
Abstract
Unicompartmental knee arthroplasty (UKA) in anterior cruciate ligament deficiency (ACLD) has been debated for decades after the development of highly cross-linked polyethylene. This study aims to evaluate the effect of posterior tibial slope on restoring adequate knee stability and flexion after UKA in patients with ACLD. A total of 15 fresh cadaveric knees were divided into three groups: intact ACL, partial ACLD, and complete ACLD. Fixed-bearing UKAs including 3-D-printed tibial inserts with the slopes ranging from 3° to 12° were performed using computer-assisted navigation. Blinded evaluation of knee motion and anterior knee translation with knees flexed 20° and 90° was conducted using KT-arthrometry and stress radiography. A 1° slope increase translated the knees anteriorly by 0.85 mm and 0.76 mm in 20° and 90° of knee flexion for a complete ACLD (R = 0.7 and 0.8, respectively, p < 0.001) compared to 0.5–0.6 mm for the normal and partial ACLD groups, respectively. Setting a slope of 5–8° of UKA for an intact ACL maintained both the stability and the motion of native knees. No significant changes of knee translation and flexion ability were observed after leveling the slopes at 5–7° and 5–6° for partial and complete ACLD, respectively (p > 0.05 for all comparisons). In conclusion, UKA in complete ACLD knees is challenging since 1° of slope change nearly doubles the degree of knee translation compared to ACL-intact knees. The optimum posterior tibial slopes for fixed-bearing UKA patients with partial and complete ACLD are 5–7° and 5–6°, respectively.
Keywords
Introduction
Anterior cruciate ligament (ACL) injury is the primary constraint preventing anterior translation of the tibia on the femur and stabilization of the knee against rotational and valgus stress. 1 Recurrent knee injuries secondary to instability can aggravate intra-articular damage and progression of knee osteoarthritis (OA). Surgical treatment of medial compartmental OA with ACL deficiency is currently the state of the art. Specific aspects of treatment are determined by characteristics of the individual patient, knee instability, and surgeon preference.
Most patients with primary ACL injuries who develop secondary OA are usually young and active. The treatment with high tibial osteotomy (HTO) and ACL reconstruction has shown a high (21%) complication rate. 2 Unicompartmental knee arthroplasty (UKA) and ACL reconstruction are preferable and result in similar clinical outcomes to UKA in ACL-intact patients. 3,4 On the other hand, patients with primary OA due to a cartilage destruction and joint deformity may develop a secondary ACL instability. They are relatively older and less active compared to the secondary OA due to ACL injury. If the disease involves both the medial and the lateral knee compartments, total knee arthroplasty is considered the treatment of choice. However, there is no consensus on the treatment of isolated medial knee OA with secondary ACL instability, especially for patients over 55 and those who are less active.
UKA with ACL reconstruction is considered conceptually the best technique for normal knee kinematic restoration, since evidence has shown increased wear and aseptic loosening of the tibial component after treatment of an isolated UKA. 5,6 However, this technique is difficult to obtain a balanced ACL tension and motion after UKA. Recently, a development of highly cross-linked polyethylene in a fixed-bearing type UKA can decrease wear resulting from sliding and rolling motion. Balancing postoperative complications of UKA with ACL reconstruction with patient activity demands, the isolated UKA may be a reasonable option. 7 Both positive and negative outcomes have been reported after isolated UKA in medial OA patients with secondary ACL instability. 8,9 While indications and contraindications for UKA have never been clearly defined, tibial slope modification in case of ACL instability seems to be crucial to decreasing anterior sagittal displacement, similar to what has been reported for HTO. 2 However, the potential for decreased knee flexion subsequent to tibial slope modification should be taken into account.
To date, there have been only limited studies of the correlation between posterior tibial slope adjustment for UKA and anterior sagittal knee stability in patients with ACL deficiency (ACLD). According to previous studies, 10 –12 tibial slope more than 10° showed an excessive tibial translation and failure, and the slope less than 4° was recommended. This study aimed to investigate the relationship between posterior tibial slope and anterior knee translation with different ACL conditions, that is, ACL intact, partial ACLD, and complete ACLD, and to determine whether isolated UKA treatment for medial OA in patients with ACLD can restore normal anterior knee stability.
Materials and methods
Specimens and tibial component design
Fifteen fresh frozen cadaveric knees (mean age 64.26 ± 8.58 years; male:female = 12:3) were included in this study. Specimens that had undergone previous knee surgery or that had gross abnormality/instability of the knee were excluded. ACLDs were classified based on the integrity of the anteromedial (AM) and the posterolateral (PL) ACL bundles. As the AM bundle plays a major role in anterior instability, 13 specimens were randomly divided into three groups: intact both AM and PL bundles (five intact ACL, mean age 62 ± 9 years), AM bundle torn (five partial ACLDs; mean age 60 ± 5 years), and both AM and PL torn (five complete ACLDs; mean age 68 ± 8 years). There is no significant difference of demographic data including age, height, weight, BMI, and tibiofemoral angle between groups (p = 0.89, 0.85, 0.80, 0.75, and 0.65, respectively). The study protocol was approved by the institution’s Internal Review Board.
Custom-made trials of fixed-bearing tibial inserts with 1 of 10 degrees of slope (−4° to +5°) were designed using computer-aided design software (SolidWorks 15, USA) and manufactured using 3D printing techniques (Fused Deposition Modelling; Ultimaker B.V., Cambridge, MA, USA), as shown in Figure 1.
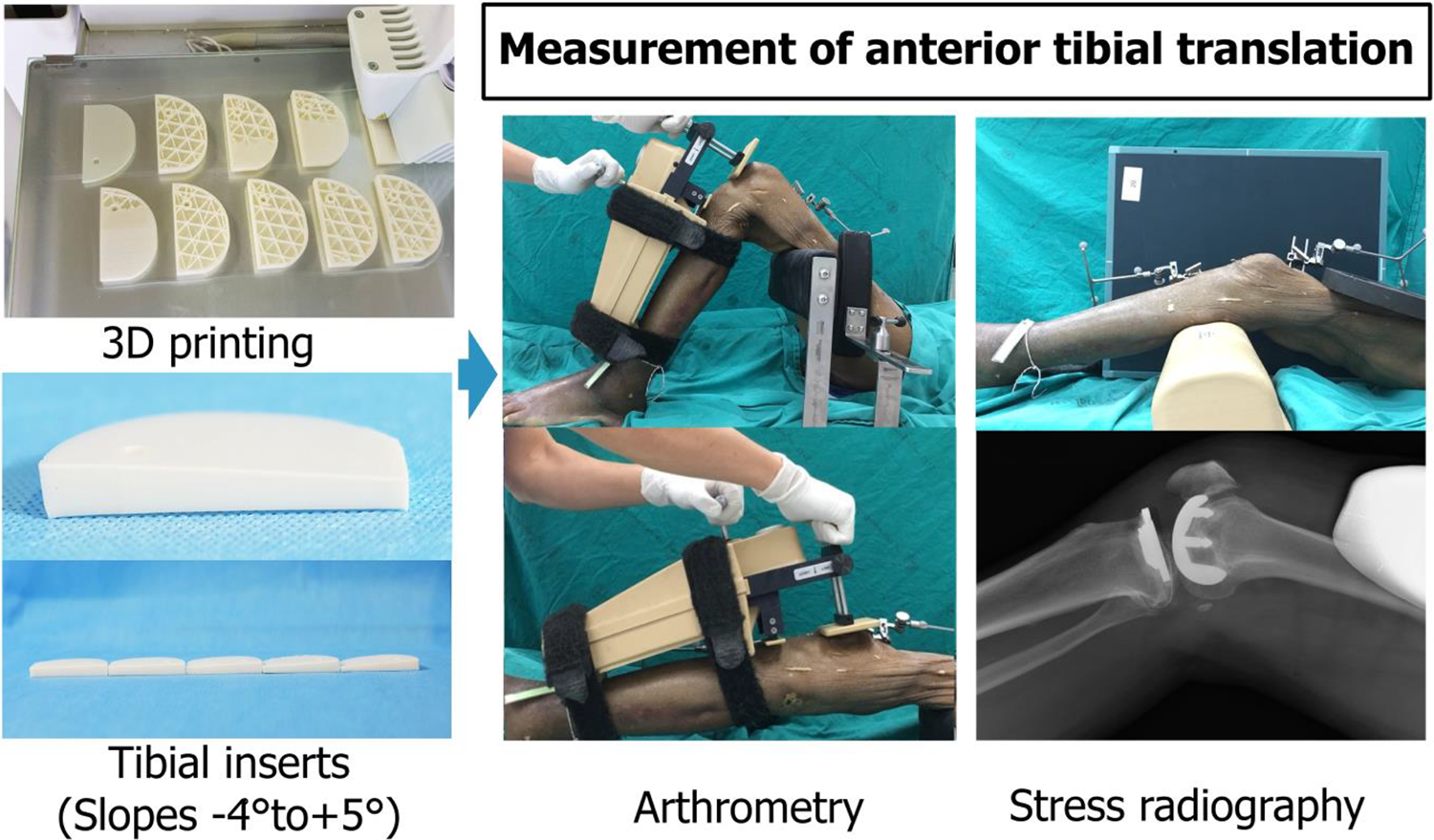
Using 3D-printing technology, customized tibial inserts with slopes ranging from −4° to +5° were made to create the slope variations used in this study. Anterior tibial translation was tested using arthrometry techniques at knee flexion of either 20° or 90° and stress radiography.
Surgical procedures
Specimens were thawed for 48 h at room temperature before surgery. A fixed-bearing medial UKA (Synthes Joint Reconstruction SIGMA® High Performance Partial Knee System; DePuy Johnson & Johnson, USA) was done using a computer navigation-assisted system (Knee Navigation System KNEE3®, Brainlab, Germany). Specimens in which intraoperative visualization revealed ACLD were excluded from the study. Native anterior knee translations and knee range of motion were measured as a reference before an experiment. The surgical procedure was performed with mini-medial parapatellar approach by one senior surgeon. The thickness of proximal tibial cut contributed to the degree of knee extension and coronal alignment. 14 Proximal tibial bone cut that resulted the extension medial joint gap of 7 mm and the proximal tibial slope of 7° were targeted under the navigation. Hence, after inserting the custom-made tibial inserts (7-mm thickness), the ability of anterior knee translation and knee flexion angle will be varied regarding with the different angles of posterior slope ranging from 3° to 12° with a difference of 1°.
Knee capsule and surgical site closure using standard sutured was performed to reestablish soft-tissue integrity before each test.
Testing protocol
Native anterior knee stability was evaluated prior to surgery. Tibiofemoral angle and medial and lateral gaps throughout the range of knee motion after UKA were recorded using the navigation software to confirm adequate coronal knee correction. A second surgeon who was blinded to the degree of slope assessed the anterior knee stability using two testing methods: knee arthrometry (KT-2000, MEDmetric, San Diego, CA, USA) 15 at both 20° and 90° of knee flexion and stress radiography 16 with the knee flexed 20° (Figure 1).
Statistical analysis
The cohort size was calculated using the non-inferiority trial with continuous outcome formula. According to Myrer et al., 17 the non-inferiority margin of KT arthrometry is 3 mm. Therefore, the minimum sample size of 5 in each group was enough to achieve the power of study at 80% with the statistical significance at p ≤ 0.05. Pearson’s correlation was used to determine the association between the degree of posterior tibial slope and the anterior tibial translation. One-way ANOVA and Tukey’s method were performed to detect significant mean translational differences between the groups and subgroups.
Results
All 15 specimens showed mild varus angulation (3–7°) and normal anterior knee translation (average 4.63 ± 1.63 mm and 2.71 ± 1.3 mm with knee flexed at 20° and 90°, respectively) with full passive flexion of 130–150° and extension of 0–4°mm (Table 1).
Demographic data and preexperimental parameters between normal ACL, partial ACL deficiency, and complete ACL deficiency.
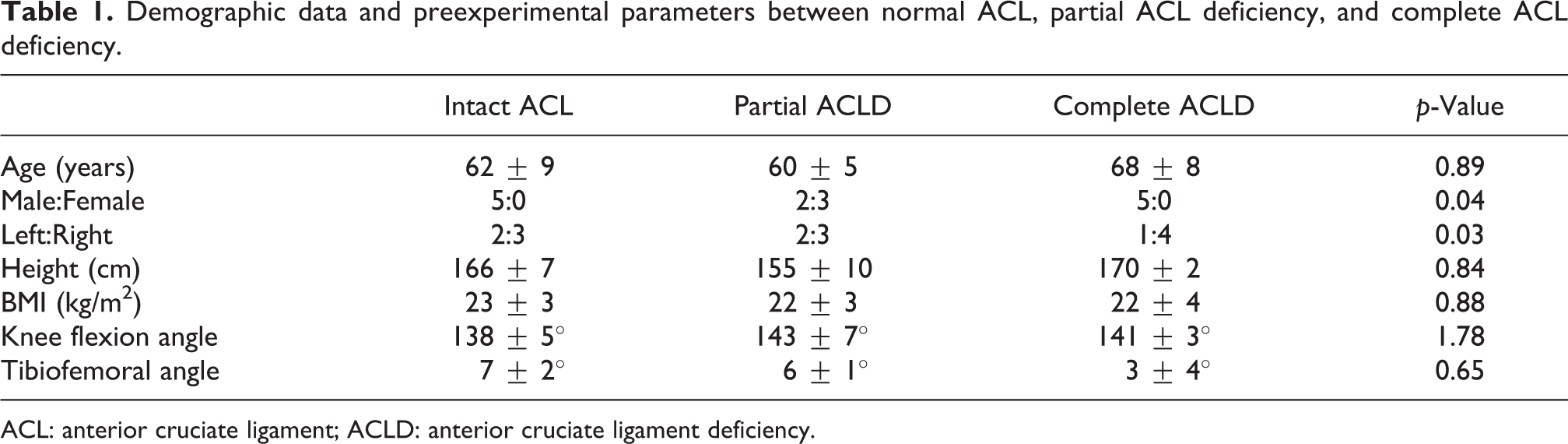
ACL: anterior cruciate ligament; ACLD: anterior cruciate ligament deficiency.
Correlation between posterior tibial slope, anterior tibial translation, and knee flexion and extension
The greater the posterior tibial slope, the greater the distance the knees were translated. The degree of anterior knee translation showed a significant linear correlation with the degree of posterior tibial slope with knees flexed at 20° and 90° in all study groups (p < 0.001) (Figure 2(a) and (b)). Measurements indicated that each additional 1° of posterior tibial slope increased the anterior tibial translation by 0.48 mm and 0.52 mm with knees flexed 20° and 90°, respectively, for specimens with intact ACL (R = 0.6 and 0.7, respectively). Results were similar for 0.52-mm and 0.41-mm translation in knees flexed 20° and 90° in specimens with partial ACLD (R = 0.6 and 0.5, respectively). However, greater anterior tibial translations were observed for each degree of slope increase in the complete ACLD group (increases of 0.85 mm and 0.76 mm for knees flexed 20° and 90°, R = 0.7 and 0.8).

Influence of posterior tibial slope modification on anterior tibial translation at knee flexion of 20° (a) and 90° (b) and knee flexion ability (c).
Increased posterior tibial slope also significantly increased the degree of knee flexion in all groups (p < 0.001, 0.02, and 0.01 for intact ACL, partial ACLD, and complete ACLD, respectively, Figure 2(c)). While the slope and degrees of knee flexion exhibited a linear correlation for specimens with intact ACL (R = 0.5), the relationship was less linear for specimens with ACLD (R = 0.1 and 0.3 for partial ACLD and complete ACLD, respectively).
Changing the slope did not affect the knee extension ability. All specimens showed the knee extension angle ranging from 0° to 4°. This indicated that changing the posterior tibial slope did not alter the knee extension gap.
Posterior tibial slope optimization for ACLD
Posterior tibial slopes between 5° and 8° successfully maintained both anterior tibial translations (5.0 ± 1.6 mm and 3.1 ± 1.4 mm for knee flexion of 20° and 90°, p = 0.21 and 0.28, respectively) and increased knee flexion from 140° ± 5° to 143° ± 4° after UKA for an intact ACL (p < 0.01). For specimens with partial ACLD, UKA with a slope of 5–7° attained anterior knee stability similar to an intact ACL with translation of 4.6 ± 2.2 mm and 3.6 ± 1.4 mm for knees flexed 20° and 90° (p = 0.27 and 0.17) without restriction for knee flexion (143° ± 7° and 144° ± 5° for native knee and UKA, respectively, p = 0.32) (Figure 3(b)). With completely torn ACL, isolated UKA with a posterior tibial slope of 5–6° restored normal anterior tibial translation (5.8 ± 2.3 mm and 3.4 ± 1.0 mm for knees flexed 20° and 90°, p = 0.10 and 0.14, respectively) with no effect on knee flexion (141° ± 3° and 143° ± 3° for native and UKA, p = 0.15) (Figure 3(c)).

Illustrating anterior tibial translations with optimized posterior slope for intact ACL (a), partial ACLD (b), and complete ACLD (c); *statistically significant.
Stress radiography was used to confirm the arthrometry measurements by evaluating anterior tibial translations of 4°, 7°, and 10° of posterior tibial slope. UKA with a posterior tibial slope of 4° showed normal anterior tibial translation for specimens with both partial and complete ACLD (p = 0.31). Conventional cutting of posterior tibial slopes at 7° and 10° increased anterior knee translation (p = 0.01 and <0.001, respectively) (Figure 4).

Anterior tibial translation at 4°, 7°, and 10° of posterior tibial slope from stress radiographic tests. ACL: anterior cruciate ligament; ACLD: anterior cruciate ligament deficiency.
Discussion
Restoration of native articular joint line and tibial slope angle is the treatment goal of UKA. However, the slope modification is important when loss of knee stability for ACLD. The benefit of an increased posterior tibial slope had been recommended to increase knee flexion and femoral rollback and promote stress distribution at the bone–tibial component interface. Hernigou and Deschamps 10 argued the increased posterior slope does not improve mobility but cause progressive disruption of ACL occurred over time in relation to the posterior slope of the tibial component more than 7°–9°. Excessive leveling posterior slope angle also leads to excessive stress and ACL avulsion on the other hand. 18 There is no clear cut of the adequate slope angles performed for patients during ACL insufficiency; however, a high survivorship was observed after UKA when leveling posterior tibial slope.
This fixed-bearing UKA study primarily demonstrates the effect of posterior tibial slope on anterior knee stability with and without the presence of ACL. Every 1° of slope modification creates 0.48–0.52 mm of gap for UKA patients with intact and/or sufficient ACL function, compared to 0.76–0.85 mm for patients with insufficient ACL (completely torn). Although the effect of posterior tibial slope on anterior tibial translation has been described in previous studies, 10,11,19 this study emphasized that this correlation does not result in reduction of knee flexion ability in knees with ACLD.
The physiological lateral knee ligament gap is typically wider than on the medial side, and both the extension and flexion gaps are increased after ACL resection. 20 Tightening both flexion and extension gaps in the medial compartment by creating an optimum tibial slope for UKA increases anterior stability while preserving the functional range of knee flexion. Medial gap tightening may also allow physiologic tibial internal rotation in deep flexion due to reduced constraint on the lateral knee. 12 The results might be changed if the disease involved to the lateral knee compartment leading to the tightening of the lateral knee ligament. Our study determined the optimum range of tibial slope for each ACL condition, 5–7° for partial ACLD and 5–6° for complete ACLD and successfully restored anterior knee stability after UKA. A decrease in sliding and rolling distance may reduce abrasive wear; however, it can result in an overstuffed knee gap, producing concentrated stress which results in surface cracking on the highly cross-linked polyethylene liner. 21
Long-term clinical outcomes of fixed-bearing UKA with leveling posterior tibial slope techniques for patients with ACLD are less well known. Engh and Ammeen 8 reported similar 6-year UKA survivorship in ACLD knees (94%) and ACL-intact knees (93%). There have been no published reports, however, of functional outcomes of this procedure. Based on a biomechanical study, Suero and Citak 12 reported that leveling the tibial slope did not restore rotational stability although it could successfully restore the anterior stability. This suggests that isolated UKA with tibial slope leveling may not be the best option for younger patients with medial OA secondary to ACL injury where reduction of rotational instability is a main goal of the treatment. On the other hand, the posterior tibial slope leveling procedure is a reasonable option for treatment of ACL insufficiency secondary to medial OA in older adults due to lower functional demands. No difference of failure modes was noted between UKA with and without the presence of ACL. 8
Although isolated UKA with tibial slope leveling could restore enough stability in ACL insufficient knees. However, it does require precise measurement of the tibial bone cut. There is only a 1°–2° target range which can produce a balance between anterior tibial translation and knee flexion for UKA with complete ACLD. Recent technological advances, for example, robotics, computer-assisted navigation, and custom sawing jigs are recommended to help achieve target tibial slope leveling during the UKA procedure.
This study should be interpreted in the light of its potential limitations. One potential limitation was the measurement method itself. KT-2000 arthrometer has been considered as the standard measurement technique with high reliability and accuracy. 15,17 We also optimized the reliability of the test by assigning the same surgeon to perform all arthrometer tests three times each to eliminate inter- and intra-observer variation. However, subjective measurement problem can occur and might affect the results. Another limitation was the experiments in vitro cannot mimic the in vivo kinematics during functional activities and so the optimum slopes in in vivo may be changed. However, this cadaveric study preliminarily showed the advantages of slope modifications for UKA patients with ACLD. Further studies on kinematics, component wear, rotational stability, and component failure are needed to predict long-term outcomes of isolated fixed-bearing UKA in ACLD knees.
Conclusions
Unlike invasive total joint replacement, isolated UKA with posterior tibial slope leveling is a reasonable treatment option for older patients with ACLD secondary to medial OA knee as anterior knee stability can be restored while maintaining a functional range of knee flexion. UKA in complete ACLD knees is challenging since a 1° slope change nearly doubles the degrees of knee translation compared to ACL-intact knees. The optimum posterior tibial slope of fixed-bearing UKA for patients with partial and complete ACLD is 5–7° and 5°–6°, respectively.
Footnotes
Acknowledgements
The authors would like to express their sincere thanks to Dr G. Lamar Robert and the Cadaveric Surgical Training Center, Faculty of Medicine, Chiang Mai University for providing the cadavers used in this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DePuy Synthes, a Johnson & Johnson company, donated the implants and the computer-assisted navigation system used in this study. The authors have no professional or financial affiliations to this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) recieved financial support from faculty of medicine, Chiang Mai university for the research, authorship, and/or publication of this article.