
Abstract
Background:
This retrospective cohort study aimed to investigate whether simple routine blood tests at presentation (C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), alkaline phosphatase and albumin) predict survival in patients with osteosarcoma.
Methods:
Between January 1998 and February 2015, 134 patients with a histological diagnosis of osteosarcoma were treated in our unit. Of these, 79 patients with high-grade osteosarcomas were included in the study. Demographic and clinical data, and laboratory parameters obtained prior to biopsy (CRP, ESR, alkaline phosphatase and albumin levels), were obtained from patients’ records.
Results:
There were 44 males and 35 females. Univariate analysis showed that high pre-biopsy CRP (p = 0.004), raised pre-biopsy ESR (p = 0.010), older age (p < 0.001), poor tumour necrosis rates (≤90%, p = 0.023) and metastasis at presentation (p < 0.001) were poor prognostic factors. Multivariate analysis showed pre-biopsy CRP and ESR levels to be independent predictors of overall survival (p = 0.020 and p = 0.025, respectively). Kaplan–Meier survival was significantly lower in patients with elevated CRP (p = 0.002) and ESR (p = 0.003). Hypoalbuminaemia and elevated alkaline phosphatase levels did not correlate with overall survival.
Conclusion:
Preoperative CRP and ESR levels may have value in building a prognostic model for patients presenting with osteosarcoma.
Background
Osteosarcoma is the most common primary malignant bone tumour. 1,2 Accurate staging is important to guide therapy, and in recent years, there has been an emphasis on developing and identifying new biomarkers associated with treatment response and prognosis. Many of these proposed biomarkers are novel and include, for example, microRNA evaluation. 3 –5 However, it is clear that some existing routine diagnostic blood tests may have value as biomarkers, including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), alkaline phosphatase and albumin; the measurement of which is simple, rapid, and cost-effective.
CRP is an acute phase protein, which is predominantly produced by hepatocytes. A high-serum CRP level is an indicator of a poorer prognosis in many cancers, including breast cancer, colorectal cancer and gastrointestinal cancer. 6 –8 Patients with other diseases such as type 2 diabetes, cardiovascular disease and arthritis may develop high CRP levels. 9 –11 Both tumour growth and host response to tumour growth can result in tissue inflammation, leading to an elevated CRP.
ESR is a classic inflammatory marker that constitutes one of the oldest laboratory measurements. ESR can often be elevated in cases of infection, malignancy and autoimmune disease. 12 –14 It also has clinical significance in the follow-up and prognosis of noninflammatory conditions such as prostate cancer 15 and coronary artery disease. 16 Alkaline phosphatase is primarily secreted by the liver and the bone, although a small amount is also secreted by intestine, kidneys and leukocytes. 17 Serum alkaline phosphatase level is usually greater in children than in adults 18 due to osteoblast activity at the growth plates. It can therefore be considered to have some disease specificity in the context of osteosarcoma.
Increased albumin degradation rates have been documented in patients with chronic inflammation. 19 Hypoalbuminaemia has been reported to have prognostic value in prostate cancer. 20 Tumour necrosis factor (TNF) and interleukin 6 (IL-6) are known to downregulate albumin synthesis and increase acute-phase protein production in hepatocytes. 21
This retrospective cohort study aimed to investigate whether routine blood tests (CRP, ESR, alkaline phosphatase and albumin) predicted overall survival in patients with osteosarcoma (Figures 1, 2, 3, 4). We wanted to evaluate whether these tests could serve as useful benchmarks with which to compare novel disease-specific biomarkers and whether they should be included in a prognostic model.

Kaplan–Meier curve for overall survival of patients with osteosarcoma according to serum CRP levels. High CRP taken as over 5 mg/mL correlates with decreased survival (p = 0.002), n = 70. CRP: C-reactive protein.
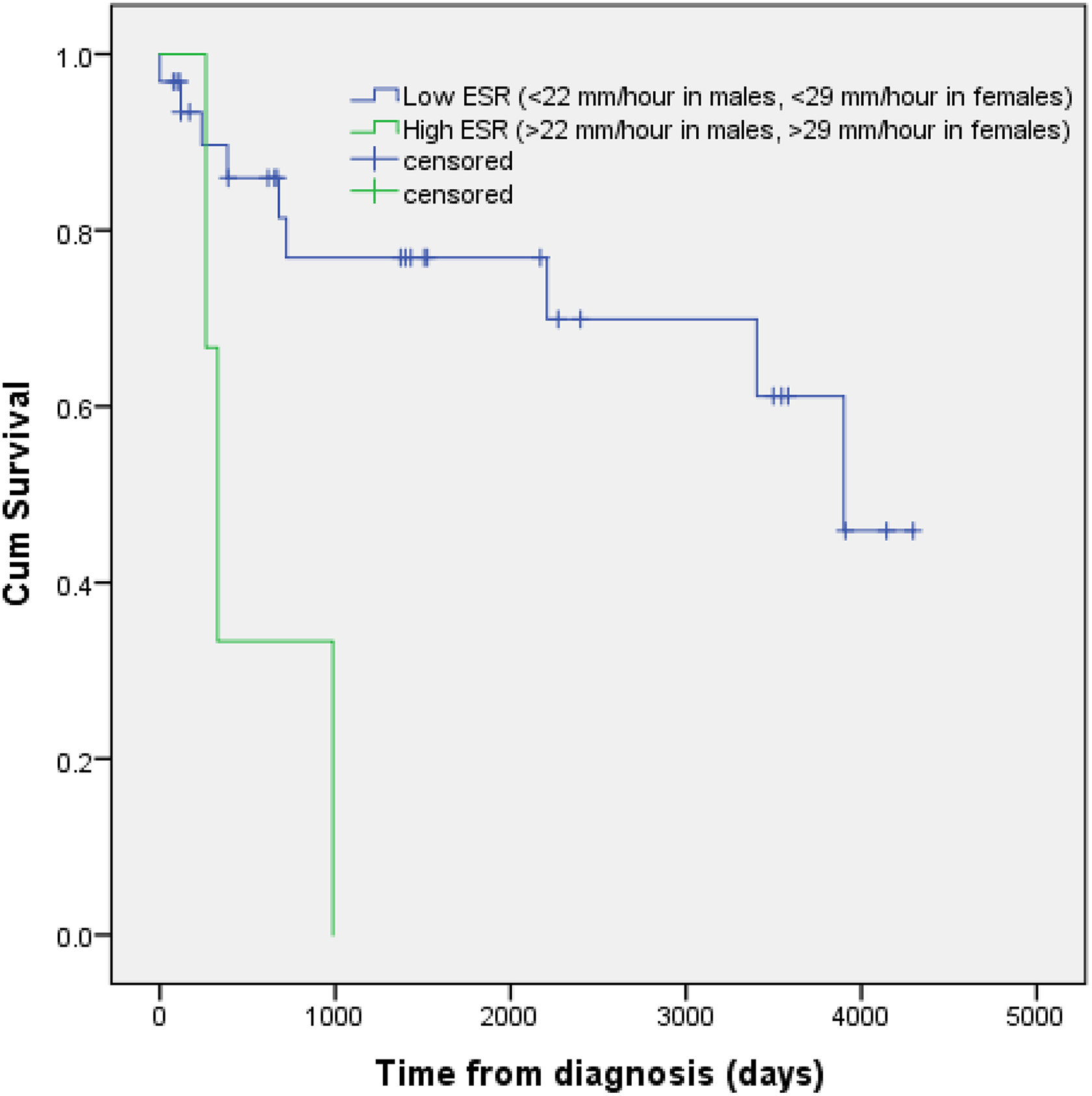
Kaplan–Meier curve for overall survival of patients with osteosarcoma according to ESR levels. High ESR correlates with decreased survival (p = 0.003), n = 40. ESR: erythrocyte sedimentation rate.

Kaplan–Meier curve for overall survival of patients with osteosarcoma according to serum alkaline phosphatase levels. There was no correlation between alkaline phosphatase levels and survival (p = 0.417), n = 78.

Kaplan–Meier curve for overall survival of patients with osteosarcoma according to serum albumin levels. There was no correlation of albumin with survival (p = 0.539), n = 79.
Methods
Study design and patients
Between January 1998 and February 2015, 134 patients with a histological diagnosis of an osteosarcoma were treated at our centre. Demographic data including age, sex, tumour site, stage, grade, metastases at presentation and the results of blood tests prior to any therapy were obtained from clinical records. The tumour necrosis rate after chemotherapy was defined as poor if ≤90% or good if >90% on histological assessment.
Patients were excluded from this retrospective cohort study because of incomplete clinical data in 37 cases and 18 cases with low or unknown grade of osteosarcoma. All 79 patients had an alkaline phosphatase level available. Albumin was unavailable for 1 patient, CRP was unavailable for 9 patients and ESR was unavailable for 39 patients.
Overall survival was the primary endpoint in this study; this was defined as the period from diagnosis to death. Patients were treated within a multidisciplinary team according to best practice at the time of presentation, in recent years as per the British Sarcoma Group guidelines. 22
Blood tests
CRP, alkaline phosphatase and albumin assays pre-biopsy were measured as part of a routine biochemical examination. During the period of the study, the biochemistry laboratory used different machines: Olympus AU, Roche Modular P and Roche Cobas c702 autoanalyser, which was introduced in 2010. While there would be slight variation in measurement accuracy this would not be at a level that would affect the overall results. The following methods were used for the respective analytes, serum albumin: spectrophotometric method using bromocresol green, serum ALP: spectrophotometric method using p-nitrophenyl phosphate and serum CRP: particle-enhanced immunoturbidimetric assay. A high-serum CRP level was defined as >5 mg/L, high alkaline phosphatase was taken as >110 U/L in adults and >150 U/L in children, low albumin as <40 g/L. ESR was measured using the Starrsed RL analyser, a high ESR was defined as >22 mm/h in males and >29 mm/h in females.
Statistical analysis
Analyses were performed to assess the relationships between CRP, ESR, alkaline phosphatase and albumin levels, baseline clinical factors, tumour necrosis rates and overall survival of the patients. Kaplan–Meier survival curves were used to estimate the overall survival in patients grouped according to high or low values of CRP, ESR, alkaline phosphatase and albumin at presentation. The log-rank test was used to compare overall survival of the patients. A multivariate analysis was performed using a Cox proportional hazard model with significant blood tests identified in the univariate analysis as variables. A value of p < 0.05 was considered to be significant in all statistical analyses. Calculations were made using IBM SPSS Statistics for Windows, version 24, 2016 (IBM Corp., Armonk, New York, USA).
Results
The demographic details are given in Table 1. The mean follow-up was 45 months (1–172). The primary sites for tumour were the extremity in 64 cases, pelvis in 1 case, spine in 4 cases, head in 6 cases and trunk in 4 cases.
Baseline patient characteristics.

Discussion
We investigated the role of routine blood tests in predicting clinical outcomes in patients with high-grade osteosarcoma (Table 2). Our finding of an association between an elevated CRP and worse overall survival is consistent with previous observations in many other malignancies. Immune cells responding to inflammation produce cytokines, particularly IL-6, which in turn induces transcription and subsequent production of CRP from hepatocytes. 23 –25 In patients with osteosarcoma, Nakamura et al. 26 reported that an elevated CRP was an adverse prognostic factor for local tumour control but did not affect the disease-specific survival. However, they found that a raised CRP was an adverse prognostic factor for disease-specific survival in chondrosarcoma and Ewing’s sarcoma. Our data corroborate with Funovics et al. 27 who showed that in patients with high-grade osteosarcoma, preoperative CRP levels, that is, after biopsy but before tumour resection correlate with disease-specific outcome. Our patients had blood tests prior to biopsy, and therefore there were no confounding variables relating to prior invasive procedures.
Univariate analysis of prognostic factors for overall survival.a
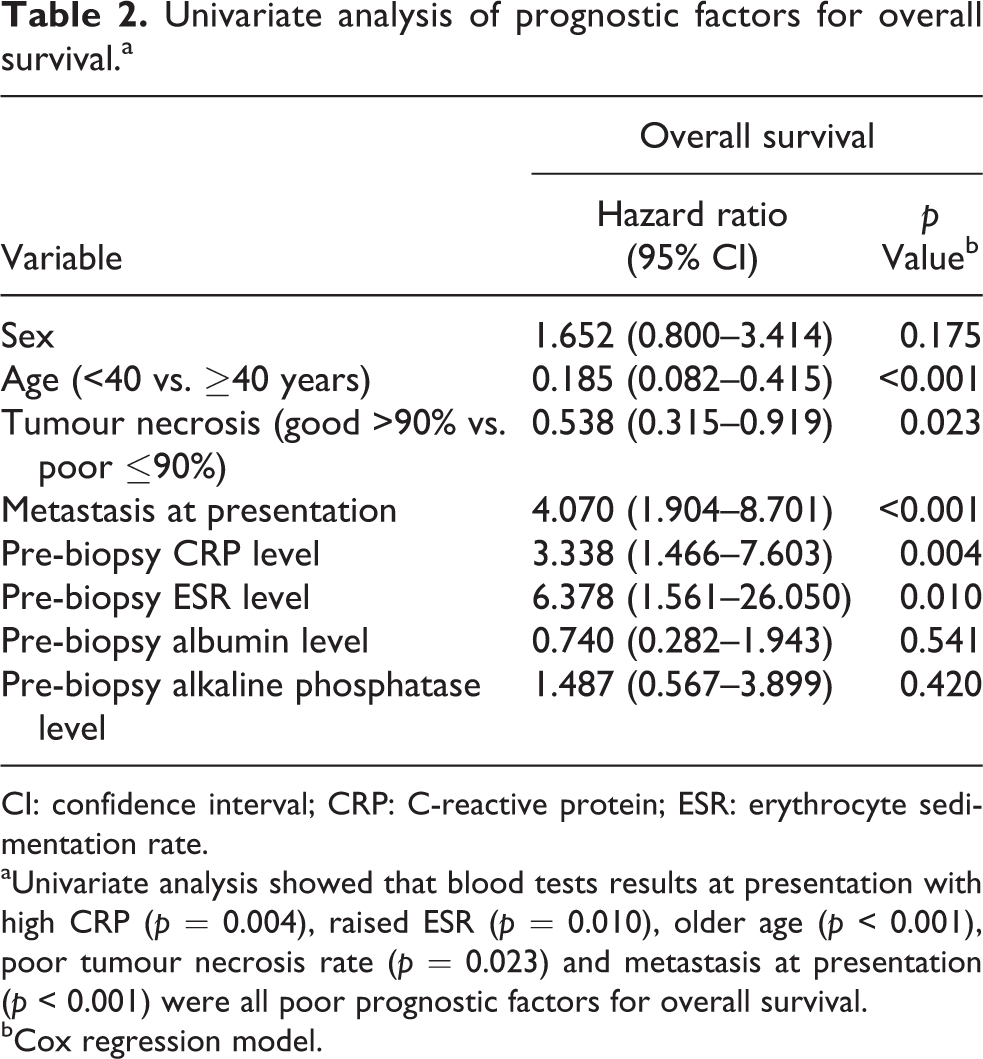
CI: confidence interval; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.
aUnivariate analysis showed that blood tests results at presentation with high CRP (p = 0.004), raised ESR (p = 0.010), older age (p < 0.001), poor tumour necrosis rate (p = 0.023) and metastasis at presentation (p < 0.001) were all poor prognostic factors for overall survival.
bCox regression model.
Alkaline phosphatase can be regarded as a marker of bone turnover. A meta-analysis by Ren et al. concluded that a high-serum alkaline phosphatase level is associated with poor overall survival in osteosarcoma patients. 28 Cultured human osteosarcoma cell lines 29,30 have been shown to produce large amount of alkaline phosphatase, and serum levels have been shown to be significantly elevated in patients with osteoblastic osteosarcoma subtypes. 31 There are reports of patients presenting with an initial raised serum alkaline phosphatase that return to normal levels after preoperative chemotherapy, 32 however in an international multicentre study involving 2680 patients with osteosarcoma, Pakos et al. 33 reported that serum alkaline phosphatase was not a prognostic factor in terms of disease outcome. Likewise, raised alkaline phosphatase levels did not correlate with overall survival in our study and this may be due to the wide range of values that are produced when alkaline phosphatase is measured.
Regarding clinical factors, metastases at presentation, age, 34,35 tumour location, 33 size 36 and chemotherapy-induced necrosis 33 have been reported as important prognostic factors in osteosarcoma. We found older age (>40 years) to be an adverse prognostic factor, while tumour necrosis was significant in the univariate analysis but not the multivariate. Some studies have also not clearly demonstrated the correlation of tumour necrosis with survival in osteosarcoma patients. 37,38 Kim et al. 39 reported that tumour necrosis rate adjusted by tumour volume change was a better predictor of survival in osteosarcoma patients. In our series, CRP and ESR have out-performed tumour necrosis rate in the multivariate analysis indicating that they are useful to document as an indicator of prognosis (Table 3).
Multivariate analysis for prognostic factors for survival.a
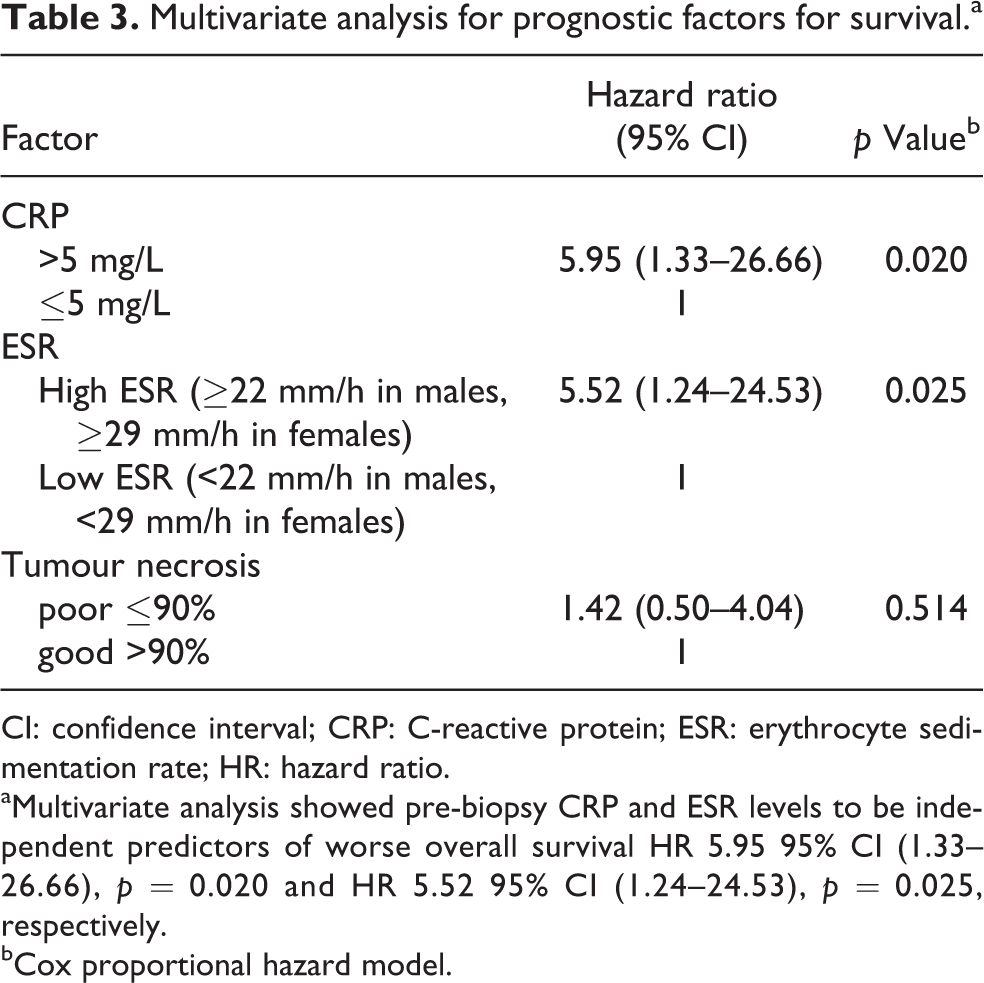
CI: confidence interval; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; HR: hazard ratio.
aMultivariate analysis showed pre-biopsy CRP and ESR levels to be independent predictors of worse overall survival HR 5.95 95% CI (1.33–26.66), p = 0.020 and HR 5.52 95% CI (1.24–24.53), p = 0.025, respectively.
bCox proportional hazard model.
Research into circulating disease-specific biomarkers for osteosarcoma has increased markedly in recent years. MicroRNAs in particular 3 –5 have received attention and there are ongoing studies assessing circulating free tumour DNA and intact circulating tumour cells. The attraction of these novel biomarkers is not only the potential for correlation with clinical outcomes but also the potential to indicate additional therapeutic options for the patient. However, to date none of these newer biomarkers have made it into the clinical arena. It is important therefore that groups researching novel biomarkers compare the performance with readily available laboratory values such as CRP and ESR in terms of correlation with clinical outcomes. Moreover, the development of algorithms which include all of these markers is proving effective in other solid cancers. 40
The strength of our study is that CRP and ESR remain useful markers despite the heterogeneity of our study population of osteosarcoma patients which has included a wide age range and various pathological subtypes. There are limitations of our study including its retrospective design and a small sample size from a single-centre experience. We did not consider the presence of other systemic conditions that could be associated with raised inflammatory markers. We did not have a sufficient number of patients to allow further risk stratification. We reported on the overall survival (Figure 5) rather than disease-specific survival because we did not have a specific cause of death.

Kaplan–Meier curve for overall survival of patients with osteosarcoma. The estimated 1-, 5- and 10-year overall survival was 0.802 (SE: 0.049), 0.549 (SE: 0.069) and 0.474 (SE: 0.078), respectively, n = 79. SE: standard error.
Conclusion
Elevated serum CRP and ESR are associated with worse overall survival in this group of osteosarcoma patients. We recommend the use of these routine blood markers to help identify patients at higher risk of mortality and to use as a benchmark to compare the novel disease-specific biomarkers currently being extensively investigated.
Footnotes
Authors’ contributions
PJ, GJST, CHG and KSR contributed to the conception, design, data analysis and interpretation. The authors helped to draft the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.