoperative direct radiography after reconstruction with massive allograft.

(a) Type 8 resection + proximal humerus tumor resection prosthesis and suspension of prosthesis to clavicle. (b) Prosthesis luxation in the postoperative period.
Polyclinic data of Musculosceletal Tumour Society Scoring System (MSTS) scoring, which gave information about the physical examination findings and functional results of the patients’ last application, were evaluated together with radiographic findings.
It was aimed to determine the functional differences between the resection types by evaluating the functional outcomes and results of the MSTS system. Also a number of patients in some types of resection were insufficient. Therefore, functional outcomes were assessed for the preservation resection of the abductor mechanism or reconstruction type independently.
Results
Amputation/disarticulation was performed in 13 (9.6%) patients who underwent operation, and limb-sparing surgery was applied to the other 123 of 136 (90.4%) patients. Forty-five of 136 (33%) patients who underwent operation were under our control, 26 patients (19%) abandoned follow-up, and 65 patients (48%) died.
The mean duration of follow-up in all the 136 patients was 29.5 months (range 12–191 months) and patients who were followed for at least 12 months were included in our study (31 patients died within 12 months).
The mean follow-up time was 37.0 and 16.0 months in patients who had primary and metastatic disease.
Oncologic efficacy
At the time of admission, 22 of 37 patients with primary localized disease were followed as “disease free” during the mean follow-up period was 67.6 months (12–191 months). Sixty-five patients died at an average rate of 17.7 months. When patients’ recent polyclinic examination grades were generally evaluated, patients demonstrated satisfaction from functional outcomes after shoulder malignant tumor surgery.
When complications were examined, postoperative complications were observed in 15 patients and relapses were observed in 14 patients (Table 2). A single patient had delayed wound healing, four patients had skin defect, and two patients had prosthetic infection. Prosthetic infection was occured in one of four patients who underwent type 8 resection. Custom-made scapular prosthesis, proximal humerus resection prosthesis, and skin defect occurred in three of these patients. A skin defect occurred in one patient who underwent type 3 resection and proximal humerus endoprosthesis. In addition, prosthetic infection, aseptic stem loosening, and luxation occurred each in a single patient. In one patient who had total humerus prosthesis, severe elbow pain developed and pain was felt despite of strong analgesics. In the patient who received type 2 resection and osteoarticular allograft and one that underwent partial claviculectomy and fibula graft, pin migration developed and pin extraction was performed. Luxation developed in the patients who underwent type 8 resection, proximal humerus resection of the tumor prosthesis, and prosthesis clavicle suspension.
Complications and relapse.

Functional results and quality of life
Type 1 resection
We performed partial claviculectomy in six patients, total claviculectomy in two patients, partial resection of scapular body in three patients, and scapular body resection with glenoid preserved in four patients. We obtained better functional results than the other types because we were able to protect the rotator cuff in most cases (Figure 8). Patients whose Abductor mechanism was completely preserved and the type 4 resection group had the best functional outcomes.
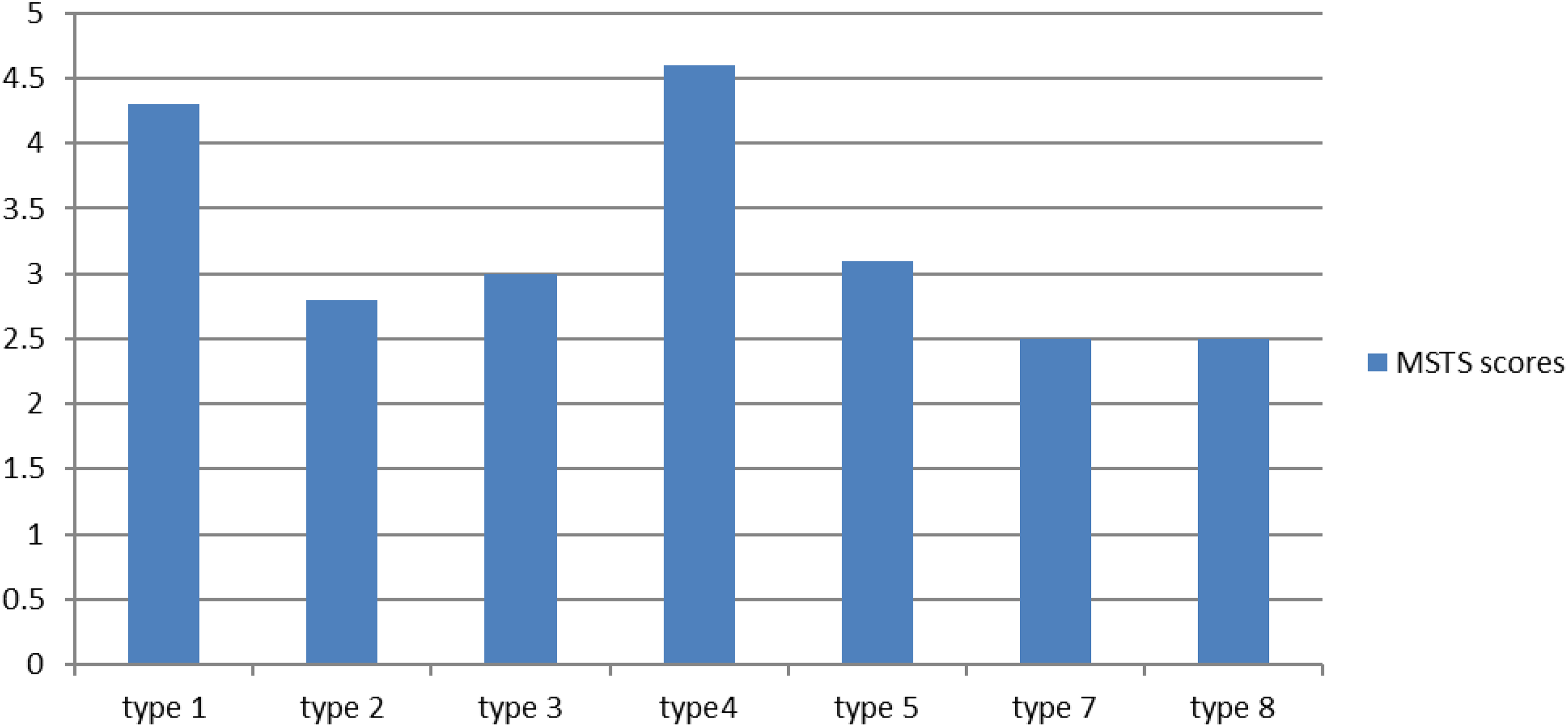
MSTS scores of resection types of shoulder girdle. MSTS: Musculosceletal Tumour Society Scoring System.
Type 2 resection
Glenoid + acromion + clavicle shaft resection was performed with preserving the scapula medial in one patient. One fresh-frozen scapula was placed, the lateral tip of the distal clavicle was fixed to acromion, and the medial tip of distal clavicle was fixed to proximal clavicle. At the postoperative 51st month, the scapula allograft union was found. However, the nonunion in the clavicle, as well as the acromion displacement and pin migration, was observed. Therefore, revision surgery was done.
Type 3 resection
A total of 74 patients underwent type 3 resection. In all patients, tumor endoprosthesis (71 proximal humeral resection prosthesis, 2 inverse tumor prosthesis, and 1 total shoulder tumor prosthesis) was applied. Thirty-five patients were primer and 38 patients had metastatic disease. The rotator cuff and deltoid muscle can be completely protected in some patients, while others were totally resected in some partial patients. Functional outcomes were generally proportional to the rate of preservation of abductor structures while the results were moderate-to-good in both patient groups (Figure 8).
Type 4 resection
Type 4 resection was performed in six patients. Three patients were reconstructed with a free fibular graft, preserving the proximal humeral physis lines as far as possible, as the physiology did not close. In three patients, intramedullary humerus nail + defect area was applied with a cement spacer after en bloc resection of tumoral segment. In this group, regardless of the reconstruction type, both functional outcomes and patient satisfaction had the best functional outcomes in the study.
Type 5 resection
Type 5 resection was performed in one patient and the proximal humerus was stabilized in clavicle with biceps long head and tapes. Movements depending on rotator cuff and glenoid resection were very limited. The patients had abduction movement among 25°–35° and had a moderate functional outcome.
Type 7 resection
Type 7 resection was performed in one patient. Proximal humerus was stabilized to clavicle and remained scapluae with biceps long head and tapes. In this case, movements depending to rotator cuff and glenoid resection were very limited.
Type 8 resection
Type 8 resection was done in six patients. In four of these patients, custom-made scapula prosthesis + proximal humerus resection prosthesis were applied. Wound problems occurred in all these cases and prosthetic infection developed on one side. In two patients, proximal humerus tumor resection prosthesis was performed after resection. First, a plaque was placed to the lateral side of the clavicle. The long head of biceps and prosthesis were suspended in the remaining clavicle and plaque by tapes, prolene mesh, and proximal holes of the tumor prosthesis. Postoperative luxation was observed in one patient, and therefore a revision was made.
Discussion
Large resection and reconstruction of the malignant tumors of the shoulder girdle for providing maximum protection of the soft tissues with sufficient surgical margin have their own difficulties. 6,7
Before 1970, shoulder girdle tumors were generally treated with amputation. Limb-sparing surgeries have been applied up to 80% with the development of imaging modalities, adjuvant therapies, and surgical techniques. 1,4,5,8 In our study, the ratio of limb-sparing surgery was determined as 90.4%.
Limb-sparing resection of the shoulder girdle has three steps: tumor resection, bone defect reconstruction (if required), and soft tissue reconstruction. 2,3,6 In 1991, Malawer et al. described a classification based on the status of resection types, glenohumeral joints, and abductor mechanics. 9,10 This classification has been used in many studies day by day and many reconstruction methods have been described. 4,5,7,11 –19
Since the 1990s, the glenoid resection and reconstructions have been defined by preserving the medullary scapula, but neither the resection type nor the clavicle resections have been included in traditional classifications. 3,7,11,12,20 We described a modified classification system. Therefore, we included both an increasingly common type of surgery in recent years and provide more surgical procedures with shoulder girdle in the classification.
In this classiffication, regardless of the type of reconstruction, it is possible to give an idea about the type of resection applied, functional outcomes, and possible complications. In type 1 and type 4 resections, functional results and fewer complications through better preservation of muscles and related structures were observed. In the other six types, however, functional results were obtained as close to each other according to our study. These were ranked type 5, type 3, type 2, and type 7–8 toward best to worst. Specific complication rates and types for each type were described. When the literature was examined, the results of partial scapulectomy were good in most studies and the mean MSTS scores were 72–88%. 1,14,21 Functional results were published about partial and total scapulectomy. Although functional outcomes were bad in the literature for other types, they were better than amputation. 21 –23
Our study only involved malignant tumors as distinct from many other studies. In addition, all patients were included in the study and therefore the number of patients with metastatic disease was relatively higher than other studies. Because of these two factors, the mean age of our study was higher than the other studies (mean age 47.9 in our study, 39.7 in patients with primary disease and 58.5 in patients with metastatic disease). This study had a higher number of patients than the other studies. Because of these three features, we think that our study better reflects the demographic data of malignant tumors located around the shoulder.
When reconstruction methods were examined, it was reported that bone reconstruction was not required after partial scapulctomy and partial or total claviculectomy. 5,22 Also, it was reported that soft tissue reconstructions can be performed. We did not perform bone reconstruction in the scapula but only reconstructed some of cases where partial resection was done to distal clavicle. The functional results were rather good in all patients, but we encountered complications depending on reconstructions.
Scapular allograft reconstruction can be performed after type 2 resection and complications can occur such as shoulder pain and infection. 7 We applied this to one case and showed acromion displacement and pin migration despite full union.
After the resection of the proximal humerus, fibular graft, osteoarticular allograft, tumor prosthesis replacement, and many other procedures have been described in the literature. The most reliable procedure has been reported to be prosthetic replacement. 3,13,15,17,18 In our study, prosthetic replacement was the most common procedure.
After interacalary resection, fibular graft or cement + nail reconstruction can be applied. Good results have been reported after fibular graft. 1 One of the types with the best functional results was this group.
After total scapulectomy, scapular endoprosthetic reconstruction or humeral suspension can be applied. We performed the humeral suspension procedure in one case and we did not encounter any complications with moderate functional results. 16 The most common reconstructive procedures after extraarticular resection of the scapula and proximal humerus are prosthetic replacement or suspension. 7,12,16 In our study, after the type 7 and type 8 resections, we applied both methods by based on patient-specific criteria. Reconstruction with massive scapula-proximal humerus osteoarticular allograft has also been reported. 4
In our study, 45 (33%) of the 136 patients who were operated on were still under follow-up, 65 (48%) died, and 26 patients (19%) left follow-up. While the reasons for the death rate being higher than other studies are under investigation, benign and malignant tumors were examined together in the majority of studies of other shoulder girdle tumors. In addition, some cases only had primary tumors included in the study. In other cases, all patients were treated at the same hospital since the initial diagnosis. 1,5,7,24 The ratio of the number of metastatic patients to the number of primary patients in our study was much higher than the other studies.
At the time of admission, 22 (60%) of 37 patients with primary localized disease were followed for an average of 67.6 months (range: 12–191 months) as disease free after surgery. This ratio was 51% in the study of Kiss et al. in which benign and malign tumors were evaluated together and 66% in a study by Yang et al. 1,5
This study has some limitations. Firstly, it was a retrospective study. In addition, the number of patients in some of the resection types in the classification was very low and insufficient. However, it was not possible to achieve functional results according to the preservation and ablation of the abductor mechanism or according to the different reconstruction types specific to each resection, because of insufficient number of patients in the types.
Conclusion
As a result, malignant tumors of the shoulder girdle and soft tissue can be treated with limb-sparing surgery procedures. Reconstructive procedures and reconstructive methods such as prosthetic replacement, auto-allograft, and soft tissue reconstructions should be specified in each case. These described resection and reconstruction methods are reliable and applicable procedures for local tumor control, pain control, and functional outcomes. More rarely, amputation and disarticulation can be performed.
Footnotes
Acknowledgment
The authors would like to thank investigators, patients, and their families.
Authors’ contribution
RÖ made the study design, data collection and interpretation, and manuscript writing. BŞG did the final approval of the manuscript. Both authors read and approved the final manuscript.
Availability of data and materials
Please contact the corresponding author for data requests.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.