
Abstract
Purpose:
To determine an easy and convenient method of sacral-alar-iliac (S2AI) screw fixation and introduce the surgical landmarks for fluoroscopic procedure by analyzing 3-D models of pelvis and virtual implantation in a 3-D model.
Materials and Methods:
Eighty-two cadavers underwent computed tomography scans and the images imported into Mimics® software to make the 3-D pelvis model. The pedicle screw (Ø 8.5 mm/length 115 mm) was processed into a 3-D model using a 3-D-sensor (Comet5®) at the actual size and virtually placed as the S2AI screw. The ideal screw position was defined as the maximal intraosseous length without cortical perforation along the entire path. The ideal entry point and screw trajectory were verified and assessed to introduce the surgical landmark for fluoroscopic procedure.
Results:
There was no cortical violation around nerve root canal and greater sciatic notch through the entry point between first and second dorsal sacral foramen. There was no impossible model of S2AI screws. The average screw length was 99.8 mm (range, 59.8–115 mm; standard deviation, 16.1) and just one model had shorter than 65 mm S2AI screw. The factors limiting the intra-iliac screw length were sex (p = 0.000) and the iliac groove around the sacroiliac joint (p = 0.000). A free 360° rotation with magnification revealed that the screw trajectory was consistently directed toward the anteroinferior iliac spine (AIIS) in any plane.
Conclusion:
The ideal entry point of S2AI screw showed a wide range of tolerance between the first and second dorsal sacral foramen; and thus, there was no need for deep dissection to identify the first dorsal sacral foramen. Considering the tendency to shift the pilot hole laterally and the ideal screw trajectory was consistently directed toward AIIS, the entry point is better to be located with a medial shift.
Keywords
Introduction
Iliac screw fixation in the lumbopelvic construct is an important factor for the prevention of pseudoarthrosis and fixation failure. 1 –3 Although iliac screw fixation has been used as general option, this requires separate fascial or skin incisions or the use of connecting rod, extensive dissection to expose the entry point, prominent discomfort to patient, and sacrificing the posterosuperior iliac spine. 2 Since the sacral-alar-iliac (S2AI) screw technique 4 –6 was described, it has emerged as an alternative option, which may address these limitations and result in improved biomechanical strength. 3,7 However, considering that the iliac screw has the intra-iliac position along the entire screw path, S2AI screw fixation might be more complicated and critical owing to the proximity to dorsal sacral foramen and greater sciatic notch and the penetration of the sacroiliac (SI) joint. Therefore, the technique of S2AI screw fixation is a challenge compared with iliac screw.
During the S2AI screw fixation, safety and technical success are ensured by clearly presenting the entry point and screw trajectory. Initially, a few authors 5,8 –10 described the entry point based on the first sacral dorsal foramen in millimeters through cadaveric or 3-D computed tomography (CT) imaging studies. O’Brien described that the use of S2AI screw might be limited by the articular cartilage violation, suggesting the need for evaluation of the short- and long-term effects because S2AI screw crossed the SI joint. 5 However, several clinical case series 1,2,11,12 and a biomechanical study 13 reported satisfactory clinical and biomechanical outcomes with minimal complication rate. They also observed that the screw trajectory should be directed toward the anteroinferior iliac spine (AIIS) and the screw length must be at least 65 mm without cortical perforation. 13 However, to the best of our knowledge, no studies demonstrated the optimal S2AI screw trajectory and simulated the cortical perforation by misplaced screws. We performed the computational simulation of S2AI screw fixation at actual size using 3-D rendering software.
The primary purpose of this cadaveric study was to identify a simple and convenient approach for S2AI screw placement via intentional malposition and introduce the surgical landmark for fluoroscopic procedure by analyzing 3-D pelvis models with virtual implantation.
Materials and methods
Digital data of the human body were collected from the Korean Institute of Science and Technology Information and used with permission. We enrolled 82 adult cadavers (40 females and 42 males) and none of the cadavers had pelvic problems based on a review of their records. The mean age of cadavers was 52.1 years (range, 21–60 years; standard deviation (SD), 9.2) and the mean height was 161.3 cm (range, 146–176 cm; SD, 7.1). All the cadavers underwent continuous 1.0-mm slice scans (Pronto; Hitachi, Tokyo, Japan) in the supine position. The CT data in Digital Imaging and Communications in Medicine (DICOM) format were imported into Materialise Interactive Medical Image Control System (Mimics®) software (Materialise, Antwerp, Belgium) to reconstruct the 3-D pelvis models including sacrum and two iliac bones. The 3-D pedicle screw model (Ø 8.5 mm/length 115 mm, L & K Biomed, Yongin-si, Korea) was created as a stereo-lithograph (STL) using a 3-D sensor (Comet5®; Carl Zeiss, Steinbichler, Germany) at the actual size to simulate the S2AI screw fixation.
After obtaining 3-D reconstructions of pelvis and pedicle screw, the simulated insertion of S2AI screw was performed using Mimics® software. Based on the original techniques, 1,2,4,10,14 the entry point and screw trajectory were selected using the moving tool of the software: (1) In the horizontal direction, the screw was started in the area between the first and second dorsal sacral foramen. (2) Based on the direct extension from the fifth lumbar and first sacral fixation constructs without connecting the rod, the entry point was chosen in the mediolateral direction. (3) In the iliac oblique view, the screw trajectory was nearest to the superior rim of greater sciatic notch. (4) In the pelvic inlet view, the screw was placed just lateral to the linea terminalis (Figure 1). For achieving the maximal intraosseous length of screw without cortical perforation along the entire screw path, the position of S2AI screw was fine-tuned via four synchronized windows composed of axial plane, coronal, sagittal, and 3-D biplanar images and verified definitively by an experienced surgeon (corresponding author). The S2AI screws were evaluated via free 360° rotations with magnification in any plane, and the features were assessed to introduce surgical landmarks for fluoroscopic procedure including the entry point, exit of screw tip, cortical violation around the screw path, and others. If the screw length was less than 65 mm, the model was assigned as short model (group). 13 To determine the location of the cortical perforation of S2AI screw, the moving tools of Mimics® software were used to simulate the intentional malposition according to the entry point and screw trajectory.
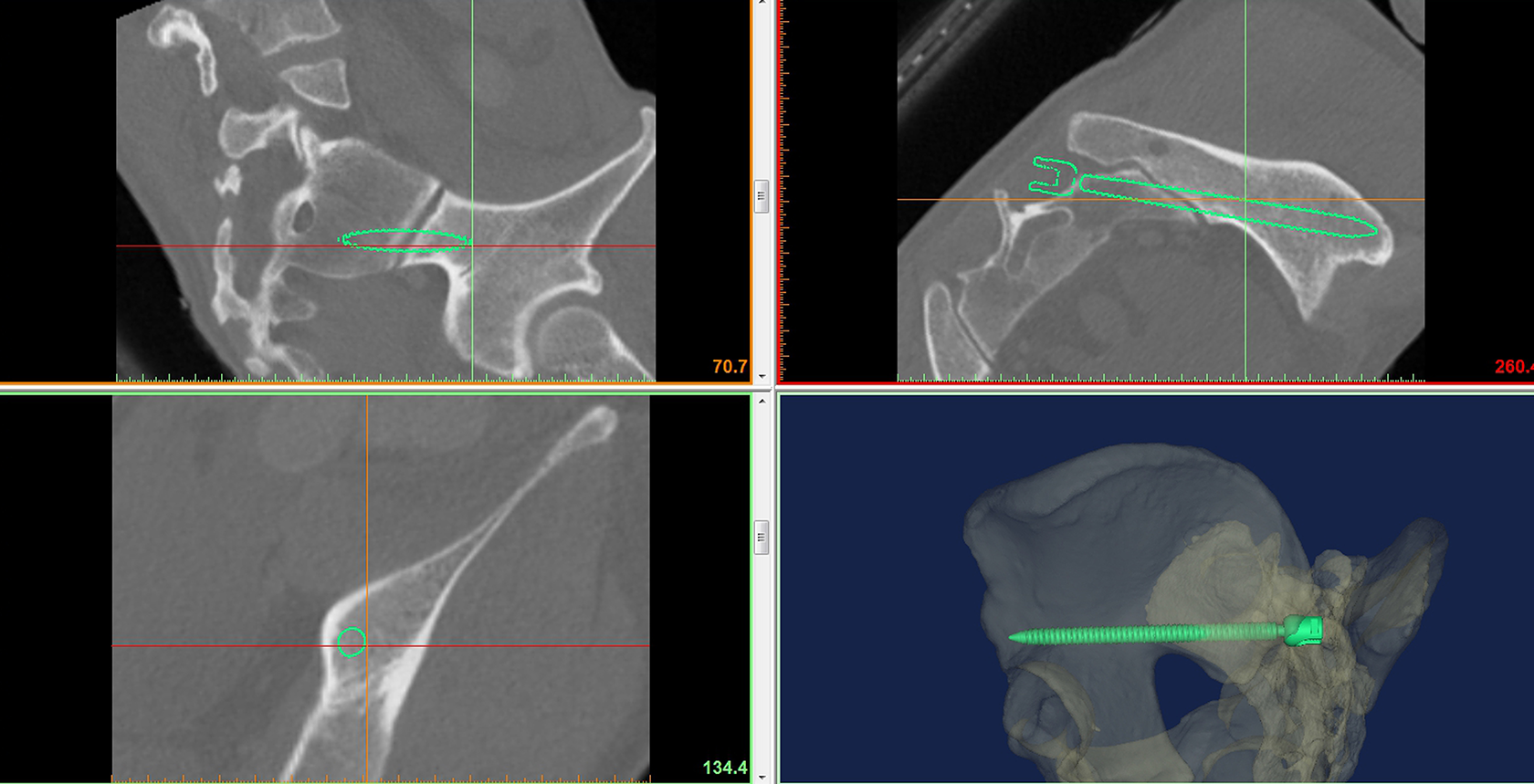
Using the Mimics® software, a virtual S2AI screw was ideally placed in the 3-D pelvis model via four synchronized windows composed of axial plane, coronal, sagittal, and 3-D biplanar images. S2AI: sacral-alar-iliac.
All measurements are presented as mean and range or binary variables including the possibility of S2AI screw. Two sample t-tests were used to compare differences between groups based on the variables. The statistical analyses were performed using the SPSS statistical software package for Windows version 20.0 (SPSS Inc., Chicago, Illinois, USA). Values of p < 0.05 were statistically significant.
Ethics approval and consent to participate
All authors read and agreed with the editorial policy. This study design was approved by appropriate ethics review boards.
Results
None of the models was impossible for S2AI screw fixation owing to the cortical violation along the entire screw path. The average length of intraosseous screw path was an average 99.8 mm (range, 59.8–115 mm; SD, 16.1; Table 1). The only one was assigned as short model and had the length of 59.8 mm. All screws exited around the AIIS in the iliac oblique view, and 10 models had acetabular perforation of screw tip. Computational simulation indicated that the entry point had a relatively wide tolerance in the area between first and second dorsal sacral foramen, once the screw trajectory was no greater than 5 mm from the superior rim of greater sciatic notch in the iliac oblique view (Figure 2). In the pelvic inlet view, none of the S2AI screw violated the linea terminalis and directed at the AIIS approximately. Verification after removal of the iliac bone on the same side showed that the cortical purchase of sacrum was maximal without the violation of nerve root canal based on the entry point in line with two dorsal sacral foramina (Figure 3). The degree of sacral osseous anchorage was verified by visualizing the modified inlet view, which was vertical to the iliac bone, compared with the conventional inlet view (Figure 4). The modified inlet view also facilitated the central location of the screw in the iliac bone, and the trajectory was directed to the middle of acetabulum.
Descriptive data and correlation of S2AI screw length between variables.
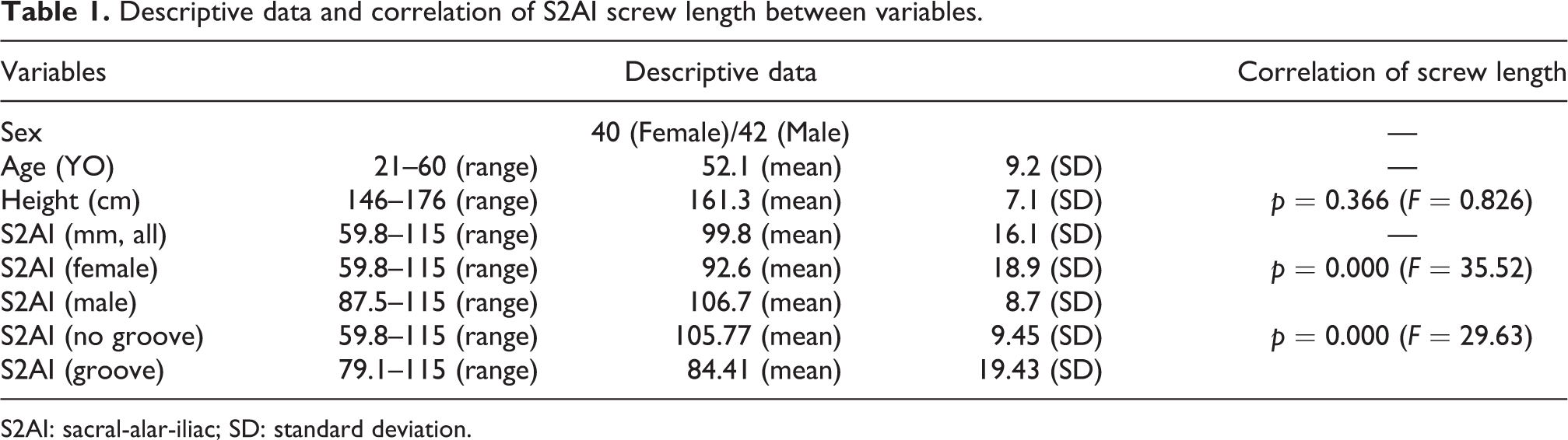
S2AI: sacral-alar-iliac; SD: standard deviation.
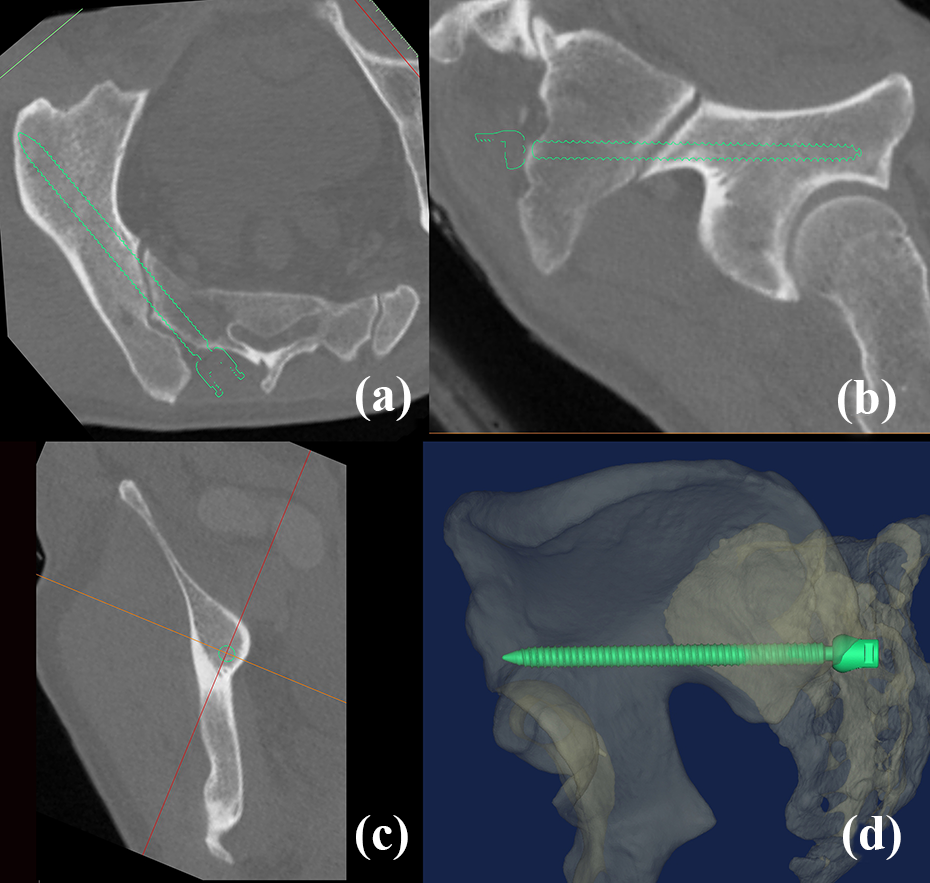
Based on the reformatted CT scanning plane parallel to the ideal S2AI screw, (a) the safe corridor for S2AI screw was relatively wide in the axial view. (b) The screw was placed immediately above the superior rim of greater sciatic notch. (c) The ideal screw was placed in the cancellous bed in the coronal view, without violating the cortex. (d) The 3-D biplanar image shows the entire path of S2AI screw. S2AI: sacral-alar-iliac; CT: computed tomography.

The ideal entry point of S2AI screw had a wide tolerance between first and second dorsal sacral foramen and was in line with two dorsal sacral foramina. S2AI: sacral-alar-iliac.

(a) Fluoroscopic modified inlet view vertical to the iliac bone shows the sacroiliac joint and the entire corridor of S2AI screw. (b) The screw was centrally located in the iliac bone through the modified inlet view and the trajectory was directed to the middle of acetabulum. S2AI: sacral-alar-iliac.
The factors limiting the intraosseous S2AI screw length were sex (p = 0.000) and iliac groove around the SI joint (p = 0.000). The average length of male was 106.7 mm (SD 8.68) and female, 92.6 mm (SD 18.8). The iliac grooves were found in 23 models and inevitably tilted the screw in an outward direction (Figure 5). The model without iliac groove was an average 105.77 mm (SD 9.45) in length and the model with iliac groove, 84.41 mm (SD 19.43). The exits of models with iliac groove were located at the iliac tubercle just above the greater sciatic notch. By simulating the intentional malposition in the horizontal direction, the medially shifted trajectory induced the cortical perforation around the iliac side of the SI joint, which was identical to the site of iliac groove. If laterally shifted, the screw tip penetrated the cortex at the iliac tubercle (Figure 6). Thus, the trajectory was the most important factor determining the adequacy of intraosseous length of S2AI screw, because the entry zone was relatively tolerant in the area between the first and second dorsal sacral foramen. Once the S2AI screw was placed at the nearest trajectory to the greater sciatic notch, there was no significant risk of neurovascular complications occurred related to malposition.

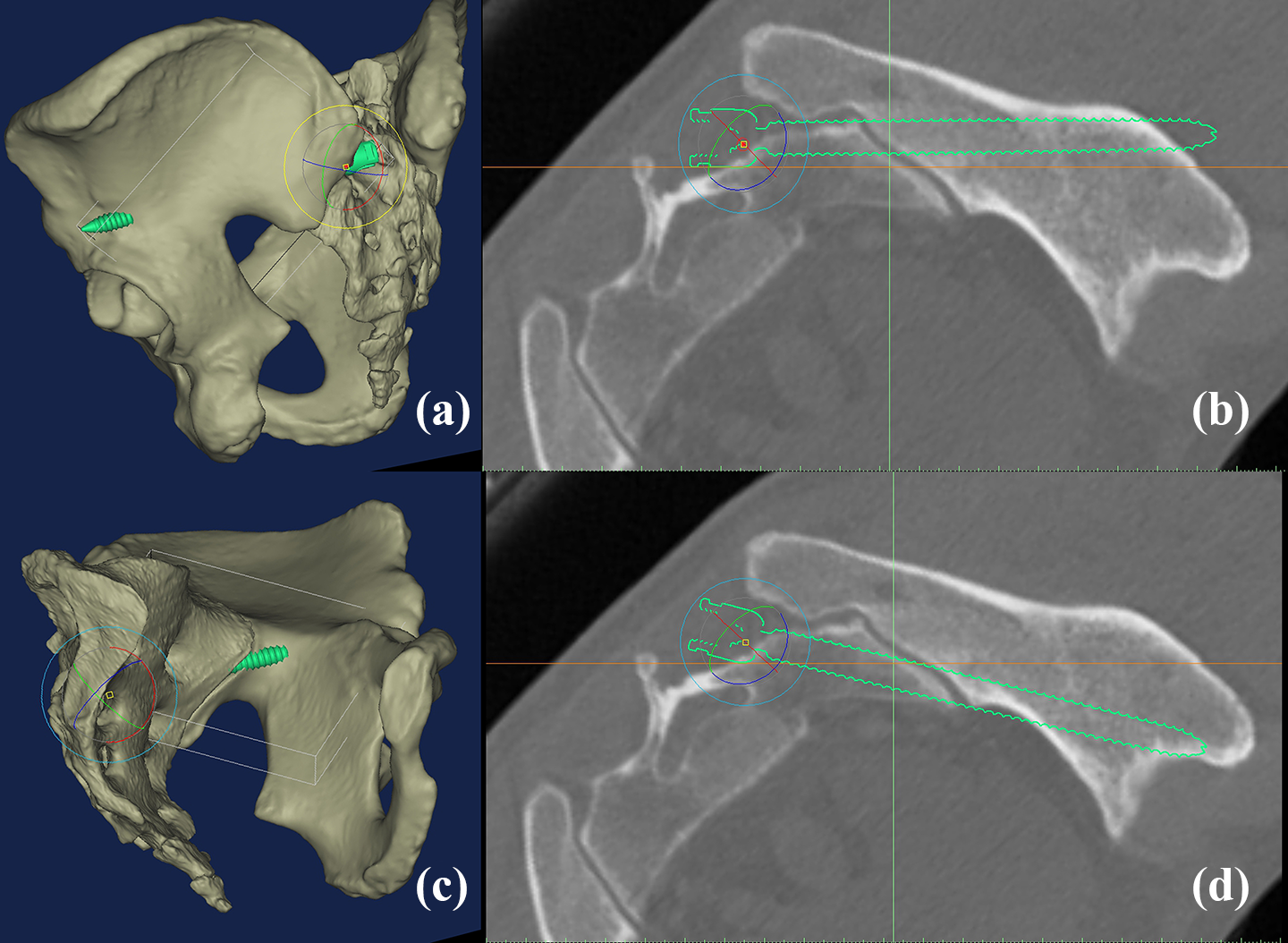
Through the reformatted CT scanning plane parallel to the S2AI screw, (a) the conventional screw trajectory violating the cortex around the iliac groove was clearly identified. (b) To prevent cortical violation, S2AI screw should be directed outward. (c) If the trajectory was not modified, the screw was exposed around the iliac groove. S2AI: sacral-alar-iliac; CT: computed tomography.
Simulation of the intentional malposition in the horizontal direction (a and b) The medially shifted trajectory caused cortical perforation around iliac tubercle. (c and d) If medially shifted, the S2AI screw induced cortical perforation around iliac side of SI joint, which was identical to the site of iliac groove. S2AI: sacral-alar-iliac.
Discussion
Since the clinical utility of S2AI screw is well known based on several advantages including the lower profile construct and biomechanical strength, 1 –4,11 it has gradually replaced the conventional iliac screw in the spinopelvic fixation. However, despite the benefit in pelvic fixation, S2AI screw fixation remains a challenge for orthopedic trauma surgeon when compared with the iliac screw fixation. The challenge might be related to feasibility and safe osseous corridor. Therefore, using this computational simulation of S2AI screw fixation with intentional malposition, we investigated the ideal entry point and screw trajectory and introduced the surgical landmark for fluoroscopic procedure. Through this study, we could summarize it for convenient and safe placement. (1) Because the optimal entry point had a wide tolerance range, the S2AI screw trajectory was the most important for fixation no more than 5 mm from the superior rim of greater sciatic notch in the iliac oblique view to obtain sufficient screw length. (2) The linea terminalis was not violated in the pelvic inlet view, and the screw trajectory was directed around AIIS. (3) The iliac groove around SI joint should be preoperatively identified by 3-D reconstruction image or the manipulation of CT scanning plane, since it interfered the sufficient intra-iliac screw length. (4) The modified inlet view was useful for identifying the lateral shift of entry point and insertion through lateral edge of SI joint.
In recent years, several anatomical studies 5,6,8 –10 of various optimal entry points and trajectories of S2AI screw used CT images. Most of them manipulated the CT imaging plane to match the screw trajectory for measuring the greatest intra-iliac length. 6,8 –10 O’Brien et al. 5 conducted CT scan of cadaveric specimens, which were fixed with S2AI screw. Although a few differences existed in the entry points, the screw length of CT imaging study (an average 110 mm) was greater than the cadaveric study (average 84 mm). This point may suggest significant discrepancy between CT image–based study and actual surgery. In this virtual fixation using the Mimics® software, the osseous corridor for S2AI screw was relatively wide to accommodate sufficient length exceeding 65 mm, in the absence of iliac groove. The screw length of models with iliac groove was an average 84.4 mm and was significantly shorter than in models without iliac groove, which was an average 105.8 mm (p = 0.000). To the best of our knowledge, our study was the first of its kind to determine that the iliac groove should be preoperatively identified as the obstacle to achieve the sufficient screw length. Considering that there was just one short model, despite the iliac groove, the S2AI screw trajectory based on the optimal entry point might be a key step. We also identified the narrowest zone of osseous corridor of acetabulum, which influences the screw trajectories to be fixed (Figure 7). In measuring the safe osseous corridor of S2AI screw three-dimensionally, we could not overcome the issue of technical details when using the Mimics® software because of its complex plane. However, it could be found that the key anatomical structures at risk of being perforated due to malposition were the inner iliac surface around SI joint. Once trajectory was placed over the greater sciatic notch and in the iliac bone. The optimal screw trajectory could be determined intraoperatively by the modified inlet and iliac oblique view.

The key anatomical structures at risk of being perforated due to malposition were verified by placing the 12-mm-diameter cylinder around S2AI screw. The most dangerous part was the area of linea terminalis around SI Joint. S2AI: sacral-alar-iliac; SI: sacroiliac.
In the original technique, 4 –6 the ideal screw trajectory was angled approximately 40° laterally and 40° caudally, based on the CT imaging study. Unless surgical navigation was used, it was very difficult to determine whether the screw trajectory was optimal or not. Practically, most surgeons performed the S2AI screw fixation as a fluoroscopic procedure based on the surgeon’s knowledge of pelvic anatomy. Therefore, this study did not measure the angle of ideal screw trajectory. During fluoroscopic procedure of S2AI screw placement, it was important that the target points and fluoroscopic landmarks to control the screw trajectory were well visualized. We reemphasized the importance of greater sciatic notch and AIIS even though they were already well known. In the iliac oblique view, the screw trajectory was directed toward AIIS and passed just over the superior rim of greater sciatic notch. In pelvic inlet view, the screw tip should also point toward the AIIS without involving the linea terminalis, if there was no iliac groove. When considering that a more anterior trajectory often resulted in a longer screw, the modified inlet view might be so useful to prevent the intrapelvic penetration, since the S2AI screw was centrally located in the iliac bone and the trajectory was directed to the middle of acetabulum and the intra-iliac position of screw was better visualized compared with the conventional inlet view.
Studies reported subtle differences in opinion on the entry point of S2AI screw. 2,5,6,9,10 Yamada et al. 8 reported that the entry point at 2-mm medial to apex of lateral sacral crest on the midline between S1 and S2 dorsal foramen was selected. Lee et al. 10 proposed that the insertion started from the point in which the midline between the first and second posterior sacral foramina met the lateral sacral crest. Zhu et al. 9 selected the entry point on the images of the 3-D CT reconstruction at 1-mm inferior and 1-mm lateral to the first dorsal sacral foramen. In this computational simulation study, no cortical violation occurred in any point between the first and second dorsal sacral foramina once the screw trajectory was directed to the AIIS over the greater sciatic notch. In addition, the pilot hole showed a tendency to push laterally and eccentrically enlarge it to the lateral side. The starting point is determined based on three factors: (1) connectivity with cephalad instrumentation without connecting rod, (2) the intentional medial shift of entry point, and (3) the height of entry point over the superior rim of greater sciatic notch. Based on our results, we recommend the medial shift entry point, which had several advantages including sufficient sacral osseous anchorage across the SI joint and percutaneous insertion without deep dissection to identify the first sacral foramen.
However, our computational analysis has several fundamental limitations. First, all measurements were performed from normal pelvis using manual methods and the cortical expansion around screw was not considered. Second, because the soft tissue of posterior sacrum and deformities due to sacral fracture could not be considered, there might be significant discrepancy between our virtual placement and actual surgery. Thus, our results may have a rather descriptive character compared with clinical studies. Despite these limitations, our demonstration based on computational simulation had several strengths. First, this simulation at actual size not only reaffirmed the usefulness of well-known landmarks but also enabled us to improve 3-D understanding about safe screw corridors. Our findings of entry point and screw trajectory will facilitate the fluoroscopic procedure of S2AI screw fixation, either open or percutaneous. Second, our findings of iliac groove are valuable for understanding the associated anatomy and implications of S2AI screw fixation, because there was a large change in the intra-iliac screw length with a slight shift on the horizontal plane in a groove model. Third, although this research was not based on clinical techniques and outcomes, it might be able to directly suggest technical relevance to minimize intraoperative complications associated with screw malposition.
Conclusion
Our computational simulation revealed that the ideal entry point of S2AI screw showed a wide range of tolerance between the first and second dorsal sacral foramen, obviating the need for deep dissection to determine the first dorsal sacral foramen. Considering the tendency to shift the pilot hole laterally and the ideal screw trajectory was consistently directed toward AIIS, it is better that the entry point is located with a medial shift to the extent possible for connection with cephalad instrumentation.
Footnotes
Authors’ Note
All data analyzed during this study are included in this published article.
Authors’ Contributions
Jeong designed and analyzed data as a first author. Jung was a major contributor in writing the manuscript as a corresponding author. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.