
Abstract
Purpose:
Dysphagia due to anterior cervical osteophytes is a rare condition. However, it can become serious enough to permanently impair the quality of life up to making normal food intake impossible. If conservative treatment fails, there is the option of surgical resection of the osteophytes. The objective of this study was to assess the outcomes of resections of anterior cervical osteophytes causing spondylogenic dysphagia, taking literature into consideration.
Method:
Resection of anterior cervical osteophytes using a standard anterior approach was performed in 14 consecutive patients with spondylogenic dysphagia between 2009 and 2015. Indomethacin or radiation was used to prevent recurrence. Imaging and clinical data were collected in follow-up examinations over an average of 50 months.
Results:
The osteophytes were sufficiently resected in all cases. Anterior plates were placed in three patients due to pronounced segmental mobility. Five patients were given recurrence prevention in the form of indomethacin, nine with radiation. One patient required revision surgery for a hematoma. No other serious complications were observed. All patients had significant improvement of their symptoms. No recurrences or signs of increasing instability were found during the follow-up period.
Conclusion:
When conservative treatment fails, surgical resection of cervical osteophytes is a sufficient method for treating spondylogenic dysphagia. High patient satisfaction and improvement of the quality of life are achieved with a low complication rate. Routine additional stabilization has been discussed as recurrence prevention. Prophylaxis using indomethacin or radiation, known primarily from hip replacement, also appears to be an option.
Introduction
Cervical anterior osteophytes have a prevalence of 20–30% among the elderly. Large symptomatic osteophytes usually develop in the context of ankylosing hyperostosis, first known as Forestier’s disease, and later diffuse idiopathic skeletal hyperostosis (DISH). They are systemic and are defined by radiological criteria. 1 –3 DISH is a rare disease and is a noninflammatory condition. 3 –9 By contrast, in inflammatory axial spondyloarthritis, similar osteophytes usually also involve the sacroiliac joint. 4
If anterior cervical osteophytes are symptomatic, symptoms can occur due to compression of neural or soft tissue structures. 10 –15 One of the main symptoms is dysphagia. 16,17 Its primary cause is structural from direct compression of the esophagus, 2,18 but a secondary cause can also be inflammation of the adjacent soft tissue, for example. 4,19 –23 In an advanced stage, malnutrition and weight loss are possible. 4,22,23
When the extrinsic cause of the compression is the most prominent, surgical resection of the osteophytes via a standard anterior approach can be performed for more severe conditions and impairment of the quality of life. 4,24 –28 The results are less satisfactory the more the changes in the esophagus itself have progressed. 4,29
The resection of the osteophytes does not eliminate the underlying disease, so new ossification can develop. 4,17,29 –31 Therefore, routinely performed additional fusion is discussed not only due to potential surgery-induced instability, but also because segmental mobility can promote the development of osteophytes. 9,29 –31 Experience in the prevention of ossification after surgery is available in particular for hip replacement surgery, where the administration of indomethacin 26,32,33 and radiation 34,35 has been established as a preventive measure.
The objective of this study was to evaluate the results of patients with anterior resection of cervical osteophytes due to spondylogenic dysphagia, taking literature into consideration.
Materials and methods
Patient characteristics
The routinely collected prospective data of all anterior operations of the cervical spine were analyzed retrospectively. The research protocol for this study has been reviewed by the Hospital Institutional Review Board. A specific patient consent was not required regarding the federal data privacy act because this retrospective study is based on intradepartmental medical records. The study included 14 consecutive patients who underwent resection of cervical anterior osteophytes due to spondylogenic dysphagia via a standard anterior approach between 2009 and 2015. The patient characteristics are presented in Table 1.
Patient characteristics.

DISH: diffuse idiopathic skeletal hyperostosis; Ø: average.
Inclusion criteria
The following were the criteria for the indication for surgery: progressive or chronic dysphagia >3 months; anterior cervical osteophytes in imaging (X-ray, computed tomography (CT), magnetic resonance imaging (MRI)) with compression of the cervical soft tissues (Figures 1(a) and (b) and 2); compression in the barium swallow test; exclusion of differential diagnoses (neurological, internal medical, ENT, etc.); no abnormal findings in esophageal function diagnostics; prior conservative treatment.
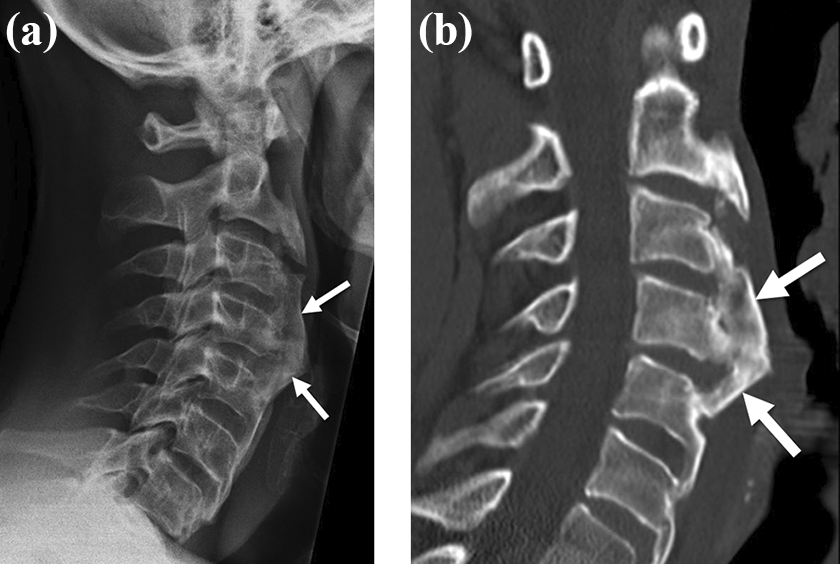
(a and b) Preoperative lateral X-ray image and sagittal CT reconstruction with anterior cervical osteophytes (arrows). CT: computed tomography.

Preoperative transversal CT reconstruction of the osteophyte (arrow) with compression of the cervical soft tissues (large asterisk) and original anterior edge of the vertebral body (small asterisks). CT: computed tomography.
Surgical technique and procedure
The operation was performed in the known standardized technique using a left approach along the sternocleidomastoid muscle under general anesthesia in a supine position. The head was rotated slightly to the right and fixated in a Mayfield head clamp. The anterior spine was visualized to the appropriate extent after blunt preparation between the neurovascular bundle and viscera and after bilateral resection of the longus colli muscle. The osteophytes were resected primarily with a high-speed diamond drill up to the original anterior edge of the vertebral body (Figure 3(a) and (b)). An attempt was made to preserve the integrity of the anterior annulus of the disc. Sufficient resection was checked using intraoperative fluoroscopy. Additional stabilization (plate) and/or fusion (cage) was performed only if segmental instability was determined intraoperatively.

(a) Intraoperative view with anterior osteophytes (asterisks). (b) Intraoperative view of the original anterior edge of the vertebral bodies after resection of the osteophytes.
All patients up to age 55 were given indomethacin 50 mg twice daily for 10 days with gastric protection directly postoperatively as prophylaxis against the recurrence of osteophytes. If NSAIDs were contraindicated in the patient history or if the patients were older than 55, fractionated radiation with five doses of 2 Gray was given. Radiotherapy was started on the first postoperative day and was continued at intervals of 4 days. All patients were provided with a semirigid brace for 6 weeks. If necessary, speech therapy was started.
Follow-up and analysis
The data were collected routinely pre- and postoperatively, after 6 weeks, and then annually. The patients came to follow-up in person. In addition to clinical and if applicable, imaging parameters, the Functional Outcome Swallowing Scale (FOSS), 36 the Prosiegel deglutition disorder scale, 37 and the dysphagia numeric rating scale (NRS; 0 = swallowing not impaired, 10 = swallowing impossible) were used to determine the severity of dysphagia. Preoperatively, postoperatively, and in the follow-up examinations, X-rays, MRI, and CT scans were conducted, depending on the findings. All 14 patients were available to follow-up. The Wilcoxon test and the Mann–Whitney U test were applied for comparison of preoperative and postoperative global results, and for comparison of results in the groups at different times. McNemar’s test was used to compare characteristics. Depending on the group characteristics, the descriptive assessments and analytical statistics were performed with the SPSS program package. A positive significance level was assumed at p < 0.05.
Results
Operative technique
The osteophytes were sufficiently resected in all cases. In four cases, the resection extended caudally up to C1. Even if the osteophytes extended further into the cervical spine, this did not result in additional compression. The slight rotation of the head to the contralateral side within the range of motion of the atlantoaxial joint allowed easy access to the axis. In one case, adhesions were found between the esophagus and the osteophytes. It proved helpful to use the C-arm to check for complete resection up to the original anterior edge of the vertebral body because the purely visual check of the site was not always conclusive. In three patients, the anterior segment of the annulus was also damaged following resection of the osteophytes. Intraoperatively, significant hypermobility in the sense of segmental instability was found, so the decision to use anterior plates was made. In one patient, the anterior annulus was opened so a cage was implanted for additional intervertebral fusion.
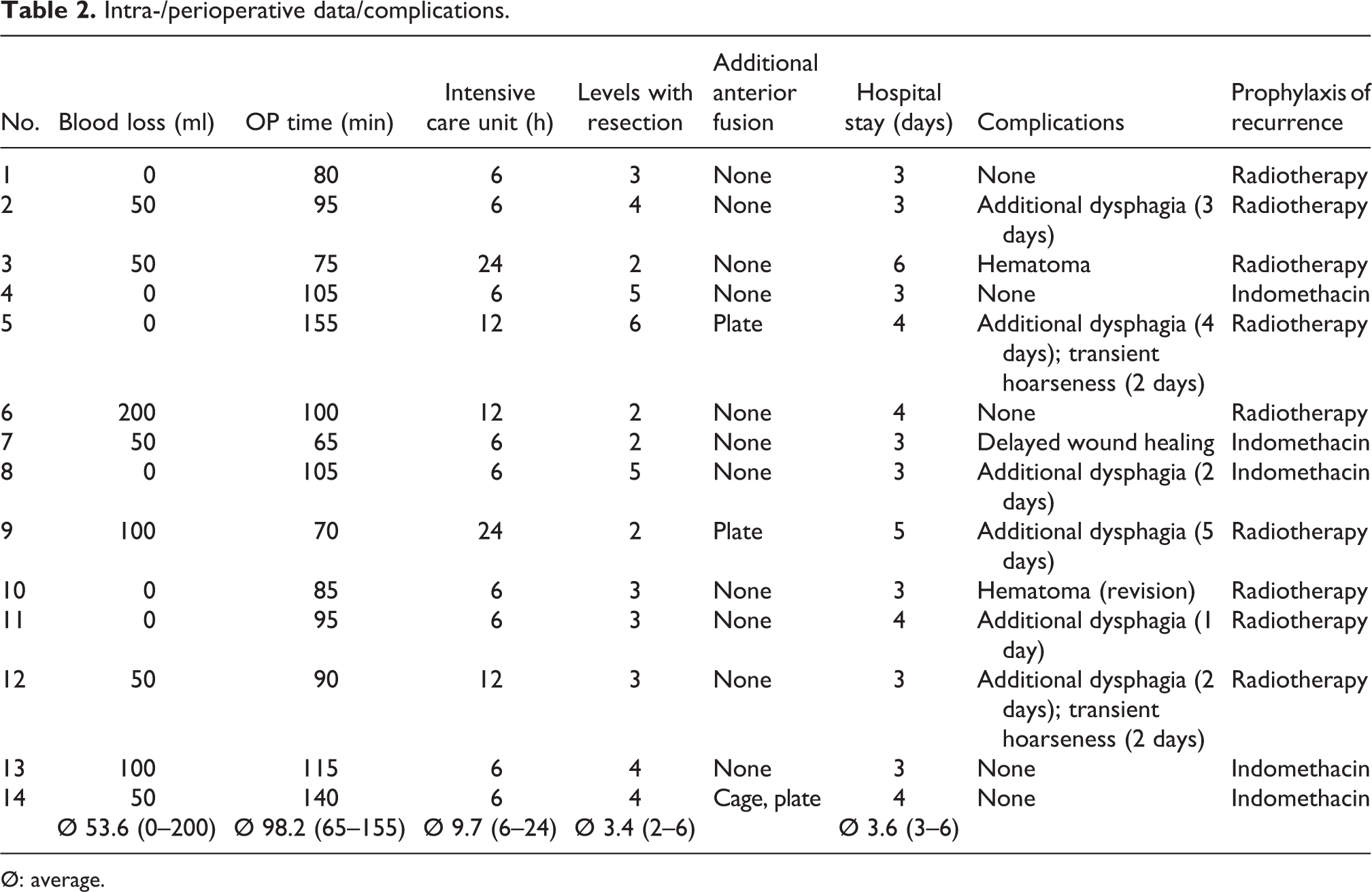
Intra- and perioperative data/complications
The intra- and perioperative parameters are presented in Table 2. No significant blood loss occurred. All patients were extubated immediately postoperatively. Five of 14 patients remained in the ICU for observation for 18 and 24 h, the other 9 only until the anesthesia wore off. No surgery-related pain medication was necessary. Six patients had a temporary postoperative increase in dysphagia for a few days; two patients had temporary hoarseness. Two patients had a hematoma, one of which was revised via the same surgical access. No other serious problems requiring treatment occurred. There was also no deterioration of the preoperative symptoms lasting more than 1 week. No additional complications were observed in the follow-up examinations. Two patients died after 72 and 47 months; the deaths were not related to the operation or dysphagia. Five patients were given indomethacin as recurrence prevention; nine patients received radiation. No recurrence of dysphagia occurred in the follow-up period. One patient still needed to adapt the consistency of food.
Intra-/perioperative data/complications.
Ø: average.
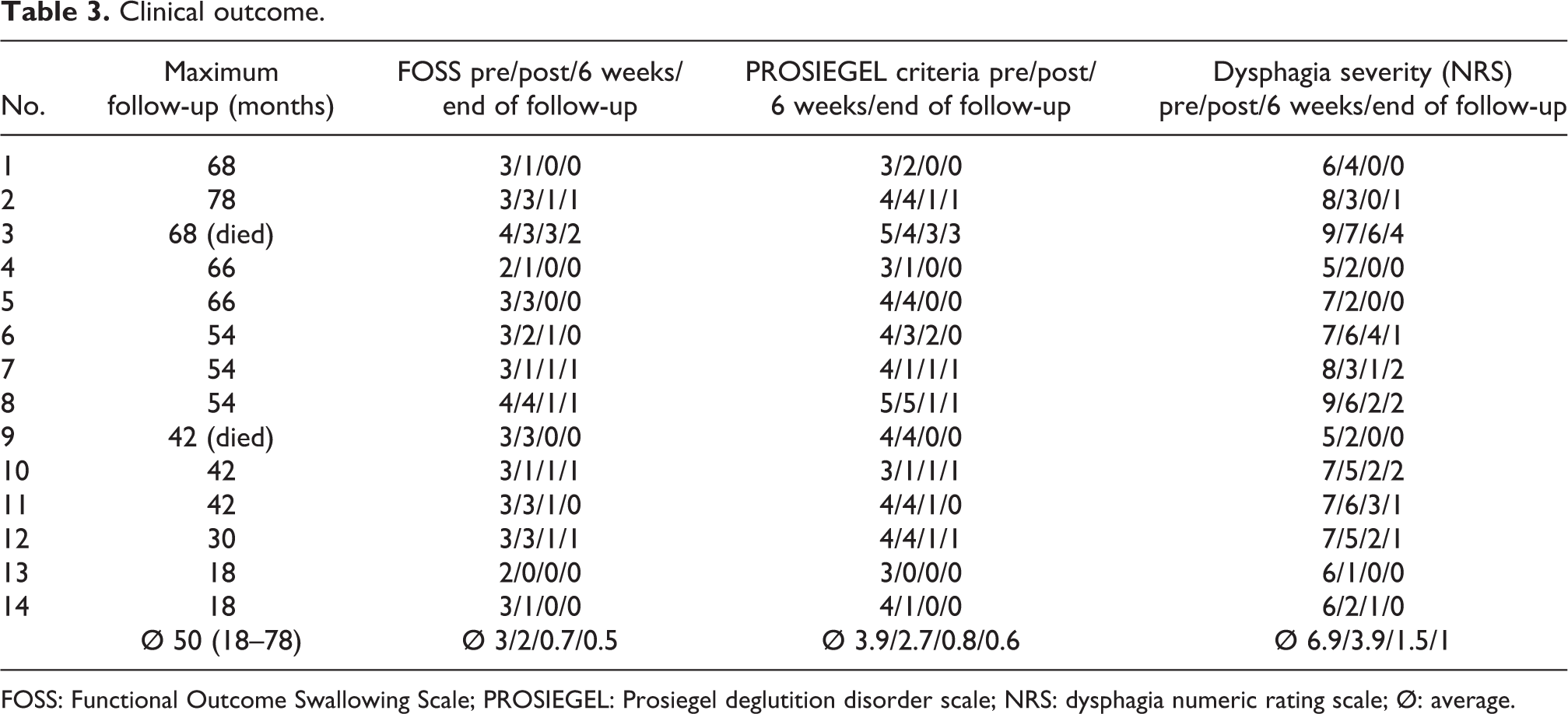
Clinical and radiological outcome
The clinical scores are presented in Table 3. Substantial improvement of the symptoms was observed in all patients. Only one patient (no. 3) continued to suffer from considerable limitations in food intake. In this patient, the symptoms had been present for 6 years. In 14 patients (86%), the final outcome was achieved after 6 weeks. Significant improvement of 2.5 was seen in the FOSS score, 3.3 in the Prosiegel criteria, and 5.9 in the NRS. The results remained stable over time. No patient reported symptoms of recurring dysphagia. The postoperative imaging examination showed the respective resection of the osteophytes up to the anterior edge of the vertebral bodies (Figures 4(a) and (b) and 5). Based on the clinical findings (no dysphagia) and the X-ray images, no recurrences were found during follow-up. There was also no increasing instability or failure of anterior fusion found.
Clinical outcome.
FOSS: Functional Outcome Swallowing Scale; PROSIEGEL: Prosiegel deglutition disorder scale; NRS: dysphagia numeric rating scale; Ø: average.

(a and b) Postoperative lateral X-ray and sagittal CT reconstruction after resection of the osteophytes up to the original anterior edge of the vertebral bodies. CT: computed tomography.

Postoperative transversal CT reconstruction after resection of the osteophytes with decompressed esophagus (large asterisk). CT: computed tomography.
Discussion
The prevalence of cervical anterior osteophytes in the elderly population is 20–30%. They are most often caused by degeneration, but usually remain asymptomatic. 38,39 Large symptomatic osteophytes usually develop with ankylosing hyperostosis and were first called Forestier’s disease and later DISH. They are systemic and are defined by radiological criteria. 1 –3 DISH is a rather rare disease (prevalence 5–35%) and affects primarily elderly men (>60). The etiology and pathogenesis are largely unknown; a genetic disposition and risk factors (hyperlipidemia, insulin, mechanical stress) have been discussed. The osteophytes are a noninflammatory condition. 3 –9 In our patient population as well, DISH was found to be the cause in approximately 65% of the cases. By contrast, with similar osteophytes in inflammatory axial spondyloarthritis, there is usually also involvement of the sacroiliac joint. 4 In addition, isolated cases of other causes of osteophytes, such as post-traumatic, congenital, or osteochondromas, have been reported. 40 –42
If anterior cervical osteophytes are symptomatic, nonspecific limitations of movement occur most frequently, but symptoms caused by compression of neural or soft tissue structures have also been described (e.g. neurological deficits, thoracic outlet syndrome, Horner’s syndrome, paralysis of the recurrent laryngeal nerve, insufficiency of the vertebral artery, dysphonia, or laryngeal spasm). 10 –15 Dysphagia is the most prominent symptom because the osteophytes are most often located between C4 and C7 and can lead to constriction of the retropharyngeal space and compression of the esophagus and larynx. 16,17 While the correlation between anterior osteophytes and dysphagia has sometimes been viewed critically, 11,43 it is generally recognized today. 4,22,44 –47 Sometimes a minimum size of the osteophytes in order to trigger symptoms is described. 27,48,49 In our patient population, the osteophytes were also found in the described location and sizes. Overall however, anterior cervical osteophytes are a rare cause of dysphagia. 4,38,50
The etiology of neurogenic dysphagia (damage to the central or peripheral nervous system) must be distinguished from structural dysphagia (primary, secondary) and dysphagia from other causes (e.g. psychogenic, dementia). Dysphagia caused by osteophytes is primarily structural due to direct compression of the esophagus, 2,18 but secondary causes can be inflammation of the adjacent soft tissue accompanied by edema, changes in the esophageal wall, or an abnormal position of the epiglottis. 4,19 –23 The swallowing disorder is frequently also combined with pain and can have additional symptoms such as dysphonia, cough, aspiration, or apnea. In an advanced stage, malnutrition and weight loss are possible. 4,22,23
CT, X-ray, and MRI imaging are carried out to establish the diagnosis, and to assess the esophagus, the barium swallow test and esophageal and laryngeal endoscopy with the option of taking a biopsy are conducted. 4,27,44,51,52 An intrinsic cause (e.g. esophageal stricture, motility disorder, diverticula, neoplasms, etc.) must be excluded in a gastroenterology or pulmonary examination.
Dysphagia can be caused by mechanical compression of the esophagus. 53 At the same time, inflammatory processes and pain and muscle spasms from the irritation of osteophytes are additional factors. 4,54 Swallowing can thus also be improved by conservative measures such as anti-inflammatory and analgesic drugs, muscle relaxants, postural changes, phonophoresis, or adaptations to the diet. 24,53,55 –57 If the extrinsic cause is more prominent, in case of more severe problems and impairment of the quality of life, surgical resection of the osteophytes via a standard anterior approach is performed. 4,24 –28 This can achieve sufficient improvement with a low morbidity rate 4,17 ; regression of the symptoms can occur quickly (in up to 2 weeks) but may sometimes take months. 21,26,27,30,58
The results are more limited the more advanced the changes in the esophagus itself are (inflammation, fibrosis, impaired peristalsis, etc.). 4,29 In our patients, substantial improvement of the symptoms was achieved in all cases. Only one patient still suffered from pronounced impairment of food intake during the later course. This patient had had symptoms for 6 years. In 86% of the patients, the result was achieved in 6 weeks. In general, the patients must be informed of the possibility of prolonged healing, especially if they have a long history or functional disorders of the esophagus. The preoperative differential diagnostic investigation is obligatory. All of our patients were found to have an extrinsic cause (compression from osteophytes) and in no patient was there clear evidence of a functional disorder of the esophagus itself, even when there was a longer history. Three patients showed more pronounced intraoperative mobility after removal of the osteophytes. Carrying out additional fusion has been discussed for such surgery-induced instability. 27,29,59 We stabilized these patients using anterior plates.
There were no problems with intra- and perioperative parameters such as blood loss, operation time, or stay on the ICU. The hospital stay was short. Nevertheless, dysphonia and progressive dysphagia have been described as rare, but serious complications. 27,60 It has therefore been noted that the effect of the surgical intervention must be critically assessed due to potential problems and the indication cannot always be unequivocally established. 31,61,62 In our study, two patients developed a postoperative hematoma, one of which required revision. One patient had delayed wound healing. A temporary increase in dysphagia or hoarseness for a few days (1–4 days) occurred in six patients, which can most likely be attributed to the intraoperative manipulation and is known to occur after anterior operations of the cervical spine. 63,64 No serious complications of dysphonia or progressive dysphagia occurred. A preoperative tracheotomy because of the prolonged surgery and risk of postoperative swelling of soft tissue no longer appears to be necessary. 65
The resection of the osteophytes does not eliminate the underlying condition and ossifications can develop again. In Forestier’s disease, increased ossification of scar tissue has even been observed. 66 Recurrent cervical osteophytes are rare, develop slowly, and have been described in long-term follow-up over 10 years. 4,17,29 –31 Routine additional fusion is therefore discussed not only due to possible operation-induced instability, but also because segmental mobility can promote the further development of osteophytes. 9,29 –31
There is experience in the prophylaxis of ossification in particular in connection with the implantation of hip replacements. For this procedure, at least 1 week of NSAIDs, particularly indomethacin, taking gastrointestinal contraindications into consideration, has become the established procedure. 26,32,33 The use of the bisphosphonate etidronate disodium, which can suppress ligament ossification in animal tests, 67 has not yet become standard because of the long period of medication (up to 6 months) and high costs. 33,68 Radiation within the first four postoperative days can reliably reduce ossification without leading to serious gastrointestinal or systemic side effects. 34,35,69 The effect is based not on a cell-destroying effect such as in tumor treatment with ionized radiation, but on the short-term inhibition of osteogenic differentiation in the mesenchymal stem cells. 70,71 Continuing radiation after the 4-day window can even lead to an increase in ossification. 69 Until now, radiation has been fractionated and dose-reduced; nevertheless, a possible negative effect on the healing rate (especially for implants) is known and a possible carcinogenic effect has been discussed. 34,72 Although no data are yet available about the development of malignant neoplasms after radiation given to prevent the recurrence of ossifications, radiation is more often recommended when NSAIDs are contraindicated or in older patients (e.g. over age 55), because an increased sensitivity to radiation is assumed at a younger age. 73 –75
In general, there is limited experience and no precise guidelines for the prophylaxis of recurrent anterior cervical ossifications, made even more difficult due to the long period before a new occurrence. In our study, patients up to age 55 were given 50 mg indomethacin twice daily for 10 days as prophylaxis. If the administration of NSAIDs was contraindicated in the patient history or if the patients were older than 55, radiation was given—fractionated with five doses of 2 Gray to protect the spinal cord. No negative effect on the postoperative course (e.g. wound healing disorder) occurred in these patients. Based on the clinical findings (no dysphagia) and the X-ray images, no recurrences have been observed thus far, but cannot be ruled out during the continuing follow-up period. We, the authors, conduct additional anterior stabilization only if there was existing preoperative instability or if intraoperative instability developed, but not routinely as recurrence prevention. No signs of operation-induced instability were found in the patients with no additional anterior stabilization.
The evaluation of the results of this study is limited by the retrospective study design, the pathology-related relatively small cohort, and the limited follow-up period. Nevertheless, this study is among the studies with the largest number of cases.
Conclusion
When conservative treatment fails, surgical resection of cervical osteophytes is a sufficient method for treating spondylogenic dysphagia. High patient satisfaction and an improvement in the quality of life can be achieved with a low complication rate. The differential diagnostic clarification of extrinsic and intrinsic causes is obligatory. The exact procedure for recurrence prevention has not yet been established. In addition to routine additional stabilization, prevention using indomethacin or radiation also seems to be possible.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.