
Abstract
Background:
The purpose of this study was to compare the surgical outcomes of anterior decompression and fusion (ADF) with that of posterior laminoplasty (LAMP) for cervical myelopathy caused by ossification of posterior longitudinal ligament (OPLL).
Methods:
We retrospectively assessed the medical records of patients who underwent surgery for cervical myelopathy owing to OPLL between 2007 and 2016 at our institution. Fifty patients were included in this study, including 17 patients in ADF group and 33 patients in LAMP group. Surgical outcomes were assessed under the Japanese Orthopaedic Association (JOA) score. The radiologic and clinical data were compared between two groups.
Results:
There was no significant difference in age, follow-up time, operation time, blood loss, length of stay, preoperative JOA score, occupying ratio of OPLL, diameter of spinal canal, preoperative and final follow-up C2-C7 Cobb angles, and the change of C2-C7 Cobb angle before and after operation between ADF and LAMP groups. The final follow-up JOA score and the neurological recovery rate were significantly higher in ADF group than in LAMP group, particularly in patients with segmental-type OPLL. Cerebrospinal fluid leakage is a major complication after ADF, C5 paralysis, and axial pain frequently results from LAMP.
Conclusion:
Compared with LAMP, ADF shows better improvement of neurological function in patients with cervical myelopathy due to OPLL, especially in patients with segmental-type cervical OPLL.
Introduction
Ossification of posterior longitudinal ligament (OPLL) is a disease that is characterized by ectopic bone formation of the spinal ligament. It is most commonly found in Asian populations, especially in Japanese. 1,2 The spinal cord can be compressed due to progression of this lesion, which can cause neurological deficits. The most common location is at the cervical region of the spine, and OPLL has been considered to be a common cause of cervical myelopathy. 3,4 Conservative treatment is ineffective in relieving neurological symptoms and preventing the progression of ossification. Therefore, surgery is usually the recommended treatment option. 5
Many surgical procedures have been developed for treatment of cervical myelopathy due to OPLL, and surgery can be performed through anterior, posterior, or combined approaches. 6,7 Both anterior decompression and fusion (ADF) and laminoplasty (LAMP) are the widely used procedures in treating cervical OPLL. ADF can achieve direct decompression of spinal cord by the removal of ossified lesion and is in favor of restoring cervical spine alignment. However, ADF is technically demanding and associated with complications. 8 –11 LAMP can enlarge the available space around spinal cord and allow back shift of spinal cord, leading to indirect decompression of spinal cord. Although LAMP is low technically demanding, it increases the risk of local kyphotic deformity. Considerable controversy exists over the choice of surgical procedure for cervical myelopathy due to OPLL, ADF, 12 and LAMP. 13 –15 The authors have performed either ADF or LAMP for patients with OPLL. The purpose of this study was to compare the surgical outcomes between the two procedures for the treatment of cervical myelopathy caused by OPLL.
Materials and methods
Patient population
A total of 82 patients underwent surgery for cervical myelopathy due to OPLL between 2007 and 2016 at the authors’ hospital. Their medical records and data have been retrospectively reviewed. Patients were included if they met the following criteria: (1) cervical myelopathy due to cervical OPLL; (2) received surgical treatment with ADF or LAMP; (3) no trauma, infection, tumor, or previous surgery; (4) more than 18 years; and (5) had complete medical records. Patients were excluded if they met the following criteria: (1) did not complete minimum of 1 year of follow-up, (2) thoracic or lumbar OPLL, (3) yellow ligament ossified, (4) no contact information, and (5) death (not related to surgery). Of 82 patients, 32 were excluded owing to received anteroposterior surgery (n = 3), incomplete follow-up data (n = 8), cervical tumor (n = 1), thoracic or lumbar OPLL (n = 9), yellow ligament ossified (n = 5), or cervical disc herniation (n = 6). Finally, only 50 patients (17 patients underwent ADF, 33 patients underwent LAMP) were included in this study. The specific screening process was presented in Figure 1. This study has been approved by the authors’ institutional review board

Study sample flow chart. OPLL: ossification of posterior longitudinal ligament.
Clinical and radiographic assessment
Japanese Orthopaedic Association (JOA) scores (maximum points of 17) and recovery rates were used to assess clinical results. 16 Each participant’s JOA (preoperative, immediate postoperative, and final follow-up) was measured. The recovery rate (%) was measured by the following formula: (postoperative JOA score − preoperative JOA score)/(17 − preoperative JOA score).
On the basis of preoperative finding on standard lateral radiographs, the OPLL type was classified as mixed, continuous, segmental, and isolated 17 (Figure 2). The occupying ratio of OPLL in spinal canal and C2-C7 Cobb angle were used as radiographic parameters. The occupying ratio of OPLL was calculated using the following formula: the maximum anteroposterior thickness of OPLL divided by the anteroposterior diameter of the spinal canal at corresponding segment on a lateral radiographs. The C2-C7 Cobb angle was measured using the method described by Cobb (the angle of intersection between lines parallel to the inferior end plates of C2 and inferior endplate of C7). 18 The angle of ≥10° was recognized as lordosis, ≥−5° but <10° as straight and <−5° as kyphotic. 18

OPLL is divided into four types based on CT scan findings: (a) continuous-type, (b) segmental-type, (c) isolated-type, and (d) mixed-type. OPLL: ossification of posterior longitudinal ligament; CT: computed tomography.
Surgery treatment
Surgical procedure was selected based on individual patient. Patients with cervical OPLL involving less than three levels were treated with ADF procedure. Patients with cervical myelopathy due to OPLL involving more three levels were treated with LAMP procedure. The absolute bed rest time is 1–3 days after surgery. The duration of wearing neck collar is 8 weeks for patients with ADF and 2 weeks for individuals after LAMP.
Anterior surgery
ADF procedure was performed through a standard left-sided Robinson–Smith anterior approach (Figure 3). The base of the uncinate process or lateral border of the disc was used as a landmark for the width of the vertebral body. Subtotal corpectomy was executed at 1–3 levels as determined by the extent of neurologic involvement and reconstructed CT images. This was accompanied by total disectomy. When the posterior cortex of vertebra was exposed, we used a diamond burr to shave the cortex and ossified ligament, making the thickness of cortex and ossified ligament as uniform as possible. Ossified lesions were dissected completely if they could easily be released, but the partial removal of ossified lesion was performed if the lesions strongly adhered to the dura or the dura itself was ossified. The autologous bone was used for vertebral fusion in all patients along with the stability of anterior titanium plate.

A 31-year-old man presented with bilateral upper limb numbness. Preoperative imaging studies demonstrated that obvious OPLL at C5 level. After an anterior C5 corpectomy and fusion, he had a significant recovery. (a) Preoperative lateral radiograph demonstrated a lordosis in cervical spine. (b) Preoperative CT demonstrated compression of spinal cord anteriorly. (c) Preoperative T2-weighted MR image showed the obvious compression of spinal cord. (d) Postoperative lateral radiograph demonstrated C5 corpectomy and fusion. (e) Postoperative CT demonstrated sufficient decompression of spinal cord. OPLL: ossification of posterior longitudinal ligament; CT: computed tomography; MR: magnetic resonance.
Posterior surgery
In the LAMP procedure, single-door LAMP was performed through a standard posterior straight incision approach (Figure 4). The paravertebral muscles were detached from spinous processes on both sides. After the exposure of posterior elements, we used a piezosurgery to make bilateral gutters. One side was kept open using spacers; meanwhile, the other side was used as “door spindle.” Small bone chips made from partial C7 spinous process were inserted into the side of “door spindle.”
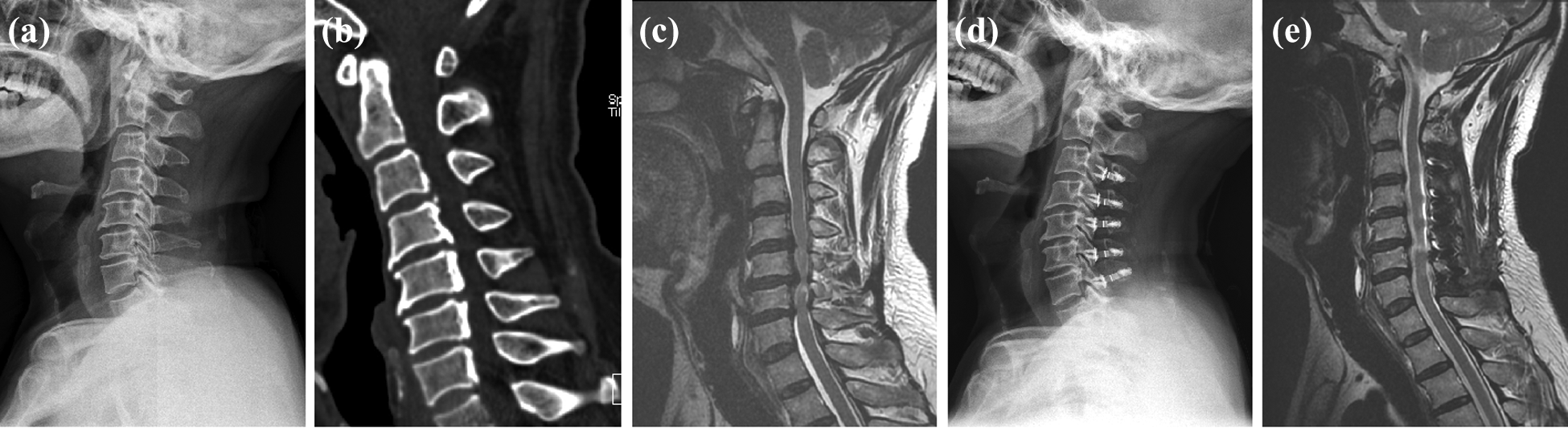
A 57-year-old man presented with bilateral upper limb numbness. After posterior C3-C7 laminoplasty, he had neurological function improvement. (a) and (d) Preoperative and postoperative lateral radiograph showed that no significant change was found in cervical alignment. (b) Preoperative CT showed obvious OPLL at C3-C7 levels. (c) Preoperative T2-weighted MR image demonstrated severe compression of spinal cord anteriorly. (e) Postoperative T2-weighted MR image showed the enlarge of spinal canal and the sufficiency of indirect decompression. CT: computed tomography; OPLL: ossification of posterior longitudinal ligament; MR: magnetic resonance.
Statistical analysis
For statistical analysis of outcomes, the independent t-test was performed using SPSS version 22.0. Significance was considered when p value < 0.05.
Ethics approval
The study was approved by the Medical Ethics Committee of the Nanfang Hospital, Southern Medical University, China.
Results
Patients’ demographics
There was no significant difference in age, follow-up time, operation time, blood loss, length of stay, preoperative JOA score, preoperative occupying ratio of OPLL, preoperative anteroposterior diameter of spinal canal, and preoperative C2-C7 Cobb angle between ADF and LAMP groups. However, the surgical segment in ADF group was less than that in the LAMP group (ADF: 1.2 ± 0.4 vs. LAMP: 4.1 ± 0.6, p < 0.05; Table 1).
Patient background and postoperative data.

ADF: anterior decompression and fusion; LAMP: laminoplasty; JOA: Japanese Orthopaedic Association; OPLL: ossification of posterior longitudinal ligament; SD: standard deviation.
OPLL was classified into four categories: continuous-type (ADF group = 2, LAMP group = 6), segmental-type (ADF group = 9, LAMP group = 13), mixed-type (ADF group = 0, LAMP group = 6), and isolated-type (ADF group = 6, LAMP group = 8). The preoperative cervical sagittal alignment was lordosis in 12 ADF patients and 17 LAMP patients and straight in 5 ADF patients and 16 LAMP patients. No patients had cervical kyphosis (unintentional exclusion) before surgery (Table 2).
Preoperative cervical alignment and type of OPLL.

OPLL: ossification of posterior longitudinal ligament; ADF: anterior decompression and fusion; LAMP: laminoplasty.
Clinical outcomes
The immediate postoperative JOA score was significantly higher in ADF group than in LAMP group (14.7 ± 1.2 vs. 13.6 ± 1.6, p = 0.014). The final follow-up JOA score after ADF procedure was higher than that of after LAMP procedure (15 ± 2.2 vs. 13.7 ± 1.9, p = 0.031). Compared with LAMP group, a better final follow-up recovery rate was found in ADF group (59.9 ± 33.8% vs. 35.8 ± 35.3%, p = 0.025; Table 1).
Radiologic outcomes
The decrease of cervical lordosis after surgery was observed by measuring the change of C2-C7 Cobb angle in two groups. The final follow-up C2-C7 Cobb angle wasn’t significantly different between ADF and LAMP groups (14.7 ± 7.3° vs. 10.2 ± 7.1°, p = 0.057). The change of C2-C7 Cobb angle was similar between two groups (−1.3 ± 6.2° vs. −1.9 ± 6.4°, p = 0.736; Table 1).
Complications
Complications in the ADF group included cerebrospinal fluid (CSF) leakage in two patients, dysphagia in one patient and surgical site infection in one patient (Table 3). CSF leakage developed because of dural tear which was attributed to the dural ossification or severe adhesion with epidural surface during the operation. After the surgery, the drainage tube was placed for 1–2 days and local constant pressure to wound was conducted. Generally, CSF leak stopped after approximately 3–5 days after conservative treatment. Recovery also be achieved in this patient with dysphagia or surgical site infection after symptomatic treatment.
Summary of surgical complications after ADF and LAMP.
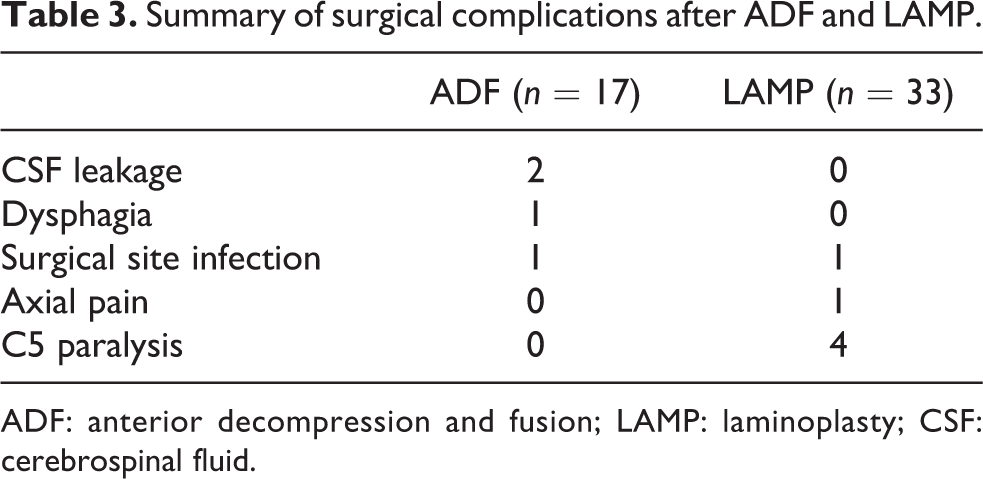
ADF: anterior decompression and fusion; LAMP: laminoplasty; CSF: cerebrospinal fluid.
In this LAMP group, four patients had C5 paralysis, one had axial pain, and one had surgical site infection (Table 3). Of four patients with C5 paralysis, one C5 paralysis patient required revision surgery owing to the declining strength of deltoid muscle, who achieved full recovery after revision surgery. The C5 paralysis of the remaining three patients and other complications were resolved by conservative therapy.
Surgical outcomes of ADF and LAMP on basis of the OPLL type
For continuous-type OPLL, the immediate postoperative JOA score (15.5 ± 0.7 vs. 13 ± 1.5, p = 0.078), final follow-up JOA score (15.5 ± 0.7 vs. 14.5 ± 1.6, p = 0.453), and final follow-up recovery rate (54.2 ± 29.5% vs. 56.8 ± 27.9%, p = 0.913) all showed no significant difference between ADF and LAMP groups. For segmental-type OPLL, no significant difference was found in immediate postoperative JOA score between two groups, but a higher final follow-up JOA score (15.2 ± 1.3 vs. 13.5 ± 1.3, p = 0.007) and recovery rate (65.1 ± 24.4% vs. 28.2 ± 27.3%, p = 0.004) were found in ADF group compared with LAMP group. For isolated-type OPLL, the immediate postoperative JOA score (14.7 ± 1.5 vs. 13.6 ± 1.5, p = 0.224), final follow-up JOA score (14.5 ± 3.4 vs. 13.6 ± 3, p = 0.62), and final follow-up recovery rate (53.9 ± 49.2% vs. 39.1 ± 51.2%, p = 0.611) all were similar between ADF and LAMP groups. The above information is summarized in Table 4.
Surgical outcomes of ADF and LAMP on basis of the type of OPLL.
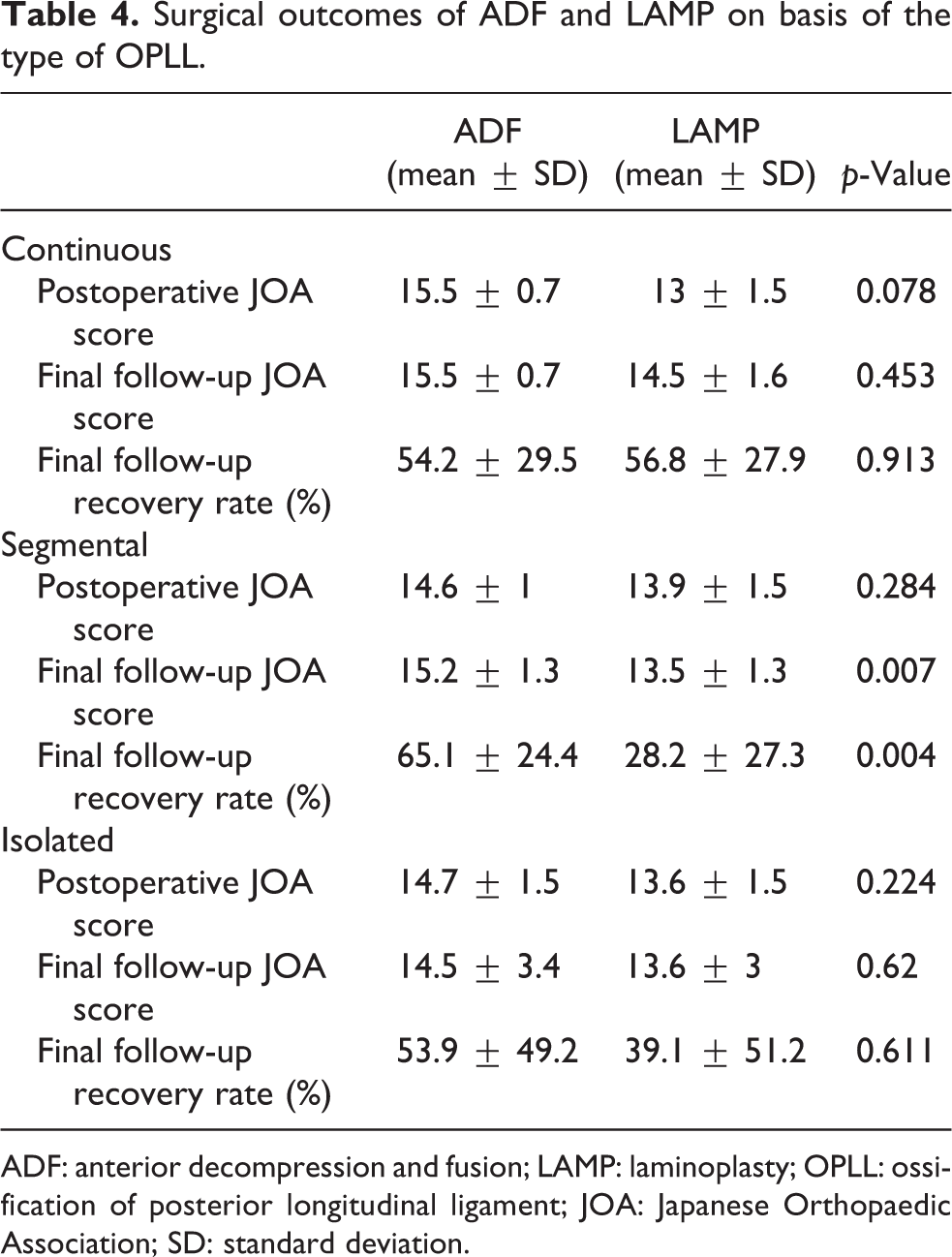
ADF: anterior decompression and fusion; LAMP: laminoplasty; OPLL: ossification of posterior longitudinal ligament; JOA: Japanese Orthopaedic Association; SD: standard deviation.
Discussion
Cervical OPLL has been known to be one of the common causes of cervical myelopathy among the Asian population. 1,3,4 No conservative treatment has been confirmed to be effective for this disease, surgical treatment is usually established. The aim of surgical treatment for cervical OPLL is to relieve the compression of spinal cord and nerve roots and achieve the stability of vertebral body at lesion area. Therefore, the surgical options should take the location and type of OPLL into consideration. LAMP provides indirect decompression by shifting the spinal cord posteriorly. If OPLL patients had postoperative worsening of cervical alignment, the spinal cord is less likely to shift posteriorly after posterior LAMP, resulting in late neurologic deterioration. Some studies have reported segmental-type OPLL are more likely to develop postoperative kyphosis and induce late neurologic deterioration than other types OPLL after posterior LAMP. 19 Therefore, ADF is often indicated in segmental-type OPLL rather than other types of OPLL. 5 The present study indicated that, compared with LAMP, ADF had a better neurological recovery for treating cervical myelopathy owing to OPLL, especially in patients with segmental-type cervical OPLL.
LAMP provides indirect decompression by a posterior shift of spinal cord caused by the enlargement of spinal canal. However, postoperative progression of kyphotic deformity after LAMP often lead to inadequate spinal shift and late neurological deterioration. 20 Some studies have reported that the cervical spinal cord is stretched 10–20% more in a flexed position than in extended position. 21,22 The healthy cord possesses an elasticity against deformity caused by cervical flexion or extension. 21,22 The degenerated spinal cord, however, may lose such feature and become vulnerable to such dynamic factor. Different from other types of OPLL, a good range of motion (ROM) of cervical spine was maintained for a long time in patients with segmental-type OPLL after LAMP. 19 This may lead to the repetitive deformity of cervical spinal cord and facilitate the development of late neurologic deterioration. With regard to anterior surgery, ADF offers a direct decompression of the spinal cord by removing ossified substance and maintains the stability and proper ROM of cervical spine, which can relieve the dynamic stress on degenerated spinal cord. Recent studies have reported that, compared with ADF, LAMP is more likely to develop cervical kyphosis and has a higher risk of late deterioration. 23 –25 In the present study, our results showed that ADF was superior to LAMP in neurological recovery, especially in patients with segmental-type OPLL.
In the current study, operation duration and blood loss were all similar between ADF and LAMP group. Theoretically speaking, anterior surgery has high technique demanding and need to complete the fusion of bone grafting in the area where the vertebral body was resected, which may require longer operation time and result in larger blood loss. However, when multiple cervical spine is included in the exposed area of posterior surgery, where the venous plexus is highly developed, increasing exposure time and blood loss. But, previous studies have shown opposite results to our study, that compared with LAMP, ADF had longer operation time and larger blood loss. 26 –28 Therefore, further study with long follow-up, large-size, and high-quality random trials should be performed to verify our results.
Limitations
There are some limitations in this study. First, it is a retrospective study at a single institution, which to some extent limited the evidence level. Although this study formulated strict inclusion criteria and detailed measurement of outcome indicators, the inherent evidence defect of retrospective study could not be nullified. Second, due to the lack of sufficient data, it could not confirm the relationship between cervical dynamic factors such as cervical ROM and K-line and surgical results in treatment of cervical myelopathy due to OPLL. Third, the number of involved segment was different between ADF and LAMP groups, which probably induces bias in this study. Fourth, the number of included patients with segmental-type OPLL was small in our study. This may induce result bias, which means that some patients who had bad neurological outcomes after surgery probably were missed.
Conclusion
In summary, this study indicated that, compared with LAMP, ADF is associated with better neurological improvement in treatment of cervical myelopathy caused by OPLL, especially for patients with segmental-type OPLL. Additional prospective study with high-quality, long follow-up, and large-size is needed to confirm this conclusion.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or immediate family has no funding or commercial associations (e.g. consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.