
Abstract
Background:
Plate fixation using traditional lateral L-shape approach for intra-articular calcaneal fractures is complicated by 30% of wound complications, and the lateral small incision techniques with a tarsal sinus approach cannot sufficiently address all the fragments. A modified tarsal sinus approach with combined advantages of traditional lateral L-shape and tarsal sinus approaches for the treatment of intra-articular calcaneal fractures was developed.
Method:
This prospective study included 29 patients (13 Sanders type II and 16 type III) with calcaneal fractures were managed with this technique. Calcaneal height, width, length, Bohler’s angle, and Gissane angle were measured preoperatively, postoperatively, and at 1-year follow-up. Functional outcomes were assessed based on American Orthopedic Foot and Ankle Society (AOFAS) ankle/hindfoot score.
Results:
Twenty-nine patients with average follow-up time of 18 (range 13–29) months were included. The radiographs demonstrated significant corrections of the Bohler’s angle and Gissane angle, calcaneal width, length, and height from preoperation to postoperation and 1-year follow-up. Among all follow-up patients, one case had skin necrosis but healed after dressing. Another case had symptoms of numbness in the sural innervation area, which disappeared after 5 months of physical therapy and drug therapy. One case showed degenerative changes of subtalar joint at 1-year follow-up. No other wound complications like incision infection (superficial or deep) and wound dehiscence occurred. At 1-year follow-up, the mean AOFAS score was 90.2 ± 17.7 (range 70–98) and the good and excellent rate was 89.7%.
Conclusion:
The modified tarsal sinus approach in the treatment of Sander’s type II and III calcaneal fractures allowed adequate reduction and rigid fixation with low incidence of wound complications. Compared to sinus tarsi approach, this technique required shorter learning curve and was more easily mastered by young orthopedic surgeons. Thus, it was worthy of application clinically.
Keywords
Background
The extended lateral L-shaped approach is commonly used for the treatment of calcaneal fractures. This approach accurately reduces the subtalar joint, fully exposes, and addresses the intra-articular calcaneal fragments and conveniently places the plate to achieve a stable fixation. 1 However, the wound complications’ rates were reported to be as high as 30%, including delayed wound healing, infection, dehiscence, and flap necrosis. 2 Thus, many minimally invasive techniques have been developed, and sinus tarsi approach being the most commonly used. 3 –5 This approach starts from the tip of the lateral malleolus in a straight line toward the base of the fourth metatarsal, mainly exposing the posterior facet and the calcaneocuboid joint. Due to much smaller incisional design and no damage to the blood supply of the calcaneal lateral flap, this technique effectively reduces the complications associated with soft tissue and achieves good clinical efficacy. 6 However, this technique has problems, such as poor visualization, inadequate reduction, and unreliable fixation, limiting its use in the management of simple calcaneal fractures. 7 Besides, a rich surgical experience is required for this technique, especially when addressing the complex intra-articular calcaneal fractures, and thus this technique is hard for young orthopedic surgeons. Therefore, designing a modified approach combined with the advantages of traditional L-shape and sinus tarsi approaches to effectively avoid soft tissue complications and to provide wide visualization and rigid fixation has practical significance.
Therefore, we designed a modified sinus tarsi approach that is located more distally to the tip of the lateral malleolus along the calcaneal axis and extended from the base of fourth metatarsal to 1 cm anterior of Achilles tendon. This approach not only protected the blood supply of lateral calcaneal flap but also provided wide exposure of the anterior processes, calcaneocuboid joint, posterior facet, lateral wall of calcaneus and three-fourth region of calcaneal tuberosity. Besides, any plate (including traditional plates used during the traditional L-shape approach) could be placed using our modified sinus tarsi approach to acquire rigid fixation. Because of its more wide exposure similar to that of lateral L-shape approach, this approach could be easily acquired by young orthopedic surgeons. Hence, in the present study, we evaluated the outcomes of calcaneal fractures after open reduction and internal fixation through modified sinus tarsi approach.
Methods
This was a level IV prospective analytical study performed from May 2014 to April 2016. A total of 29 patients (24 males and 5 females) of intra-articular calcaneal fractures (Sander’s type II and III calcaneal fractures) were treated with open reduction and internal fixation through a modified sinus tarsi approach. Inclusion criteria included patients of Sander’s type II and III calcaneal fractures ages 18–75 years. Exclusion criteria include Sander’s type I and IV fractures, open calcaneal fractures, and those with age <18 and >75 years. All the surgeries were performed by Dr Zhan Junfeng (an orthopedic resident). All patients had anteroposterior, lateral, and axial X-ray views of both injured and normal calcaneus; also, a CT scan of the fractured site to classify the fracture patterns.
Of the 29 patients, one had a fracture in a traffic accident and rest of them were due to fall from height. All fractures were unilateral, with left side involvement in 16 cases and right side in 13 cases. According to Sanders CT scan classification system, there were 13 cases with type II (5 type IIA, 6 type IIB, and 2 type IIC) and 16 with type III (6 type IIIAB, 6 type IIIAC, and 4 type IIIBC). In addition, the lumbar vertebral or thoracic vertebral fracture was complicated in four cases, tibial plateau fracture in two cases, femoral neck fracture in two cases, and ankle fracture in one case. Fourteen patients had >5 years smoking history, and five patients had a history of excessive consumption of alcohol, and they were advised to stop smoking and abstain from alcohol until wound healing. Two other patients had diabetes, and their blood glucose levels were controlled to prevent further complications. This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Nanfang hospital, Southern Medical University. Written informed consent was obtained from all participants.
Surgery
All patients were administered with continuous epidural anesthesia or general anesthesia. All of them were operated in supine position. The brief steps of the operation were as follows: (1) Incision: Firstly, the lateral malleolus, the fifth metatarsal base, and sural nerves were marked. Then, a transverse incision was made 1.5 cm distally to the tip of the lateral malleolus along the calcaneal axis; starting from the base of fourth metatarsal to 1 cm anterior of the Achilles tendon (Figure 1(a)). The incision crossed over the peroneus longus, and brevis tendon sheath and sural nerve require separation and protection in this approach (Figure 1(b)). We defined the operation visual field by peroneus tendon sheath boundary as the anterior window (the one anterior of the peroneus tendon sheath) and posterior window (the one posterior to tendon sheath; Figure 1(c)). (2) Field exposure: With the posterior traction of the peroneus tendon sheath can expose the anterior window that includes the anterior process, the calcaneocuboid articular and posterior facet (Figure 1(d)). By partly cutting the calcaneofibular ligament, posterior facet and collapsed fracture blocks were completely exposed (Figure 1(e)). To explore posterior window, we anteriorly retract the peroneus tendon sheath and use a Hoffmann retractor to retract soft tissue posteriorly; this window exposes body of the calcaneus and three-fourth region of the anterior tubercle of the calcaneus (Figure 1(f)). (3) Fracture reduction: A large Steinmann pin placed into tuberosity fragment directed posteriorly to correct the Varus loss of height and length. Once the tuberosity was reduced, place a Kirschner wire posterolateral from tuberosity into the medial sustentaculum tali to provide provisional fixation and checked under a fluoroscope to confirm fixation. Then, through the posterior window, the lateral wall was dissected from the calcaneal body and removed. A periosteum elevator was used to displace the posterior facet fragment through the medial fracture line. Later the articular surface is also checked; if not, reduce it through the anterior window and provide a provisional fixation by Kirschner wire underneath the posterior facet and into the sustentaculum tali from the lateral to the medial side. (4) Plate fixation: Once a satisfied reduction was obtained and take an intraoperative axial view to confirm neutral alignment before application of the plate, then apply a lateral plate that extends from the anterior process of calcaneus into the most posterior aspect of tuberosity through the anterior window (Figure 1(g)). The wound was closed (Figure 1(h) and (i)).
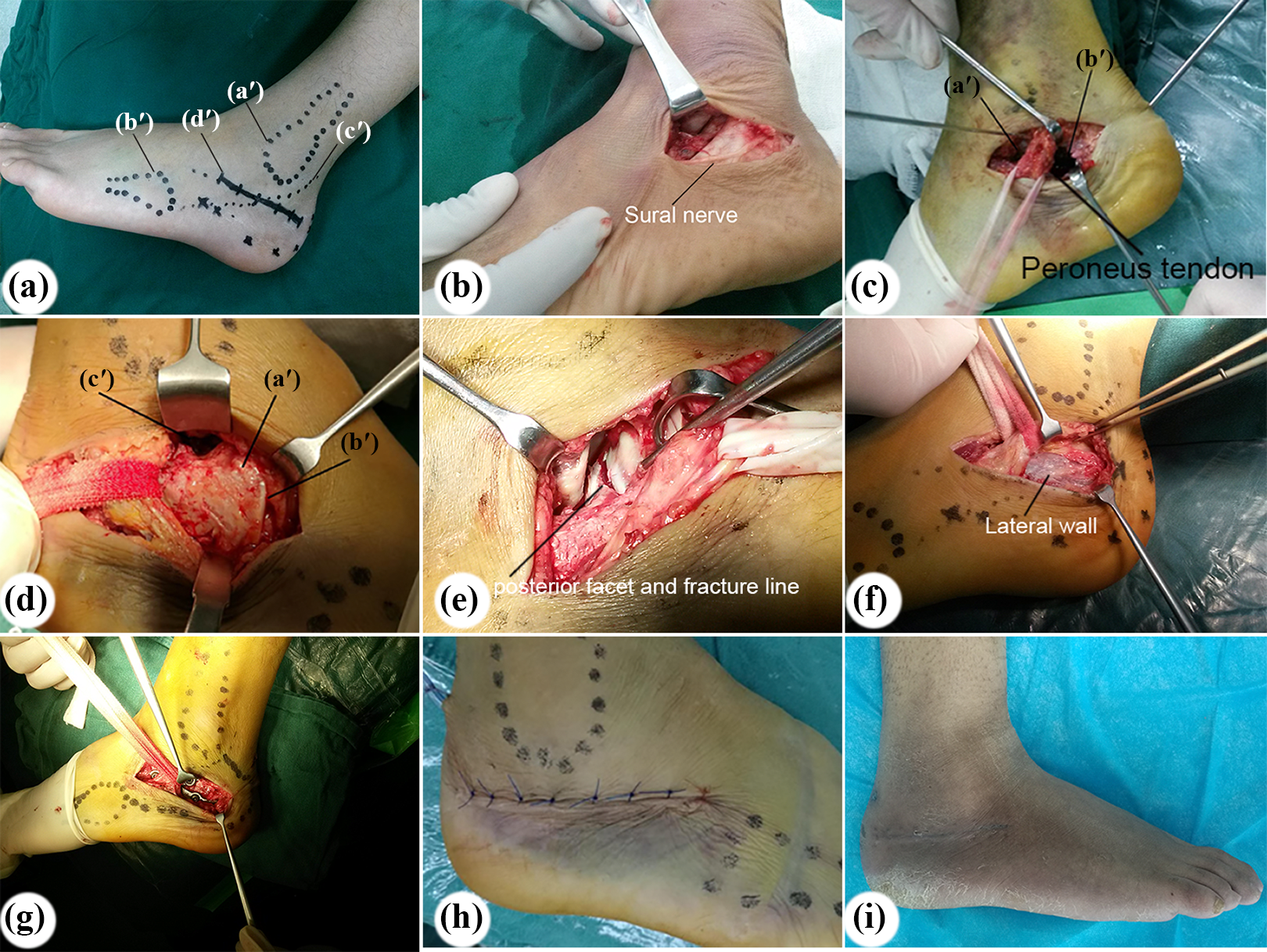
(a) The skin incision. (a′) lateral malleolus, (b′) the fifth metatarsal, (c′) sural nerve, and (d′) incision marker. (b) Sural nerve was separated and protected. (c) The operation visual field was separated into double operative fields by peroneus tendon sheath. (a′) the anterior window and (b′) the posterior window. (d) With posterior traction of the peroneus tendon sheath, the anterior process (a′) the calcaneocuboid articular (b′) and posterior facet (c′) were exposed in the anterior window. (e) By partly cutting off the calcaneofibular ligament, posterior facet and collapsed fracture blocks were completely exposed. (f) With anterior traction of the peroneus tendon sheath, the lateral wall of the calcaneus and three-fourth region of the calcaneal tuberosity were exposed in the posterior window. (g) A neutralization plate was easily placed on the lateral wall through the anterior window. (h) The skin was sutured. (i) Incision scar at 4-week follow-up visit.
Postoperative treatment
Postoperatively, the prophylactic antibiotics were given to prevent operative site infections. On the postoperative 3rd day, the patients began to perform ankle dorsal flexion function exercise. At week 4 after operation, partial weight bearing was encouraged. Full weight bearing was allowed until the signs of bone union were observed on the radiograph at weeks 10–12 postoperatively.
Anteroposterior, lateral, and axial radiographs were also obtained postoperatively at 1, 3, 6, 12 months, and at the latest follow-up period. American Orthopaedic Foot and Ankle Society (AOFAS) ankle/hindfoot score was calculated at 1-year follow-up for all the cases.
Statistical analysis
Statistical analysis was carried out using SPSS19.0 software (SPSS, Chicago, Illinois, USA). Data are presented as means ± standard deviation (SD). Preoperative, postoperative, and the last follow-up variables were compared using Student’s paired t test. p < 0.05 was considered to be statistically significant difference.
Results
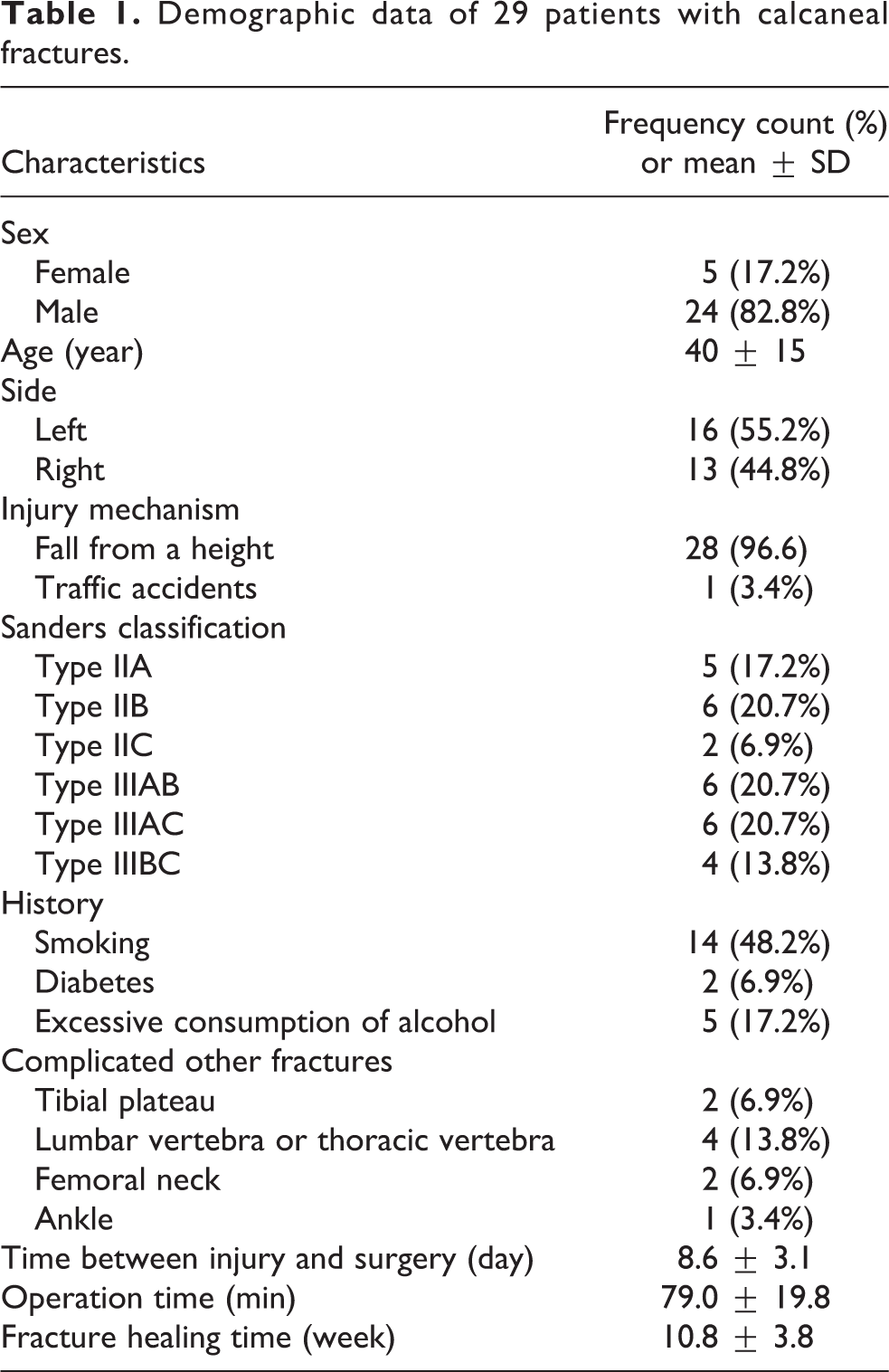
The average follow-up period of 29 patients was 18 (range, 13–29) months, and the average age of the patients was 40 ± 15 (range 18–60) years. The average time between injury and surgery was 5.6 ± 3.4 (range 1–9) days. The operation time was 79 ± 20 (range 58–100) min. The average fracture healing time was 11 ± 4 (range 9–15) weeks (Table 1).
Demographic data of 29 patients with calcaneal fractures.
The lateral and axial radiographs of the calcaneus showed good reduction and fixation, and significant corrections of the Bohler’s angle, and Gissane angle, calcaneal width, length, and height from preoperation to postoperation and 1-year follow-up (p < 0.01). However, there were no significant differences in the variables between postoperation and 1-year follow-up (Table 2). Among all the follow-up patients, one case (3.4%) had skin necrosis and healed after dressing. Another case (3.4%) showed symptoms of numbness in the area of sural innervation, which disappeared after 5 months of physical therapy and drug therapy. One case (3.4%) showed degenerative changes of subtalar joint at 1-year follow-up. No other wound complications such as incision infection (superficial or deep) and wound dehiscence occurred (Table 3).
Radiological results before and after operation.a

aThere was no statistical difference between the postoperative group and the last follow-up group.
b p < 0.01: compared with the preoperative group.
Complications after surgery.

At 1-year follow-up, the mean AOFAS score was 90.2 ± 17.7 (range 70–98), which was excellent in 20 cases, good in 6 cases, and fair in 3 cases, and the good and excellent rate was 89.7% (Figure 2 and Figure 3).

(a) Schematic representation of the surgical incision for calcaneal fractures. Tarsal sinus approach: an incision of 4–5 cm length is made from the tip of the lateral malleolus to the level of the calcaneocuboid joint in a straight line toward the base of the fourth metatarsal. Modified tarsal sinus approach: a transverse incision is made 1.5 cm distally to the tip of the lateral malleolus along the calcaneal axis, starting from the base of fourth metatarsal to 1 cm anterior of Achilles tendon. Extended L-shaped approach: the posterior arm of the line is placed in between the Achilles tendon and the posterior margin of the fibula, parallel to the longitudinal axis of the limb. The horizontal arm of the line is extended to the base of the fifth metatarsal, parallel to the plantar surface. (b) Schematic view of anterior window of modified tarsal sinus approach. (1) Collapsed posterior facet, (2) anterior process, (3) talus, (4) calcaneocuboid joint are visualized through the anterior window. (c) Schematic view of the posterior window of modified tarsal sinus approach. Lateral wall of calcaneal and three-fourth region of calcaneal tuberosity are visualized through the posterior window.

Preoperative lateral (a) and axial (b) radiographs showing an intra-articular calcaneal fracture in a 37-year-old man who had fallen from a height. Preoperative computed tomography images (c and d) showing a Sanders IIAB fractures with a bulked lateral wall. Postoperative lateral (e) and axial (f) radiographs showing anatomical restoration of the subtalar joint.
Discussion
The surgical treatment effects of calcaneal fracture vary with the surgical approach and operative methods and the incision complications directly affected the clinical results. Previously, the extended lateral L-shaped approach has been widely used for plate fixation of calcaneal fractures and 60–85% of cases showed satisfactory clinical outcomes; however, it is accompanied by high risk of soft tissue complications. 1 This approach devascularized the central and anterior part of the calcaneal lateral wall, as 45% of the total blood supply of the calcaneus enters from this site. 8 Soft tissue complications reached 11–24.6%, leading to a serious impact on the treatment of calcaneal fractures. 9 To solve the soft tissue complications related to extended lateral L-shaped approach, several lateral minimally invasive techniques with sinus tarsi approach for treating calcaneal fractures were developed. 3,4,10 Although the soft tissue problem has been minimized with the use of these techniques, issues of poor visualization, inadequate reduction, and unreliable fixation should be addressed. 11 Thus, we developed a modified approach by combining the advantage of wide surgical field of extended lateral L-shaped approach and the advantage of soft tissue protection of sinus tarsi approach.
According to the previous reports, 12,13 the subcutaneous tissues of the lateral hindfoot had two sets of blood supply systems: the above flap was supplied by the lateral calcaneal artery and the lateral malleolar artery, while the tarsal side tissue was supplied by the lateral tarsal artery. The lateral calcaneal artery was proximal to the vertical portion of the traditional L-shaped incision, and it appeared to be the most likely injured site due to inaccurate placement of the incision. Besides, the horizontal incision of traditional L-shaped incision damaged the vascular network from the plantar flap. Thus, if the lateral calcaneal artery was occluded during the injury or suffered iatrogenic injury, it causes lateral flap vascular network destruction, blood supply damage, and soft tissue healing complications. Bibbo et al. used preoperative ultrasound to determine if the lateral calcaneal artery was the main blood supply artery for lateral flap, and lateral calcaneal artery injury was closely related to wound healing complications. 14 In the present study, our modified sinus tarsi approach by taking into consideration that the lateral hindfoot anatomy and blood supply effectively avoided the damage to plantar blood vessels net and protected the lateral calcaneal artery in operation and promised the blood supply of the lateral flap.
In addition, compared to sinus tarsi approach, this modified approach had advantages in surgical field exposure, fracture reduction, and fixation. Due to limited exposure of the posterior facet and calcaneocuboid joint in sinus tarsi approach, the collapsed posterior facet was indirectly reduced through medial distraction technique and for the comminuted fracture of the calcaneal body, the exposure remained insufficient and difficult for the reduction and fixation. Thus, this technique was challenging and required a thorough understanding of the fracture patterns and calcaneal anatomy and should be performed by experienced surgeons. In addition, fixation was achieved by screws, K-wires, or minitype plate via sinus tarsi approach, and this may not provide reliable fixation for comminuted calcaneal fractures, calcaneal fractures with severely compressed articular surface, and osteoporotic fractures in the elderly patients. The visualization of fracture according to our modified sinus tarsi approach was similar to that of the traditional extended lateral L-shaped approach. A wide exposure of anterior process, calcaneocuboid joint, posterior facet, lateral wall of calcaneus, and three-fourth region of calcaneal tuberosity could be obtained via double window in our approach. The reduction and fixation technique was also similar to that of the extended lateral L-shaped approach. Posterior facet and calcaneocuboid joint could be directly visualized through anterior window of our approach, while the posterior facet fragment was visualized through posterior window and was directly reduced after opening the calcaneal lateral wall. Therefore, this technique was easy for beginners to understand and master and did not require longer learning curve. Besides, through the anterior window of our approach, traditional calcaneal plate was easily placed on the lateral wall for rigid fixation of comminuted calcaneal fractures, calcaneal fractures with severely compressed articular surface, and osteoporotic fractures in the elderly patients.
In our study, Bohler’s angle, Gissane angle, calcaneal length, width, and height were significantly improved from preoperation to postoperation after surgery with a p value of <0.01. This indicated that anatomical reconstruction of calcaneal fractures including length, width, height, Bohler’s angle, and Gissane angle could be achieved with open reduction and plate fixation through our modified sinus tarsi approach. Better reduction of the calcaneus may result in the better recovery of foot function. In our study, the mean AOFAS ankle/hindfoot score was 90.2 ± 17.7 (range 70–98), and the good and excellent rate was 89.7%. The time for fracture healing was 10.8 ± 3.8 (range 9–15) weeks. Only one case showed degenerative changes of subtalar joint at 1-year follow-up period. Our results were comparable with the results achieved using other minimally invasive techniques. 11,15
Among all the follow-up patients, only one case (3.4%) had skin flap necrosis but was healed after dressing. Another case (3.4%) had symptoms of numbness in the area of sural innervations, which were disappeared after 5 months of physical therapy and drug therapy. Our results seemed to be superior to the results achieved using sinus tarsi approach. In a systematic review of calcaneal fractures treated with sinus tarsi approach, the average rate of wound complication was 4.8%. 16 Kikuchi et al. reported three cases (13.6%) with superficial wound infections. 4 Kline et al. had wound complications in 29% of the extensile group and 6% of the sinus tarsi group. 17 Che et al. demonstrated that 3 out of 47 cases (6.4%) had minor wound complications, and 7 cases (14.9%) had painful hardware at the posterior calcaneal tuberosity. 18
The incision of our modified sinus tarsi approach was small and the skin flap was not required during the surgery, and thus operation through swollen tissue was less concerned. We performed the operation as early as possible, even in the presence of swelling, without any excessive soft tissue complications. For patients with Sanders type II calcaneal fractures without serious swelling, the operation was performed within 24 h after the fracture. For patients with Sanders type III calcaneal fractures with serious swelling, the operation was performed as earlier as possible from 5 to 9 days after the fracture. The average time interval between the injury and operation was 5.6 ± 3.4 (range 1–9) days in our study, which was a relatively short time interval for surgery.
Our study has several limitations including the small number of cases, the short follow-up time, lack of long-term curative effects, and prospective case–control study design. Therefore, further investigation is necessary to obtain a more precise efficacy evaluation by studying in a larger sample size, longer follow-up time, and a randomized control trial.
Conclusions
In conclusion, compared to the sinus tarsi approach, the modified sinus tarsi approach could obtain wider exposure and provide rigid fixation for Sander’s type II and III calcaneal fractures, limiting the soft tissue complications. Furthermore, compared to the sinus tarsi approach, this technique required short learning curve and can be easily mastered by beginners. Hence, it was worthy of application in clinics.
Footnotes
Authors’ note
The data sets supporting the conclusions of the article are included within the article.
Author contributions
ZJF and HCZ contributed to this work equally as first author. WG, HCZ, and JJH conceived and designed the study and drafted the manuscript. All the operations were performed by ZJF. ZN and FW collected the data and performed the statistical analysis. All of the authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Grants from Shanghai Tenth hospital’s improvement plan for NSFC (SYGZRPY2017021).