
Abstract
Purpose:
To evaluate the short-term clinical and radiological outcomes with degenerative changes in patients over 40 years old following isolated vertical medial meniscal tear repair.
Methods:
Between 2007 and 2015, 438 patients underwent arthroscopic meniscal repair. Thirty-three patients aged over 40 years with isolated vertical medial meniscal repair (23 males and 10 females, mean age 46.1 ± 7.0; range 40–67) were included in the study. Preoperative and postoperative physical examination findings, Lysholm knee score, the International Knee Documentation Committee score, magnetic resonance imaging findings, and Kellgren–Lawrence osteoarthritis stage were evaluated.
Results:
The mean follow-up period was 31.1 months ± 20.1 (range 12–100 months). There was statistically significant improvement in functional scores (p < 0.05) and physical examination findings. In 22 patients (66.7%), improvement in the clinical and radiological results was detected (p < 0.05). However, no correlation was found between clinical and radiological outcomes. There was also no significant change in osteoarthritis stages at the last follow-up visit. No significant difference was found between smokers and nonsmokers regarding clinical outcomes.
Conclusion:
Successful clinical and radiological outcomes can be obtained following isolated vertical medial meniscal tear repair in patients older than 40 years. Age is not the sole criterion for the success of meniscal repair; rather, the functional capacity of the patient, the location of the tear, the grade of knee joint arthritis, and the quality of the meniscal tissue should be taken into consideration.
Introduction
Menisci are involved in providing load transfer, knee stability, and shock absorption. 1
Approximately 25% of patients with meniscus lesions undergo surgical procedures, such as meniscal repair or meniscectomy. 2 In symptomatic patients, meniscal function can be preserved by partial meniscectomy in which the peripheral rim is left intact. 3,4 However, meniscectomy has long-term side effects, such as osteoarthritis, and therefore a meniscal lesion should be repaired if possible. 5 The recognition of the functional importance of menisci has led to radical changes in the treatment of meniscal injuries. 6
Meniscal healing is affected by various factors, such as age, tear pattern, location, size and extent, concomitant injuries, repair time and technique, and patient habits. 7 Repairs of acute longitudinal tears located in the red–red zone in young adults with a stable knee have been reported to have the most successful results. 8 Repairable meniscus tears are more likely to be seen in young people, as age increases, meniscal degeneration increases and healing is adversely affected; thus, the percentage of successful repair of meniscus tears is lower in middle- and advanced-age patients compared to younger patients. 9
To the best of our knowledge, only few studies evaluated the clinical and radiological outcomes following meniscal repairs in patients older than 40 years, 10 –14 and there is no specific study that examined these outcomes following isolated vertical medial meniscal tear repair in this patient group. Thus, in this study, we aimed to evaluate the clinical and radiological outcomes following arthroscopic meniscal repair of isolated vertical medial meniscal tears in patients older than 40 years.
Methods
Between January 2007 and January 2015, 438 patients underwent isolated arthroscopic meniscal repair in our hospital. Patients who did not respond to conservative treatment before surgery were selected. Conservative treatment protocol included physical theraphy (managing swelling while maintaining knee range of motion, quadriceps and hamstring strengthening, dynamic proprioceptive training, and conditioning). 15 In the follow-up period, patients who did not respond to conservative treatment underwent arthroscopic meniscal repair. Inclusion criteria were being aged 40–70 years and having an isolated vertical longitudinal medial meniscal tear of 10–30 mm caused by trauma or sports injury, lasting more than 8 weeks (chronic), and involving red–red or red–white zones. Patients were excluded from the study if they had advanced knee osteoarthritis, knee ligament injury, history of previous knee surgery, lateral meniscal tear, radial, bucket-handle, horizontal, flap, discoid or degenerative tear, patellofemoral joint instability, or lower extremity deformity (Figure 1). To achieve homogenous and trauma and sports injury-related sample, vertical medial meniscal tears were selected and collected. As a result, a total of 33 patients participated in the study. The study was approved by the institutional review board of our hospital (November 11, 2015—33).

Flowchart showing exclusion steps and exact numbers of exclusions.
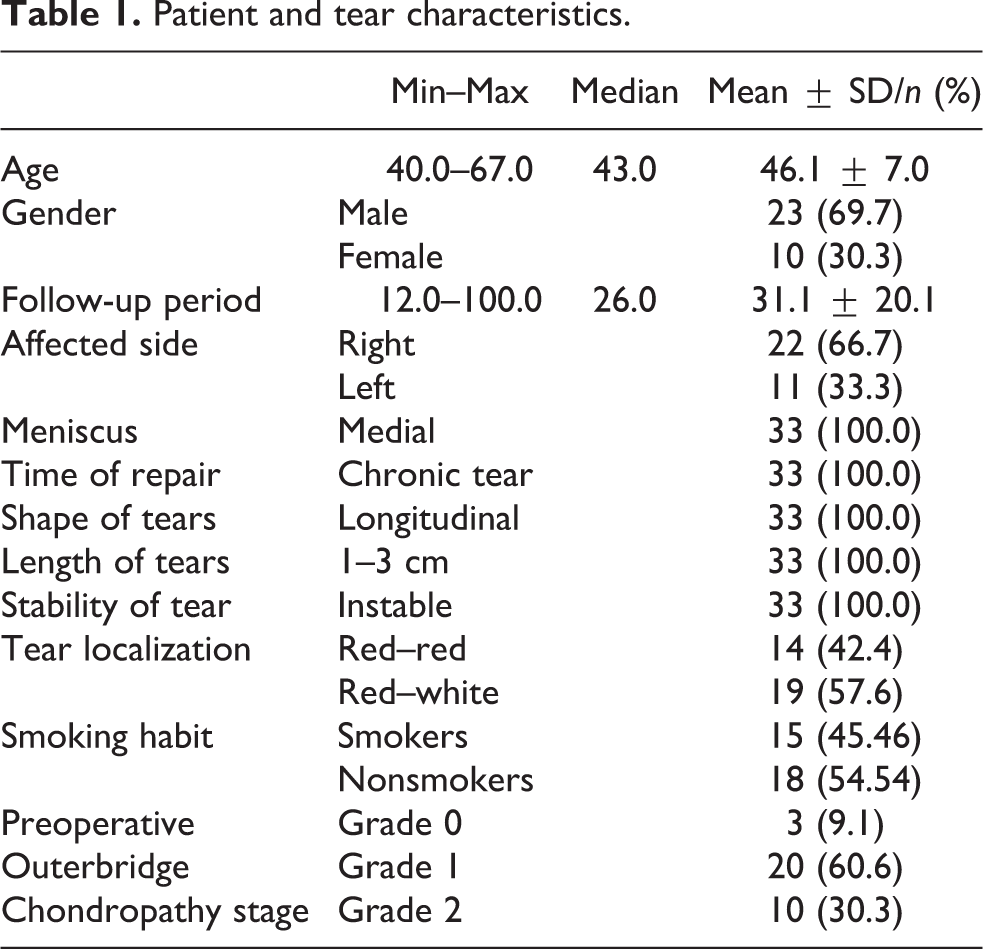
The mean age of the patients was 46.1 ± 7.0 years (range 40–67 years). The mean follow-up period was 31.1 ± 20.1 months (range 12–100 months). Patient demographics, tear characteristics, and preoperative outerbridge chondropathy grades are summarized in Table 1. Pars intermedia and/or posterior horn was involved in all tears. All-inside or inside-out repair technique was used in all cases. The medical history, physical examination findings, weight-bearing anterior–posterior (AP) and lateral knee radiographs, and knee magnetic resonance (MR) images were obtained for all patients in the diagnosis and follow-up periods. In the evaluation of functional outcomes, the preoperative and last follow-up Lysholm and International Knee Documentation Committee (IKDC) scores were used. 16,17
Patient and tear characteristics.
Patient symptoms and Barrett criteria were used in the evaluation of clinical outcomes. The absence of joint tenderness, effusion and locking, and a positive McMurray test was considered to be indicative of a healed meniscus. Unfavorable outcomes in any of the scoring or examination measures were considered clinical failures. 11
MR imaging was used in the evaluation of radiological healing. Postoperative MR imaging was performed routinely on average 1 year postoperatively. The MR images were examined by an experienced musculoskeletal radiologist and the senior author. MR imaging was performed with a 1.5-T scanner (Magnetom Aera, Siemens AG, Erlangen, Germany) with a dedicated array coil. All images had a 4-mm slice thickness. The Henning criteria were used to evaluate the signal level in the repaired area. Accordingly, the tears were considered to be completely healed if there was an increase in the signal intensity in <10% of the meniscus vertical height in the torn area, partially healed if it was <50%, and unhealed if it was >50%. 18
Knee joint osteoarthritis stage was evaluated by the Kellgren–Lawrence osteoarthritis grading system on the preoperative and last follow-up weight-bearing AP and lateral knee radiographs. 19
Arthroscopic procedures were performed under regional anesthesia by two experienced orthopedic surgeons. In the surgical procedures, routine anterolateral and anteromedial portals were used. All the knee compartments and meniscal tears were examined, and the tear was measured with an arthroscopy probe. Stability was checked; localization of the tears (red–red, red–white zones) and affected parts (pars intermedia, posterior horn) were determined. Tears within 2 mm of the meniscocapsular region were considered as the red–red zone, and 2–4 mm were considered as the red–white zone. 20
The repair was performed using all-inside suture in 21 patients and hybrid method (all-inside and inside-out) in 12 patients, depending on the extension and location of the tear. A vertical or oblique suture configuration was used in all repairs. All-inside sutures were used in the posterior horn and body of the meniscus repairs, and inside-out sutures were utilized for the body of the meniscus. A Fast-Fix meniscus fixator (Fast-Fix™ 360, Smith & Nephew, Andover, Massachusetts, USA), RapidLoc (DePuy Mitek, Raynham, Massachusetts, USA) or Meniscal Cinch (Arthrex, Naples, Florida, USA) was used for the all-inside approaches, and #0 Polydioxanone sutures (PDS) (Ethicon Inc., Somerville, New Jersey, USA) for the inside-out method.
Postoperatively, 3 of the 33 (9%) patients had temporary hypoesthesia on the medial side of the calf, and 2 patients had a superficial infection. Hypoesthesia of these patients was spontaneously resolved within 6 months. After 2 weeks of oral antibiotherapy, superficial infections were regressed. At the last follow-up examination, none of the patients had hypoesthesia or infection finding.
The participants were allowed to mobilize with a support on the first postoperative day. Weight bearing was restricted until 6 postoperative weeks. Isometric quadriceps exercises were commenced on postoperative day 1. The range of motion exercises was started on postoperative day 1 using a continuous passive motion machine; 10° of flexion increase every day was planned. The patients were discharged when they were able to perform a straight leg raise and had 90° knee flexion. Quadriceps exercises with weights were started immediately. Full weight bearing was allowed 6 weeks postoperatively. At the end of the sixth month recovery period, the patients were allowed to return to sport activities in accordance with their healing and rehabilitation status.
Descriptive statistics, including the mean, standard deviation, median, lowest, highest, frequency and ratio values were obtained preoperatively and at the last follow-up visit. The distribution of the variables was measured by the Kolmogorov–Smirnov test. The Mann–Whitney U test was performed to analyze the quantitative independent data. The Wilcoxon test was employed to analyze the quantitative dependent data. The independent qualitative data were analyzed by the χ 2 test or the Fischer test if the χ 2test conditions were not met. SPSS version 22.0 (IBM Inc. Chicago, Illinois, USA) was used for all statistical analysis.
Results
All patients had at least one physical examination finding. At the last follow-up, 11 patients (33.3%) had one or more physical examination findings, joint line tenderness in 7 patients, a positive McMurray’s test in 3 patients, and effusion in 6 patients. (5 patients had two or more physical examination findings.) It was found that the decrease in the number of patients with at least one physical examination finding before surgery was significant (p = 0.000) (Table 2).
Pre- and postoperative physical examination findings and osteoarthritis stages of patients.

aMc-Nemar test.
Compared to the baseline values, there was a significant improvement in the postoperative Lysholm knee score
Functional results.

IKDC: International Knee Documentation Committee.
aWilcoxon test.
According to the Henning criteria, 22 tears were completely and partial healed, and 11 tears were unhealed (Table 4). There was no correlation between radiological, functional, and clinical findings in terms of healing (p > 0.05; Tables 5 and 6). Preoperatively, 14 patients had stage 0 and 19 patients had stage 1 osteoarthritis. At the last follow-up, 13 patients had stage 0, 18 had stage 1, and two had stage 2 osteoarthritis. Statistical analysis revealed that the postoperative osteoarthritis of the knee joints of the patients did not change significantly compared to the preoperative status (p > 0.05; Table 2). Similarly, the preoperative and postoperative Lysholm and IKDC values did not significantly differ (p > 0.05) in the smoker and nonsmoker groups (Table 7). There was also no statistically significant difference between the smokers and nonsmokers in terms of the distribution of patients with at least one physical examination finding before and after surgery (p > 0.05; Table 8).
Radiologic healing results.

Functional results of radiologically healed and unhealed patients.

IKDC: International Knee Documentation Committee.
aMann–Whitney U test.
bWilcoxon test.
Pre- and postoperative physical examination findings of radiologically unhealed and healed patients.
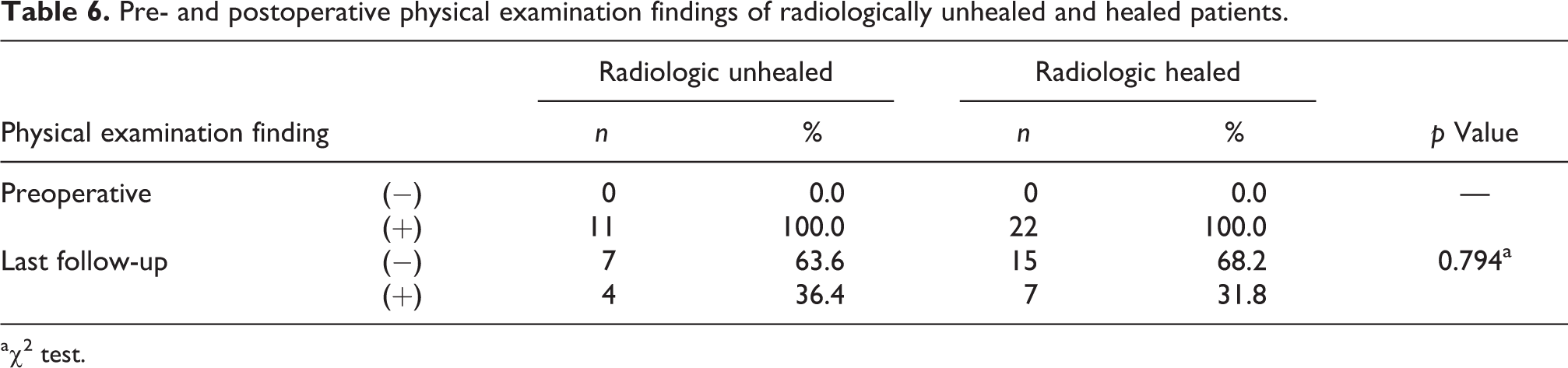
a χ 2 test.
Functional results of nonsmoker and smoker patients.

IKDC: International Knee Documentation Committee.
aMann–Whitney U test.
bWilcoxon test.
Pre- and postoperative physical examination findings of nonsmoker and smoker patients.
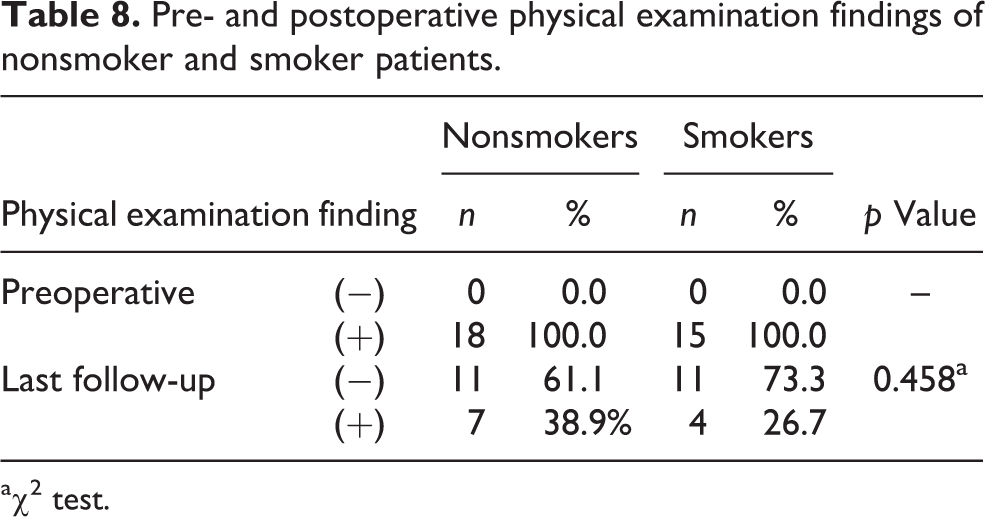
a χ 2 test.
Discussion
Despite the decrease in meniscus vascularity as people age, it has been shown that patient age does not affect meniscus healing. 10,11 However, to date, studies in this area have been conducted only with patients selected heterogeneously. In the current study, the patient group consisted of patients who had undergone isolated arthroscopic vertical medial meniscal tear repair. This is the main difference between our work and previous research.
Henning et al. 21 and Belzer et al. 22 suggested that isolated meniscus tear repair in stable knees might have a lower incidence of healing than meniscus repair combined with anterior cruciate ligament (ACL) reconstruction. Similar studies with Cannon and Vittori, 20 Barrett et al., 11 and Noyes and Barber-Westin 10 reported a high rate of clinical improvement in older patients with concomitant meniscal repair with ACL reconstruction. For example, in a minimum 2-year follow-up study, Barrett et al. 11 showed clinical improvement in 86.5% of 37 male patients aged 40 years, who had undergone arthroscopic meniscal repair. However, 4.5% clinical failure was found in patients with concurrent ACL reconstruction, and 26.5% clinical failure was seen in isolated meniscal repair. 11 Our study showed a statistically significant increase in functional recovery compared to preoperative values (increase in the Lysholm and IKDC scores), which indicated improvement in 66.7% of patients in addition to the physical examination findings. The clinical improvement ratio of our study was lower than that of similar studies because concurrent anterior cruciate ligament reconstruction and meniscal repair was not included in our study.
Conservative treatment including physical therapy remains a successful option for mitigating pain and functional deficits after a meniscal tear. 23 Initial nonoperative management of meniscal tears is dependent on clinical presentation and is typically reserved for patients who do not have severely restricted range of motion, locking, or instability of the afflicted knee. 23 Yim et al. 24 compared the conservative treatment and meniscectomy for degenerative horizontal tears of the posterior horn of the medial meniscus. There was no significant difference in patient satisfaction pain and function at 2-year follow-up. In another study, investigating the effect of conservative treatment in patients with degenerative medial meniscus tear at an average follow-up of 35 months, improvement in the functional knee scores up to 6 months was achieved. However, it was accompanied by a decline and osteoarthritis progressed later. 25 Conservative treatment was the first-line treatment in all patients in this study. However, in the follow-up period, the patient complaints continued and surgical treatment was performed.
It has been reported that whereas isolated partial meniscectomies have lower reoperation rates than meniscal repairs in the short (0–4 years) and long (>10 years) term (1.4% vs. 16.5% and 3.9% vs. 20.7%), and meniscectomies have better long-term outcomes. 26 In our short-term study, three patients (9%) required reoperation after isolated medial meniscal repair.
In their systematic review, Paxton et al. 26 reported one grade or less change in osteoarthritis in 97% of meniscal repairs and in 88% of partial meniscectomies after minimum of 10-year follow-up. In our short-term follow-up study, one patient with grade 0 and one patient with grade 1 OA (7%) progressed one grade. In the same systematic review (11 meniscal repair studies had been assessed) meniscal healing was evaluated using second look arthroscopy and they found that overall 61.7% of the menisci were completely healed and 17.4% were not healed. 26 We evaluated meniscal healing using MRI. According to our results, partial or complete healing was detected in 67.7% (22 of 33 patients) of the patients. It was slightly higher than previous reports.
In the literature, there has been only one study comparing the long-term outcomes in patients 40 years and older underwent arthroscopic meniscal repair. 27 They included 33 medial meniscal repairs in patients older than 40 years. They found similar failure rates in older and younger patients (5.3% vs. 5.5%). They used subsequent surgery history and reports to determine failure. Also, high function and patient satisfaction were reported on an average of 16 years after meniscal repair. Our study included only traumatic vertical medial meniscal tear repairs. Our failure rates were comparable with previous reports but not with Steadman et al. 27 This mismatch may be due to failure evaluation methods.
MR imaging is noninvasive and easily accessible facilitating usability evaluation after meniscus repair. Miao et al. 28 reported that MR imaging had a sensitivity of 92% and a specificity of 99% for the radiological evaluation of meniscal healing. Willinger et al. 29 found this imaging method successfully demonstrated 87% complete or partial healing after arthroscopic repair in acute meniscal tears.
Eggli et al. 30 reported that meniscal healing might be seen in the MR examination of patients without clinical symptoms. They showed that all the patients evaluated as failed repair on MR examination had clinical symptoms and that clinical improvement correlated with radiological recovery. In the current study, meniscal healing was assessed by MR imaging, and it was found that 67.7% of the patients had partial or complete healing. However, there was no correlation between MR imaging and the clinical findings. Of the 11 patients with more than 50% signal presence at the repair site on MR examination, 4 had one or more physical examination findings. Seven other patients were asymptomatic with no physical examination finding. Increased signal presence in the meniscus repair area in seven asymptomatic patients in the study confirms that the meniscal fibrovascular repair tissue may be associated with the persistent signal on MR examination. However, the long-term persistence of these signals is unknown.
Another result we obtained in our short-term follow-up of this study is that meniscal repair prevented progression of knee joint arthritis in elderly patients. This result is consistent with the current literature and is important for the evaluation of elderly patients with isolated meniscal tear repair. Long-term studies have shown increased degenerative changes after meniscectomy. 31 –33 Therefore, where possible, arthroscopic repair of the torn meniscus is now the treatment of choice. Today, the role of menisci in preventing arthritis of the knee joint is well known.
The current literature suggests that cigarette smoking has an adverse effect on the outcomes of knee ligament and meniscus repair and that smoking cessation will benefit patients in these repairs. 34 –36 However, in our study, there were no differences regarding clinical and functional improvement between smokers and nonsmokers in the elderly patients.
Retrospective nature of the study, exclusion of other types of medial meniscus and all of lateral meniscus tears, the absence of a control group, lack of long-term follow-up results, and the evaluation of radiological healing only with MR imaging were the limitations of this study.
Conclusion
As supported by the results of our study, age is not the sole criterion for the success of meniscal repair; rather, the functional capacity of the patient, the location of the tear, the grade of knee joint arthritis, and the quality of the meniscal tissue should be taken into consideration. The protective effect on the meniscus, especially in the degenerative process, can also be considered. Further comparative and long-term studies are needed to provide more precise data.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.