
Abstract
Purpose:
Reconstruction of the lateral collateral ligament (LCL) and biceps femoris tendon following proximal fibula resection is controversial. Postoperative knee instability and peroneal nerve dysfunction affect outcome. This study aimed to determine functional, clinical, and radiological outcomes of patients who underwent en bloc proximal fibula resections and to compare clinical and radiological instability rates for primary repair after type I and type II resections.
Materials and Methods:
Eleven patients with primary tumors of the proximal fibula were included. Musculoskeletal Tumor Society (MSTS) score and Lysholm knee score were used in the evaluation of functional outcomes. Clinical outcome was assessed using knee range of motion and knee varus stress test. Radiological outcome was assessed using varus stress knee radiographs. Knee stability was evaluated using the varus stress test at 30° of knee flexion and varus stress knee radiographs and graded in millimeters.
Results:
Of the 11 tumors, 6 (54.6%) underwent type I resection. In five (45.4%) patients, type II resection was performed. The mean follow-up period was 32 ± 13.9 months (range, 12–55 months; median, 27 months). The mean knee joint lateral opening, MSTS score, and Lysholm knee score with type I versus type II resection were 5.7 ± 1.2 mm versus 6.4 ± 1.1 mm (p = 0.247), 28.7 ± 1.8 (95.6%) versus 20.4 ± 7.7 (68%) (p = 0.011), and 92.2 ± 8.8 versus 62.8 ± 20.4 (p = 0.026), respectively. Postoperative complications of all patients included one (9.1%) deep tissue infection and one (9.1%) long-term knee instability. In one patient (9.1%) who underwent type II resection, above-the-knee amputation was performed after local recurrence.
Conclusions:
Primary repair of the LCL and biceps femoris tendon to the surrounding soft tissues after resection of proximal fibular tumors provides good clinical outcomes. Primary repair is a simple technique to perform with minimal morbidity. Peroneal nerve palsy was a problem, especially in type II resections.
Introduction
The proximal fibula is a rare location for primary bone tumors or metastases. 1 The incidence of primary bone tumors in the fibula is between 2.5% and 4.08% of all primary bone tumors. 2 –4 The close proximity to the surrounding tissues including the anterior tibial artery, the common peroneal nerve, and the lateral collateral ligament (LCL) causes major difficulties in proximal fibula tumor resections to provide clean histological margins. 5 Malawer described two types of en bloc resection: Type I, marginal resection, includes resection of proximal fibula with 2–3 cm of diaphysis and muscles around fibula (Figure 1). 6 The peroneal nerve is protected. In type II, wide extra-compartmental resection, proximal fibula, 5–6 cm of diaphysis, anterior and lateral muscle compartments, anterior tibial artery and peroneal nerve must be resected (Figure 2). 6 Epineurectomy can be used if the tumor contacts but does not infiltrate the nerve. 5,7 Type I resection is appropriate for benign aggressive, low-grade malignant and metastatic tumors, because these tumors have no significant extraosseous extension. 8 On the other hand, type II resection is appropriate for high-grade sarcomas invading anterior and lateral muscle groups and the common peroneal nerve. 8 Damage to the peroneal nerve and resection of anterolateral muscles lead to foot drop or sensory deficit. 6 The incidence of postoperative peroneal nerve palsy was reported between 3% and 57%. 1
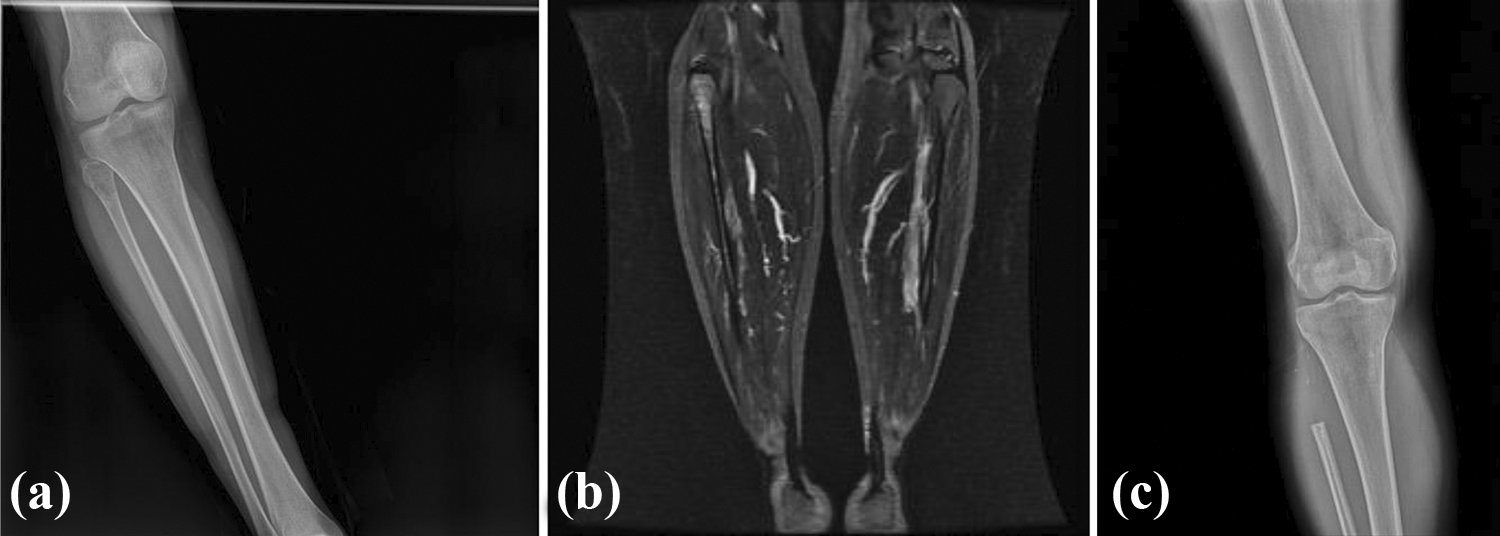
A 27-year-old patient with a high-grade chondrosarcoma of the proximal fibula. A type I resection of the proximal fibula was necessary. (a) Preoperative X-ray findings show osteolytic–osteoblastic lesion with periosteal reaction. (b) T2-weighted coronal magnetic resonance imaging of the proximal fibula tumor. (c) Postoperative X-ray findings 2 years later.

A 17-year-old patient with a high-grade osteosarcoma of the proximal fibula. A type II resection of the proximal fibula was necessary. (a) Preoperative X-ray findings show osteolytic–osteoblastic lesion with periosteal reaction. (b) T2-weighted coronal magnetic resonance imaging of the proximal fibula tumor. (c) Postoperative X-ray findings 1 year later.
Local recurrence is the most serious postoperative complication which is dependent on tumor histology and resection type. 9 The proximal fibula resection technique has some difficult steps as in dividing the interosseous membrane and extra-articular resection of the proximal tibiofibular joint. 6
Knee instability is unavoidable after resection of the LCL insertion site or a segment of LCL. 8
After proximal fibula resections, need for LCL reconstruction is controversial. 9 –11
The primary aim of this study was the assessment of clinical, functional, and radiological outcomes and complications after type I and II proximal fibula resections. Secondary purpose was to investigate clinical and radiological instability rates of proximal fibula resections due to primary fibula tumors without reconstruction of the LCL attachment.
Methods
Between 2011 and 2016, 11 patients with primary malignant proximal fibula tumors were diagnosed and treated in our clinic. Of these, four patients were treated before 2014. Their records were reviewed retrospectively. The remaining seven patients were treated and followed prospectively. The ethics committee of our hospital approved this study.
An open or closed biopsy was performed before resections. Histologic diagnoses included four cases of malignant low-grade chondroid tumor (36.4%), two cases of osteosarcoma (18.2%), two cases of Ewing sarcoma (18.2%), one case of chondrosarcoma (9.1%), one case of pleomorphic sarcoma (9.1%), and one case of osteochondroma (9.1%).
An en bloc resection was performed in all patients. Type I (marginal) resection was performed in six patients (54.6%). The common peroneal nerve and its branches were preserved in all patients who underwent type I resection. One patient had intermittent peroneal nerve palsy that completely resolved 4 months postoperatively. The anterior tibial artery was spared in patients if possible. The proximal tibiofibular joint was excised intra-articularly.
A type II resection was performed in five patients (45.4%). Approximately 5 cm of normal diaphysis of the fibula, anterior and lateral muscle compartments and anterior tibial artery were resected. The peroneal nerve was resected in four patients who developed drop foot postoperatively. LCL and biceps femoris stumps were reattached to the surrounding soft tissues. Additional reinforcement sutures were placed to the overlying iliotibial band.
In the surgical technique, semisupine position with previously described single utilitarian approach was used to access all four compartments of the leg and popliteal fossa. 6 The previous biopsy tract with 3 cm margin was included in the incision site. Exploration of the common peroneal nerve at the base of the fibular head, exploration of the popliteal fossa and blood vessels, excision of the anterior and lateral muscle compartments with underlying deep fascia, release of LCL and biceps femoris tendon insertion sites 2.5–5 cm proximal to fibular insertion site, and proximal fibula resection with extra-articular resection of proximal tibiofibular joint were performed in type II resections. The knee joint capsule was repaired to prevent synovial fistula if opened. LCL and biceps femoris stumps were reattached to the surrounding soft tissues with nonabsorbable sutures (Ethibond no. 5, Ethicon Inc., New Jersey, USA) when the knee was in 30° of flexion. Additional reinforcement sutures were placed to the overlying iliotibial band. In type I resections, the common peroneal nerve and its branches were preserved in all patients. The anterior tibial artery was spared in patients if possible. The proximal tibiofibular joint was excised intra-articularly.
The routine follow-up protocol included patient visits at 2 weeks, 1 month, 3 months, 6 months, 1 year, 18 months, 2 years, 3 years, and 4 years postoperatively. Follow-up was dependent upon patient and pathology. Weight-bearing plain radiographs were obtained at all follow-up visits, and MRI was obtained at every 6 months in postoperative 2 years and yearly after that.
Functional outcomes were assessed using the Musculoskeletal Tumor Society score (MSTS) and Lysholm knee score. 12,13 A percentage of total scores for MSTS were expressed (Table 1). Anterior and posterior cruciate ligaments, posteromedial and posterolateral corners of the knee were examined both by physical examination and preoperative knee MRI examination and they clarified to be intact. Clinical outcome was assessed using knee range of motion and knee varus stress test. Radiological outcome was assessed using varus stress knee radiographs. Knee stability was evaluated using the varus stress test at 30° of knee flexion and varus stress knee radiographs and graded in millimeters. 14 Zero to 5 mm lateral opening was graded as grade I, 6–10 mm lateral opening as grade II, and more than 10 mm lateral opening as grade III. 15
Summary of patient demographics, diagnosis, treatment, complications, clinical and radiologic outcomes.

MSTS: musculoskeletal tumor society.
The rehabilitation program was patient- and resection-type based. In both type I and type II resections, 0–90° passive ROM and strengthening exercises were initiated 1 day postoperatively. Six weeks of partial weight-bearing with a knee immobilizer locked in extension was allowed. After 6 weeks, the immobilizer was discontinued, and patients were encouraged to perform full active and passive ROM, and progressive full weight-bearing with a crutch for the next 6 weeks. In type II resections, 6 weeks of partial weight-bearing with a knee immobilizer and an ankle-foot orthosis (AFO), and 0–90° passive ROM was allowed. After 6 weeks, the immobilizer was discontinued, and patients were encouraged to perform full active and passive ROM, and progressive full weight-bearing with an AFO and crutch for the next 6 weeks. Passive ROM and strengthening exercises were initiated 1 week postoperatively. In patients with postoperative peroneal nerve dysfunction and lack of anterior and lateral muscular compartments, an AFO was used to prevent equinus deformity.
The following values were used for descriptive statistics of the data: mean, standard deviation, median, lowest, highest, frequency, and ratio. The distribution of variables was measured using the Kolmogorov–Smirnov test. The Mann–Whitney U test was used in the analysis of quantitative independent data. In the analysis of qualitative independent data, χ 2 test and Fisher’s exact test were used in the analysis of qualitative independent data. A p value of <0.05 was considered to be statistically significant. SPSS IBM Statistics 22 (IBM, Armonk, New York, USA) was used for all statistical analyses.
Results
There were seven females and four males, with an average age of 36.2 ± 19.4 years (range, 15–78 years). The proximal epiphysis was involved in 11 patients (100%). The metaphyseal involvement was seen in five patients (45.4%). There was right side involvement in eight patients (72.7%) and left side involvement in three patients (27.3%). The mean follow-up period was 32 ± 3.9 months (range, 12–55 months; median, 27 months). No patients were lost to follow-up.
Pain was the most common presenting symptom (100%) followed by a palpable mass in four patients (36.4%). One patient (9.1%) with osteochondroma presented with signs and/or symptoms of peroneal nerve compression. No pathologic fractures were observed.
There was grade I laxity in four of six patients (66.6%) who underwent type I resection. The remaining two patients (33.4%) had grade II laxity. In the type II resection group, one patient (20%) had grade I laxity and four patients (80%) had grade II laxity. The mean knee joint lateral opening was 6 ± 1.2 mm (range, 5–8 mm); it was 5.7 ± 1.2 mm in patients who underwent type I resection and 6.4 ± 1.1 mm in patients who underwent type II resection (p > 0.05) (Table 2). One patient (9%) developed delayed wound healing and infection postoperatively. After surgical debridement and intravenous antibiotic therapy, the infection was eradicated, and a successful wound closure was provided. One patient with osteosarcoma developed local recurrence 7 months after surgery due to an undetected skip lesion of the proximal tibia which was treated with amputation. The local recurrence was detected on MRI after patient’s new onset pain complaint. A successful proximal fibula resection with wide margins was performed in all the remaining cases of malignant tumors. Preoperative mean proximal to distal diameter of the tumor was 70.2 ± 59.6 mm (range, 21–217 mm). A mean of 148 ± 89 mm (range, 60–300 mm) bone tissue was resected.
Comparative parameters of the two groups.
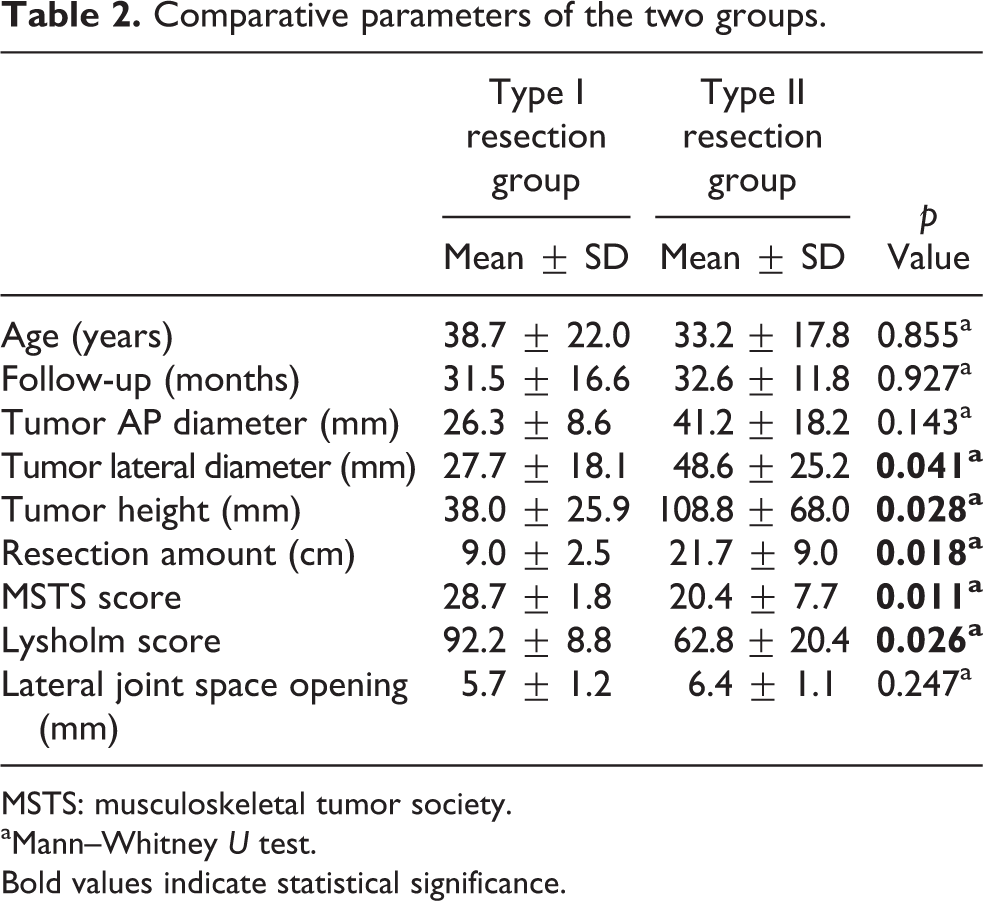
MSTS: musculoskeletal tumor society.
aMann–Whitney U test.
Bold values indicate statistical significance.
In four patients, resection of the peroneal nerve was necessary; almost complete anterior and lateral muscle groups were resected in five patients. Postoperatively, five patients developed drop foot. In one patient, the peroneal nerve was preserved, and full function was restored 16 weeks after the operation. A permanent drop foot occurred in four patients. The mean MSTS score was 28.7 ± 1.8 in patients who underwent type I resection and 20.4 ± 7.7 in patients treated with type II resection (p < 0.05). The mean Lysholm knee score was 92.2 ± 8.8 in patients who underwent type I resection and 62.8 ± 20.4 in patients treated with type II resection (p < 0.05) (Table 2). At the final oncological follow-up, all patients continued to be disease-free.
Discussion
Resection of the surrounding tissues with bone to provide local control in proximal fibula tumors increases the risk of development of complications such as peroneal nerve palsy, foot drop, knee instability, wound problems, and infection. 5,16 As a result, the functional status and the quality of life are adversely affected.
More than 3–4 cm of the proximal bone segment is needed to preserve lateral ligament complex. If the tumor involves the fibular head, an extra-articular resection of proximal tibiofibular joint is necessary. 5 In our study, all patients had fibular epiphysis involvement. We performed extra-articular resection with the lateral ligament complex.
Cadaver studies have demonstrated that LCL plays an important role in resistance to varus rotation and biceps femoris plays an important role in anterior stability. 17 Knee instability and gait abnormalities may occur after proximal fibula resection. 18 Bickels et al. reported knee instability of 7% after Malawer type I resections and 50% after Malawer type II resections. 8 Varus laxity is commonly detectable on physical examination. But, it is not often symptomatic. 19 In our study, resection of the lateral ligament complex was performed in 6 of 11 patients. After primary repair of the stumps to the surrounding soft tissue, a mean 6.4 ± 1.1 mm lateral joint opening was observed on weight-bearing radiographs. One patient had postoperative permanent knee instability after type II resection. He used an orthotic device while increasing his activity. Instability of the knee may lead to osteoarthritis. 20 After proximal fibula resections, LCL and biceps femoris should be repaired. A rehabilitation program as an acute lateral knee ligament injury is recommended to prevent knee instability. 20 In our study, patients underwent a similar rehabilitation program as acute lateral ligament injury repair/reconstruction with some minor differences. At the last follow-up, 6 of 11 patients had clinical and radiologic instability findings. Only one patient had symptomatic instability of knee.
Repair of LCL and biceps femoris after proximal fibular excision is needed. 6,18 In the literature, reconstruction of the LCL and the biceps tendon after tumor excision is controversial. 8 Some authors advocate that the knee remains functionally stable after resection of the proximal fibula because the other knee stabilizers are intact and reconstruction of the LCL is not necessary. 10,21 Remaining LCL and biceps femoris stumps may be attached to lateral metaphyseal site of tibia or repaired to surrounding capsular and ligamentous structures. 8,18 The best method for reattachment is not known. In our study, we reattached the LCL and biceps femoris stumps to the surrounding soft tissue structures.
On the other hand, Zhao et al. compared knee stability and MSTS functional scores of patients who underwent type I and type II en bloc proximal fibula resections. 11 According to their results, in patients who underwent LCL and biceps femoris tendon reconstruction surgery, higher rates of knee stability and MSTS scores were exhibited as compared to patients without reconstruction. Additionally, for type I resections, they reported a higher rate of knee stability in the reconstruction group, while no statistical difference was found for type II resections. In our study, primary repair of the LCL and biceps femoris tendon to the adjacent soft tissues was performed in all patients whether they underwent type I or type II resection. We found significantly higher mean MSTS and Lysholm scores in the type I resection group than in the type II resection group. The lateral joint space opening in the type I resection group was lower than that of the type II resection group. Loss of the peroneal nerve and large quantity of muscle tissue resected from the anterolateral compartment may be the reason for the inferior functional outcomes of patients treated with type II resection. According to our results, resection type seems to be associated with knee stability following surgery.
Additionally, the LCL and biceps femoris tendon stumps are shorter after type II resection. This may cause difficult and less effective repair and reconstruction.
A gastrocnemius flap is an alternative method for soft tissue reconstruction in type II resection to provide support. 22 This technique alone has some mechanical problems, such as increased peak knee flexion during swing phase.
Peroneal nerve resection causes stepping gait, drop foot, and gait instability and should be avoided if possible. 23 An AFO is needed when drop foot develops. 7 If patients do not tolerate an orthosis, a tibialis posterior tendon transfer might be a good alternative. Direct reconstruction of the peroneal nerve is not recommended because the results are poor. 24,25 In our case series, four patients with drop foot and with lack of anterior and lateral muscular tissues tolerated AFO well.
To obtain a safe surgical margin, tibialis anterior artery is routinely ligated. This causes no problem in lower extremity circulation if the tibialis posterior artery is preserved. In some cases, tibialis posterior artery may be sacrificed to achieve clear surgical margin. Preoperative angiography is crucial to rule out possible tumor violations, obstructions, and anatomic variations. 26 In 5% of normal lower extremities, posterior tibial artery is absent. 6 In those cases, amputation or a bypass procedure should be needed. Preoperative angiogram showed no tumor violation, obstruction, or anatomic variation in the tibialis posterior artery. Therefore, no amputation or bypass surgery needed.
Postoperative wound problems are expected in patients who receive chemotherapy and radiation therapy. 27 In our series, delayed wound healing was developed in only one patient. This patient had a deep wound infection that was treated with debridement and intravenous antibiotic therapy.
There were significantly better functional outcomes in patients with benign tumors and type I resections than in patients with malignant tumors and type II resections. This is not surprising because in cases of benign tumors and type I resections, neither resection of the peroneal nerve nor significant muscle excision was necessary.
Our study has some limitations. Our follow-up period is relatively short. The relatively small number of patients may make the statistical results less meaningful. A wide variety of histological tumor types were included, leading to widely variable pre- and postoperative medical approaches. Multiple surgeons performed the surgical procedures. Also, patients with only one repair technique were included. Patient with different repair or reconstruction techniques would give more comparable results.
Conclusion
Primary repair of the LCL and biceps femoris tendon to the surrounding soft tissues after resection of proximal fibular tumors provides good clinical outcomes. Primary repair is a simple technique to perform with minimal morbidity. Peroneal nerve palsy was a problem, especially in type II resections. A longer follow-up period with larger patient populations is required to determine the risk of knee osteoarthritis in patients with asymptomatic knee instability.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.