
Abstract
Background and objectives:
Malignant primary chest wall tumors (PCWTs) comprise a rare group of thoracic tumors with unique anatomical considerations, and experience with wide surgical resection is limited to specialty referral centers and specific diagnoses. We investigated the tumor recurrence and overall survival (OS) for patients with a variety of PCWTs diagnoses at our institution.
Methods:
From 1991 to 2010, patients with malignant PCWT undergoing wide surgical resection for curative intent under a single surgeon were reviewed. Diagnosis and grade (if applicable) of surgical pathology, along with patient demographics, neoadjuvant chemotherapy or radiation therapy, and outcomes (complications, recurrence, and OS) at follow-up were analyzed.
Results:
One hundred fifteen patients were included in the study. The most common tumor diagnoses included pleomorphic sarcoma and liposarcoma. Negative margins were achieved in 70 (74%) of cases. Postoperative complications were reported in 21 (20%) cases. The 5-year survival rate was 54%, while the 10-year survival rate was 29%. The local and distant recurrence rates were 50% and 38%, respectively. OS was significantly less in patients with any recurrence (p < 0.001) but not significantly different between pathology grades (p = 0.28).
Conclusions:
Wide resection for malignant PCWT is feasible when undertaken for a heterogenous group of diagnoses.
Introduction
Primary chest wall tumors (PCWTs) are rare malignancies that constitute 5% of all thoracic tumors, arising from the skin, soft tissue, neuromuscular structures, cartilaginous tissue, or bony structures of the thorax. The three most common causes of malignant PCWT include chondrosarcomas, liposarcomas, and fibrosarcomas. 1,2 Surgical treatment may be preceded or followed by radiotherapy according to local protocols, especially when narrow margins are expected or confirmed in the pathological specimen. However, special considerations of the anatomical constraints of the thorax, on part of the oncologic surgeon, are required to achieve a negative margin with resection.
Prior cohort studies have reported on a combination of surgical techniques in affected patients, and these procedures range from incisional biopsy to wide resection for curative intent (i.e. negative margins). 3 –9 The largest study of wide resection for curative intent for PCWT consists of 98 patients, 6 and the majority of studies focus on a few specific diagnoses, primarily chondrosarcomas. 4,6,7,10 –15 At our institution, all PCWTs are considered as a heterogenous group of tumors that receive similar preoperative evaluations and surgical resections, regardless of perioperative chemotherapy or radiation therapy protocols. We sought to determine the overall survival (OS) and tumor recurrence in PCWT patients with a broad range of diagnoses receiving surgical resection for curative intent by a single surgeon at our tertiary referral specialty center.
Methods
Data collection
The Human Subjects Division at the University of Pittsburgh Medical Center determined that this study was exempt from review by the Institutional Review Board. We collected data on all adult patients who received a surgery for malignancy that required any surgical resection to achieve negative margins (i.e. curative intent) on pathology specimens during the study period (1991–2010) at our institution by a single surgeon (MAG). This includes primary malignant chest wall tumors that involve partial or total rib resection (including rib processes and inter-rib spaces) with one or more of the following components: (1) skin, (2) subcutaneous soft tissue including fat and muscle, and (3) nerve and vascular bundles. Exclusion criteria included a history of breast cancer, surgical resection for tumors not found to be part of the chest wall, and metastatic tumors from any location. We also excluded patients with missing information regarding pathological diagnosis, operation date, and tumor location. For patients with multiple or staged procedures, we collected data on the most recent operation. Both the surgical date and the follow-up interval were thus determined from the most recent surgical date.
We reviewed patients’ medical records for surgical reports, radiographic studies, and pathological results to determine primary location, neoadjuvant treatment, primary local treatment, adjuvant treatments, local or distant recurrence, and late complications. All patients received a thorough evaluation for the extent of local and distant disease, including computed tomography scan and magnetic resonance, when appropriate to exclude spinal cord or mediastinal involvement. A complete workup was undertaken in all cases to eliminate a disseminated disease. Wide resection margins depended on the dimension and the location of the tumor, and, in all cases, resection included the adjacent sternocostal cartilages and adjacent portions of neighboring ribs. Resection and reconstruction were performed as a one-stage procedure in all cases.
For those patients who underwent surgical resection of a primary lesion, margins were described as negative or positive on the basis of review of pathological analysis, and all complications were recorded. Length of follow-up and time to recurrence were calculated based on the date of surgery and collection of the pathological specimen. All patients received clinical follow-up and MRI every 3 months for the first year, every 6 months for the next 2 years, and then annually if no recurrence was detected. If there was tumor recurrence or metastasis, then appropriate staging imaging and biopsies were performed.
Statistical methods
Univariate analyses were performed for comparison between outcome groups (e.g. local or distal recurrence and OS). Group differences in individual variables (demographic, clinical characteristics, and outcomes) were assessed using χ 2 tests along with the Fisher’s exact test correction when needed. Kaplan–Meier survival curves were created for OS as well as event-free survival. Log rank (Cox–Mantel) test was used to determine statistical significance between survival curves. Logistic regression was used to determine independent covariates for tumor recurrence. Statistical analyses were conducted with PASW Statistics 18 and 19 (IBM SPSS; IBM Corporation, Somers, New York, USA).
Results
Demographics
We identified 115 eligible procedures of a total of 599 operations for chest wall tumors during the study time period. Supplementary Table 1 lists the study exclusion criteria. Supplementary Table 2 lists the different malignant PCWTs in our study population. Pleomorphic sarcoma (n = 18; 15.6%) and liposarcoma (n = 16; 13.9%) were the most common primary malignant chest wall tumors in this series. Table 1 lists the demographic and tumor characteristics of the study population. Fifty-three patients were assigned grade classifications that were determined to be high-grade pathology, 16 patients with intermediate-grade pathology, and 21 patients with low-grade pathology. Twenty-five patients did not have a recorded grade and were regarded as indeterminate. Six patients had distal recurrence at the time of presentation for surgical wide resection of the PCWT. Negative margins were achieved in 70 cases (74%) with available data.
Study characteristics, January 1990–October 2010.

Post-op: postoperative; SD: standard deviation.
Postoperative outcomes
Table 2 lists the postoperative outcomes of the study cohort. Follow-up data were available in 109 patients. Forty-five patients (41%) were deceased at the time of follow-up, of which 39 cases (87%) had confirmed disease recurrence. The 5-year survival rate was 54%, while the 10-year survival rate was 29%. The overall complication rate was 20% (23 cases), with the majority being surgical site infections (48%). There were no perioperative deaths. Supplementary Table 3 lists all postoperative complications experienced by the time of follow-up in our study cohort.
Postoperative course and follow-up.
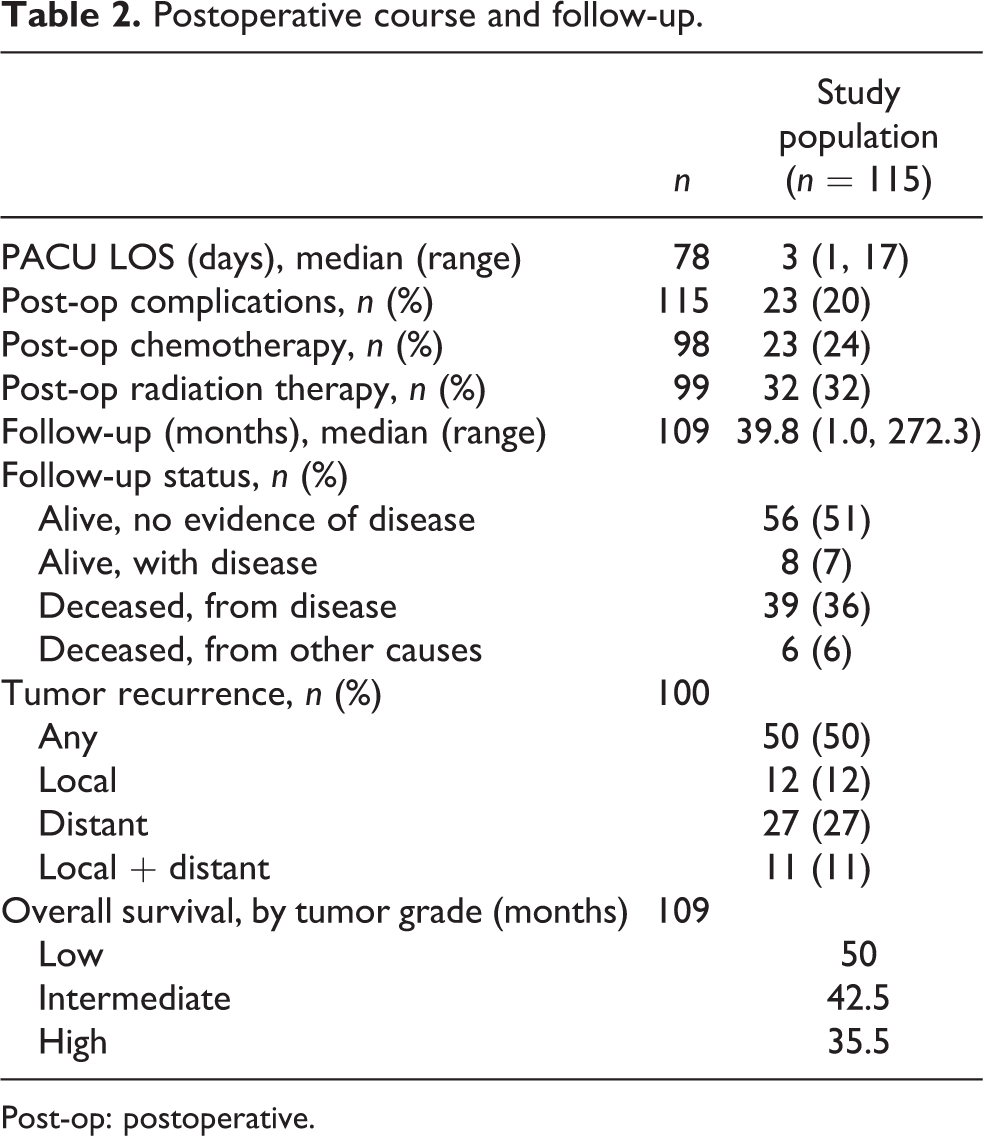
Post-op: postoperative.
Tumor recurrence
Follow-up data regarding tumor recurrence (local and/or distant) were available in 100 patients. Fifty patients (50%) had local-regional or distant tumor recurrence, and 38 patients (38%) had reported distant lesions at the time of follow-up. Table 3 lists patients, tumors, and postoperative characteristics by disease recurrence status. There were no statistically significant associations between recurrence status and demographic, procedural, or post-procedural characteristics. There was no statistically significant difference in the proportion of patients who achieved R0 margins between patients with and without any recurrence (68% vs. 83%; p = 0.20).
Tumor recurrence (local and distant) and univariate predictors.a
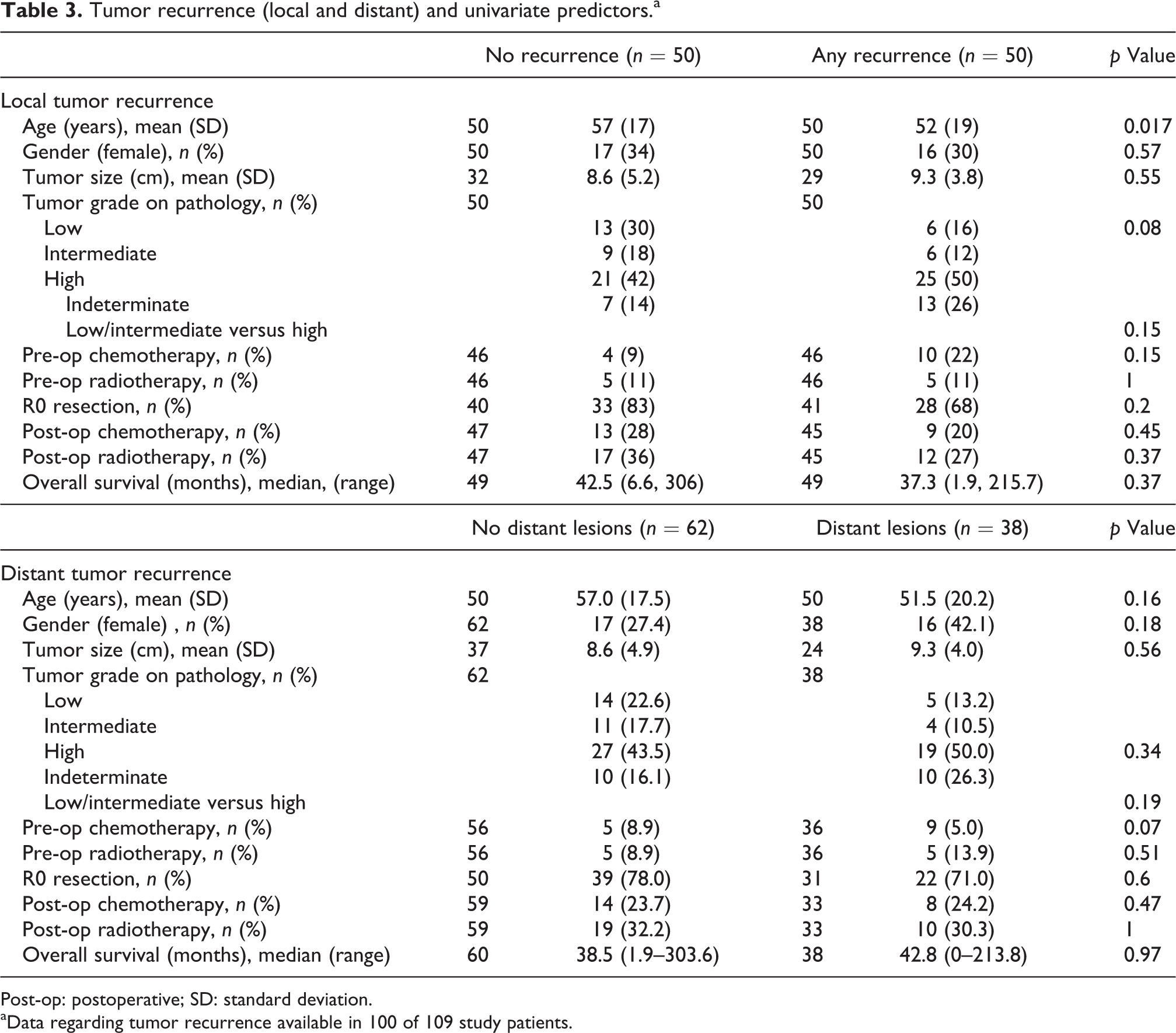
Post-op: postoperative; SD: standard deviation.
aData regarding tumor recurrence available in 100 of 109 study patients.
Overall survival
Figure 1 demonstrates the OS for the study cohort. At the time of follow-up, 45 (41%) of 109 patients with available data were deceased (Table 4). The median OS was 38.4 months (1–303.6 months). There was no statistically significant difference in OS between patients with low/intermediate versus high-grade tumors after the initial surgical resection (p = 0.28; Figure 2). Patients who experienced local or distant recurrence after initial resection demonstrated a significantly shorter OS compared to patients without recurrence (p = 0.0001; Figure 3).

Kaplan–Meier curve of OS: study cohort. OS: overall survival.
Overall survival at follow-up and univariate predictors (n = 109).a

Post-op: postoperative; SD: standard deviation.

Kaplan–Meier curves of overall survival according to tumor grade. Log-rank test: p = 0.28.

Kaplan–Meier curves of overall survival according to tumor recurrence status. Log-rank test: p = 0.0001.
Discussion
Malignant PCWTs characterize a rare and anatomically unique group of tumors. The majority of large case series are restricted to a few specialized referral centers with significant experience in undertaking complex wide reconstruction of these tumors. To date, this study represents the largest single-center case series of patients with malignant PCWT, all of whom received wide resection for curative intent under a single surgeon. Median OS was comparable to that reported by other studies, 3,5,7,14,16 as were frequently reported postoperative complications such as wound infection. 6,14,17 Although recurrence was independently associated with decreased OS, pathology grade, achievement of negative margins, and other patient and tumor characteristics were not associated with OS.
Our study population demonstrated an eclectic group of these malignant chest wall tumors. While chondrosarcomas are known to be the most common primary malignant chest wall tumor, only nine patients in this series demonstrated chondrosarcoma. In contrast, pleomorphic sarcoma and liposarcomas were more prevalent in our study population, and limited data are available on consecutive series of these tumor types. 9 This heterogeneity accounts for differences in the demographics reported in our case series compared to the literature. While we reported a similar age distribution centering on the sixth decade of life, 3,11,18 –20 we noted a male gender predisposition, which is reported in many case series with chondrosarcoma patients. 4,7,8 Although reporting bias must be considered in the comparison of descriptive statistics between studies, male gender is predominant with many PCWT types including liposarcoma and malignant fibrous histiocytoma, as in our series. 9 In contrast, studies with a more heterogenous group of PCWTs 6,17 or benign tumor types 3,21 report more similar representation between genders.
Local or distant tumor recurrence was 50% in this case series and associated with a significantly shorter OS and deceased status at the time of follow-up, findings which are reported in several previous case series. 4 –6,17 Previously reported data describe grade as an independent risk factor for survival. 4,5,7 –9,21 Widhe et al. demonstrated that high-grade, intralesional margins and treatment at a non-specialty center were predictive for recurrence. 4 However, there was no statistically significant difference in OS between patients with low/intermediate-grade versus high-grade tumors after initial surgical resection, given the heterogenous group of diagnoses and the absence of a grading system for several of the exceeding rare tumor diagnoses. Furthermore, achievements of a negative (i.e. R0) margin are associated with disease-free status at follow-up. For example, King et al. found a higher 5-year recurrence rate with 2-cm margins compared to patients with 4-cm resection margins. 5 Rahman et al. similarly found that tumor type and absence of negative margins predicted higher recurrence. 6 In the present study, less than three of the four procedures achieved negative surgical margins. True negative margins are harder to obtain due to anatomical constraints, limiting wider resection of chest wall resections, such as the thin pleura. In addition, tumor location and the behavior of specific tumors affect recurrence rate, with chondrosarcomas consistently associated with greater recurrence-free survival. 4,5,10,11,22
OS, including 5- and 10-year OS rates, was similar to that of previously reported studies and significantly shorter in patients who experienced local or distal recurrence after initial resection compared to patients without any recurrence. 7,9,16,17 Friesenbichler et al. report a slightly higher OS (74.2%) at both 5 and 10 years. 8 However, their study focused on low-grade chondrosarcomas and included several procedures limited to intralesional incisions. Previous studies with a focus on wide resection have also included patients with benign tumors, while we solely focused on malignant tumors. 3 Additional factors that can influence outcome include any pulmonary resection (and sequelae including continued postoperative ventilatory support) as part of the original operation, a factor that was not present in the included patient cohort.
We acknowledge certain study limitations, including those inherent to a retrospective, single-center case series with a relatively limited number of patients. Heterogeneity of tumor diagnoses, along with a significant proportion of patients with indeterminate tumor grades, confounded potential associations with long-term outcomes. In addition, we were unable to accurately determine event date (e.g. recurrence and death) and therefore could not calculate event-free survival for this study cohort.
Conclusions
In spite of limitations imposed by a heterogenous group of diagnoses, a single-center, single-surgeon experience with wide surgical resection of malignant PCWT demonstrates long-term outcomes comparable to those previously reported. Although recurrence is associated with decreased OS, recurrence likely varies among individual tumor types.
Supplemental material
838296_Supplementary_Tables - Overall survival and tumor recurrence after surgical resection for primary malignant chest wall tumors: a single-center, single-surgeon experience
838296_Supplementary_Tables for Overall survival and tumor recurrence after surgical resection for primary malignant chest wall tumors: a single-center, single-surgeon experience by Aalap C Shah, Kazimierz W Komperda, Arun A Mavanur, Steven W Thorpe, Kurt R Weiss, and Mark A Goodman in Journal of Orthopaedic Surgery
Footnotes
Data availability
The de-identified patient data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Aalap C Shah is Founder and Principal of PRPmobile LLC; Paid Blogger/Writer at Doximity, Medical Advisory Board Member at SureConsent LLC. All other authors have no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was performed as part of a medical student rotation and under the mentorship of academic faculty employed by the University of Pittsburgh School of Medicine and the University of Pittsburgh Department of Orthopedic Surgery.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.