
Abstract
Introduction:
The aim of this retrospective study was to evaluate the outcomes of older patients with 2-part proximal humerus fractures (PHFs) with medial column disruption stabilized using a proximal humeral internal locking system (PHILOS) plate plus oblique insertion of autologous fibula as a primary procedure.
Materials and Methods:
Data involving 112 patients (112 shoulders) sustaining 2-part PHFs with medial column disruption treated with PHILOS plate plus oblique insertion of autologous fibula as a primary procedure during 2012-2019 were identified. The median follow-up was 36 months (range: 11.2-43.5 months). The primary endpoint was the Constant scores and American Shoulder and Elbow Surgeons (ASES) scores. The secondary endpoint was the main orthopedic complication rate.
Results:
The median Constant and ASES scores were 78 (range, 52-95) and 77 (range, 62-96) at the final follow-up, respectively. The main orthopedic complication rate was 10.7% (12/112). Twelve orthopedic complications in 8 patients were detected, and they involved loss of reduction, varus collapse, aseptic loosening, mal-union, revision, and intolerable shoulder pain. Of these complications, 3 (2.6%) involved loss of reduction, 2 (1.7%) involved varus collapse, 3 (2.6%) involved aseptic loosening, 1 (0.8%) involved mal-union, 2 (1.7%) required revision surgery, and 1 (0.8%) presented intolerable shoulder pain.
Conclusion:
PHILOS plate plus oblique insertion of autologous fibula as a primary procedure may yield good functional outcomes and a low rate of the main orthopedic complications.
Introduction
Almost 50% of proximal humerus fractures (PHFs) are displaced, the majority of which involve the humeral calcar. 1 -4 The optimal management of 2-part PHFs with medial calcar disruption in the elderly remains controversial. 5 Loss of medial calcar support or calcar comminution has been acknowledged as a key prognostic factor for humeral head subsidence with reduction loss and intra-articular screw cut-out. 5,6 Although proximal humeral internal locking system (PHILOS) osteosynthesis has been deemed a standard management with primarily beneficial short-term functional outcomes, the major orthopedic complication rates remain inacceptable. 7 -9 In addition, advocates of PHILOS osteosynthesis describe activities that are contributing to the achievement of encouraging functional outcomes or point to specific challenges in complications that need to be addressed. 9,10 To date, simple PHILOS osteosynthesis remains difficult to attain. 9 Simultaneously, the utilization of hemiarthroplasty has frequently been conditioned by impaired bone quality (fracture comminution and osteopenia) in elderly individuals, especially those with severe osteoporosis. 11 Osteoporosis is overpoweringly implicated in the failure of surgical intervention produces, contributing to as high as a 10-30% revision rate. 12 Failures secondary to PHILOS osteosynthesis or hemiarthroplasty are well known, and they are universally addressed with a conversion to cemented or uncemented reverse total shoulder arthroplasty (RTSA). 13,14 This conversion will indisputably contribute to increasing treatment costs and cycles and severe mental and physical burden of patients.
The lack of consistency regarding the optimal fixation of 2-part PHFs with medial calcar disruption in elderly individuals in the literature, 15,16 accompanied by the debilitating nature of shoulder function, warrants further exploration into this challenging issue. We performed this retrospective study to assess outcomes of older patients sustaining 2-part PHFs with medial column disruption stabilized using this PHILOS plate plus oblique insertion of autologous fibula as a primary procedure.
Methods
Study Population
This study was approved by our Medical Ethics Committee, and an exemption from informed consent was obtained from our responsible Investigational Ethics Review Board. From January 2012 to December 2019, 133 patients (133 shoulders) sustaining displaced PHFs treated with PHILOS plate plus oblique insertion of autologous fibula as a primary procedure were identified from our tertiary medical center. The inclusion criteria involved patients with 2-part PHFs with medial column disruption (Figure 1A-D) and PHFs initially stabilized with a PHILOS plate (Synthes, Solothurn, Switzerland) plus oblique insertion of autologous fibula. The autologous fibula was obtained from the patient after exposing the fractured end of the humerus. The length of the fibula obtained was determined based on the patient’s bone condition, generally 4-7 cm. The main exclusion criteria involved defective clinical data, open fractures, 1-, 3-, or 4-part PHF, tuberosity fractures, severe vascular and nerve injury in the affected shoulder, pathological fracture, affected shoulder dyskinesia prior to surgery, loss of ability to follow instructions, active heavy infection(i.e., acute inflammatory response syndrome), an injury-severity score (ISS) of ≥ 8, delirium, drug or alcohol abuse, and an American Society of Anesthesiologists (ASA) score of IV or V. To avoid human error, the study data were reconfirmed by the 2 co-authors (XSZ and WY). Based on our criteria, a total of 112 patients (112 shoulders) were available and included in the final evaluation, as shown in Figure 2. The median age was 51.2 years (range, 40-62 years). The median follow-up was 36 months (range, 11.2-43.5 months). Patient characteristics were shown in Table 1.

Preoperative anteroposterior (A), coronal black and white (B) radiographs, and three-dimensional computed tomography (CT) reconstruction image (C and D), illustrating a 2-part proximal humerus fractures (PHFs) with medial column disruption. Postoperative radiographs of the proximal humerus (E and F) and three dimensional computed tomography (CT) reconstruction image (G and H).

Flow diagram demonstrating methods for identification of studies to evaluate the outcomes of older patients with 2-part proximal humerus fractures (PHFs) with medial column disruption stabilized using a proximal humeral internal locking system (PHILOS) plate plus oblique insertion of autologous fibula as a primary procedure, and to clarify the reasons for exclusion.
Patient Demographics at the Time of Surgery.
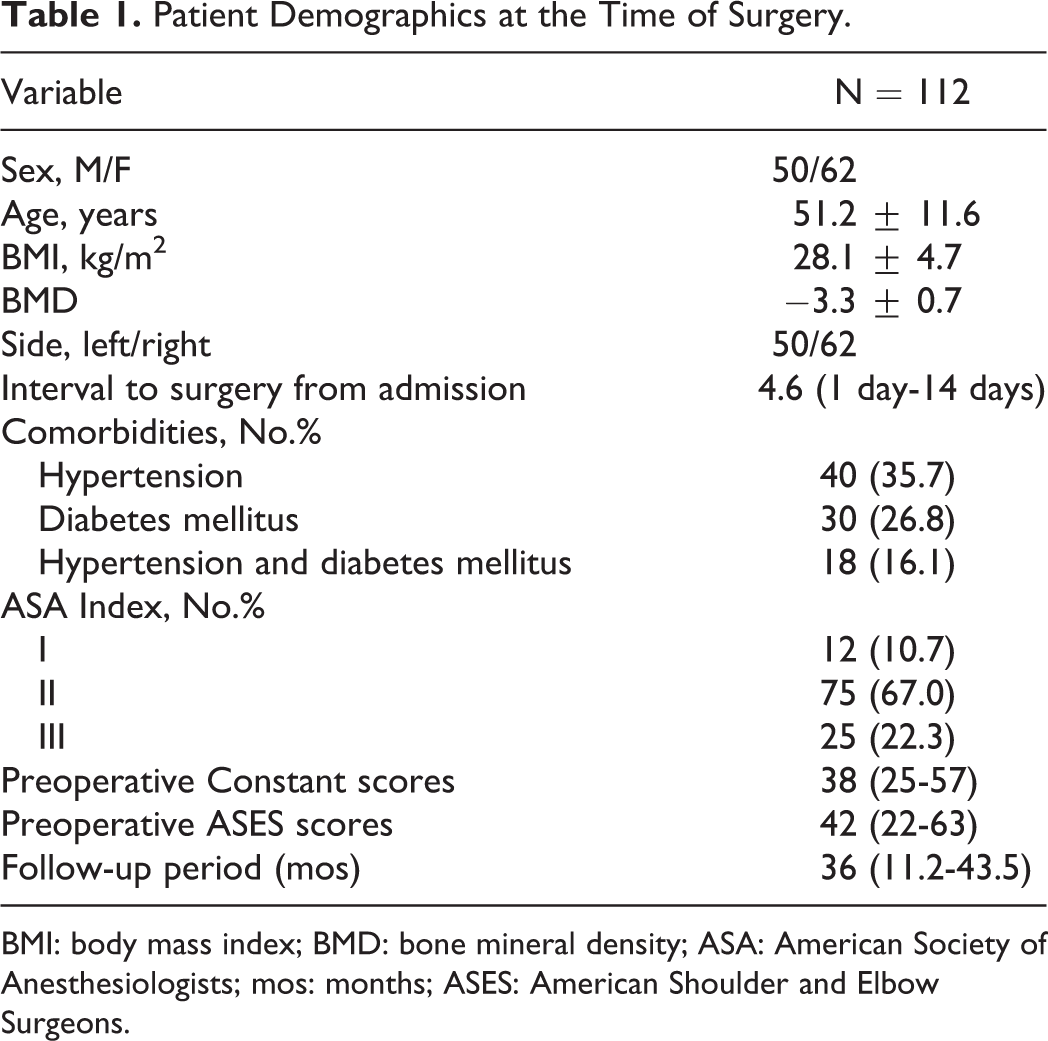
BMI: body mass index; BMD: bone mineral density; ASA: American Society of Anesthesiologists; mos: months; ASES: American Shoulder and Elbow Surgeons.
The primary endpoints were the Constant scores and American Shoulder and Elbow Surgeons (ASES) scores. The secondary endpoint was the rate of main orthopedic complication involving loss of reduction, varus collapse, screw penetration, avascular necrosis of the humeral head, aseptic loosening, mal- or non-union, periprosthetic fracture, revision, dislocation, deep infection, and intolerable shoulder pain. Follow-ups occurred 1, 3, 6, and 12 months after surgery and every year thereafter. Image data collected at the same follow-up points included the anteroposterior (AP) and lateral views and a computed tomography (CT) in a 3-dimensional reconstruction, and these data were evaluated by high-volume radiologists. Loss of reduction was assessed according to humeral head height relative to the PHILOS plate, as reported, 17 and defined as the difference of more than 3 mm in the humeral head height on the 2 AP shoulder views taken immediately after surgery and at final follow-up. The evaluation of restoration of the humeral neck-shaft angle was based on the Paavolainen method. 18 Varus collapse was defined as a change in neck shaft angulation to less than 120°. Calcar restoration was defined as previous descriptions. 17
Surgical Technique
Surgical techniques were consistent with previous reports. 5,17 The fracture site was exposed along the intermuscular space and the intertubercular groove was marked. After success to restore the medial calcar, the fracture blocks were temporarily fixed using two 2.5-mm Kirschner wires through the inner cortex of the intertubercular groove, and the wires and the bone marrow tunnel avoided intersections. The PHILOS plate was used temporarily to ascertain the entry point of the lateral cortex of the tunnel. A cylindrical autologous fibula was prepared with a length of 50 mm. Finally, the positions of the prosthesis and autologous fibula was assessed using the C-arm machine. A negative pressure drain was placed and removed 2 days after surgery. The postoperative radiographs were presented in Figure 1E-H.
The same rehabilitation protocol after surgery was performed, which emphasized the early functional activities. Partial weight bearing was advocated after 2 days of upper limb suspension. A consistent protocol of prophylactic use of antibiotics (Cefazolin, 2.0 g; ivgtt, Bid, Baomanbio, Shanghai, China) was followed for 3 days starting the day prior to surgery. An anticoagulant regimen (Enoxaparin sodium; Clexane 4000 AXa IU; ih, Qd, AVENTIS, Shanghai, China) was injected for each patient without contraindications for 7 days starting at admission.
Statistical Analysis
Preoperative and postoperative functional outcomes were expressed as the mean ± standard deviation (SD) or means and were compared using Student t-test for normally distributed variables and Mann-Whitney U test for non-normally distributed variables. Categorical variables are presented as ranges or values. Statistical significance was defined as 2-sided p < 0.05. All statistical analyses were carried out using SPSS version 26.0(Inc., New York, USA).
Results
The median Constant and ASES scores after surgery were shown in Table 2. The PHILOS plate plus oblique insertion of autologous fibula yielded satisfactory functional outcomes. The median Constant scores improved from 38 (range, 25-57 points)) prior to surgery to 78 (range, 52-95 points)) at the final follow-up; the median ASES scores improved from 42 (range, 22-63 points)) to 77 (range, 62-96 points)). Almost 78% of patients with 2-part PHFs with medial column disruption had an exciting functional score at the final follow-up.
Functional Outcomes at Each Follow-Up.

ASES: American Shoulder and Elbow Surgeons.
Table 3 showed the main orthopedic complications. Throughout the follow-up period, the main complication rate was 10.7% (12/112). Twelve orthopedic complications in 8 patients were detected involving loss of reduction, varus collapse, aseptic loosening, mal-union, revision, and intolerable shoulder pain. Of these complications, 3 (2.6%) involved loss of reduction, 2 (1.7%) involved varus collapse, 3 (2.6%) involved aseptic loosening, 1 (0.8%) involved mal-union, 2 (1.7%) required revision surgery, and 1 (0.8%) presented intolerable shoulder pain. One patient was revised using a long PHILOS plate and placing autologous sacrum; the other requested a semi-shoulder joint replacement. Revision was attributed to poor bone quality in this study. Non-union, screw penetration, avascular necrosis of the humeral head, periprosthetic fracture, dislocation, or deep infection was not detected in the current analysis.
The Main Orthopeadic Complications.

Discussion
This retrospective analysis may provide evidence that by combining axial and angular stability, a PHILOS plate plus oblique insertion of autologous fibula presents increased osseous anchorage and greater failure loads, and has a significant effect in managing 2-part PHFs with medial column disruption in elderly individuals with osteoporosis.
Limited studies 17,19 have assessed the outcomes of patients with 2-part PHFs with medial column disruption stabilized using a PHILOS plate plus vertical insertion of autologous fibula as a primary procedure. Furthermore, there remain concerns about the correctness of the PHILOS plate plus vertical insertion of autologous fibula. 19 A growing but still extremely limited body of literature 17 has assessed the role of a locking plate plus oblique insertion of autologous fibula and revealed that for 2-part PHFs, predominantly in elderly individuals with severe osteoporosis, locking fixation with an autologous fibular strut produced rigid medial support along with excellent functional outcomes and low rates of reduction loss, varus collapse and avascular necrosis of the humeral head. This favorable result could partially be attributed to the reconstruction of the medial column because the autologous fibular strut potentially improves dynamic axis stability and has the ability to minimize the risk of reduction loss or varus collapse after surgery. 20 -22 In addition, a reduced rate of complications was detected in a study by Jung et al. 20 that assessed PHFs with medial column disruption treated with locking plate plus an endosteal strut allograft as a primary procedure. The initial technique by Gardner et al. 23 demonstrated that non-union or loss of reduction failed to be observed. Combined with the current results, the locking plate plus autologous fibula tended to be the preferred surgical strategy for managing 2-part PHFs with medial column disruption. The current results of 2-part PHFs with medial column disruption treated with a PHILOS plate plus oblique insertion of autologous fibula have also revealed low rates of reduction loss, varus collapse and avascular necrosis. Shoulder stability following the PHILOS plate plus oblique insertion of autologous fibula is superior to that reported after PHILOS plate alone due to re-establishing medial support. Loss of medial calcar support or calcar comminution tends to be associated with varus collapse initiated by overloaded edge loading. 4 A previous study 21 involving 10 patients sustaining 2-part PHFs with medial column disruption showed a high rate of reduction loss or varus collapse.
To date, the existing studies on the outcomes of the PHILOS plate plus oblique insertion of autologous fibula remain lacking. Erasmo et al. 24 reported the role of the PHILOS plate and showed remarkable dissimilarities. Attention has been attracted to whether the PHILOS plate in treating 2-part PHFs with medial column disruption has a low rate of either reduction loss or varus collapse in accordance with mid- and long-term follow-up outcomes. 25,26 Zhang et al. 27 explored the effect of fixation with calcar screws and demonstrated that fracture stability with the highest strength and minimum deformation was provided by fixation using 2 calcar screws. Based on a similar premise, Oppeboen et al. 28 reported a single-centre retrospective study of 190 adult PHF patients and revealed that 14 (7%) patients underwent a reoperation, predominantly ascribed to failing to achieve structural support of the medial column. Recently, Padegimas et al. 29 reported on 112 PHFs with medial column disruption and demonstrated that failure to restore the calcar predicts varus collapse.
There were several limitations in the current study. Firstly, the retrospective nature of this study is vulnerable to errors in evaluating baseline data and could lead to weakened power to draw robust conclusions. Although we tried to avoid confounding variables, the resulting analysis could remain flawed. Secondly, the lack of a control group in the study inevitably weakened the influence of other factors besides the research factors, such as the patient’s health level, activity level, and dietary habits. But whether to control these factors and how to control, we did not give a clear explanation. The evaluation of this surgical approach is limited. Therefore, it cannot be determined that the changes in research indicators are directly related to research factors. Thirdly, potential factors related to the surgeon’s practical experience could have an impact on the outcomes. Nonetheless, abiding by acknowledged procedures ensured that we optimized patient management. Although we had such limitations, we deemed that the error margin seemed to be permissible in this study.
Conclusion
The results reported in this study may support a growing body of evidence that older patients sustaining 2-part PHFs with medial column disruption stabilized using a PHILOS plate plus oblique insertion of autologous fibula as a primary procedure have a remarkable improvement in clinical outcomes, along with Constant and ASES scores as well as low rates of loss of reduction, varus collapse, screw penetration, avascular necrosis of the humeral head, aseptic loosening, mal- and non-union, periprosthetic fracture, revision, dislocation, deep infection, and intolerable shoulder pain. Nevertheless, on the basis of the data presented here, to determine other clinical benefits, such as the prosthesis survival curve, future studies may be needed.
Footnotes
Authors’ Note
Jiali Yu and Meiji Chen contributed equally to this work. Xiangzhen Liu is nos affiliated with Department of Oral and Maxillofacial Surgery, The First Affiliated Hospital, Sun Yat-sen University, Yuexiu District, Guangzhou, China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.