
Abstract

Keywords
Introduction
Despite successful surgical fixation of calcaneal fractures, wound complications may be encountered. The presence of preoperative soft tissue damage may further complicate the postoperative recovery. Levin and Nunley discussed the use of the abductor hallucis flap to treat soft tissue defects resulting from calcaneal fractures; however, they discussed this in the context of treating postoperative wound breakdown as opposed to preoperative wounds. 3
The goal of this retrospective study was to assess the success of the abductor hallucis flap with split-thickness skin graft used in conjunction with open reduction internal fixation (ORIF) in a single-stage procedure to treat calcaneal fractures complicated by preoperative medial full-thickness skin necrosis. Our hypothesis was that an abductor hallucis flap would be a viable option for soft tissue coverage to allow ORIF of calcaneal fractures with medial soft tissue defects using a combined medial and lateral approach.
Methods
A retrospective search was performed to identify all patients between 2006 and 2012 who underwent ORIF of a displaced intraarticular calcaneal fracture by a single orthopaedic surgeon. Thirty-six patients were identified, and 10 of those also had associated medial full-thickness skin necrosis and were included in the study. All 10 patients were treated with ORIF by a single orthopaedic surgeon and an abductor hallucis flap performed by a single plastic surgeon in a single-stage procedure. Patients were followed postoperatively for a median of 11.6 (range, 3.8-39.2) months.
The primary outcome measurement was whether the abductor hallucis flap succeeded or failed. This was measured by the presence or absence of dead muscle and skin which was monitored visually and by needle sticks demonstrating bright red blood. Secondary outcome measurements included occurrence of hallux valgus on clinical examination, postoperative infection (defined as erythema, drainage, warmth), skin graft revisions, and radiographic fracture union.
Surgical Technique
Surgery was delayed a median of 21 (interquartile range 18.5-23.5) days for swelling to decrease and skin wrinkles to be observed constituting a positive “wrinkle sign” (Figure 1). The necrotic tissue and zone of injury are excised medially leaving a large defect (Figure 2A and B), which allows exposure of the medial calcaneus (Figure 3A). A direct anatomic reduction of the medial wall is performed with fixation of the sustentacular fragment to the tuberosity (Figure 3B). A lateral sinus tarsi incision allows reduction and fixation of the posterolateral and anterior fragments (Figure 3C and D).

Calcaneal fracture with medial full-thickness skin necrosis showing a positive “wrinkle sign.”

(A) The medial incision and area of full-thickness skin necrosis is outlined. (B) Wide excision of the zone of necrosis is performed exposing the medial calcaneal wall and fracture.

(A) A Steinmann pin is placed through the calcaneus to assist with the reduction. (B) A locking titanium hindfoot plate is applied to the medial wall once fracture reduction is achieved. (C) A small sinus tarsi incision technique is used laterally with reduction stabilized with Kirschner wires. (D) A titanium locking plate is applied to the lateral wall for a dual-locking plate construct.
Dissection of the abductor hallucis is then begun (Figure 4). A nonabsorbable suture is used to stabilize the great toe metatarsophalangeal joint to prevent valgus deformity. The dissection of the muscle is continued proximally and then folded posteriorly, filling the void from the excised necrotic tissue and covering the medial plate (Figure 4C and D). A split-thickness skin graft, taken from the ipsilateral thigh, is applied over the abductor hallucis flap (Figure 5). The vascular supply to the abductor hallucis from the medial plantar artery is shown in Figure 6.

(A) A longitudinal incision for dissection of the abductor hallucis is outlined. (B) The abductor hallucis muscle is exposed. Dissection of the abductor hallucis is (C) carried proximally and (D) folded posteriorly to provide soft tissue coverage in the area of the medial wound and overlying the medial calcaneus.

Split-thickness skin graft and closure of the flap donor site.
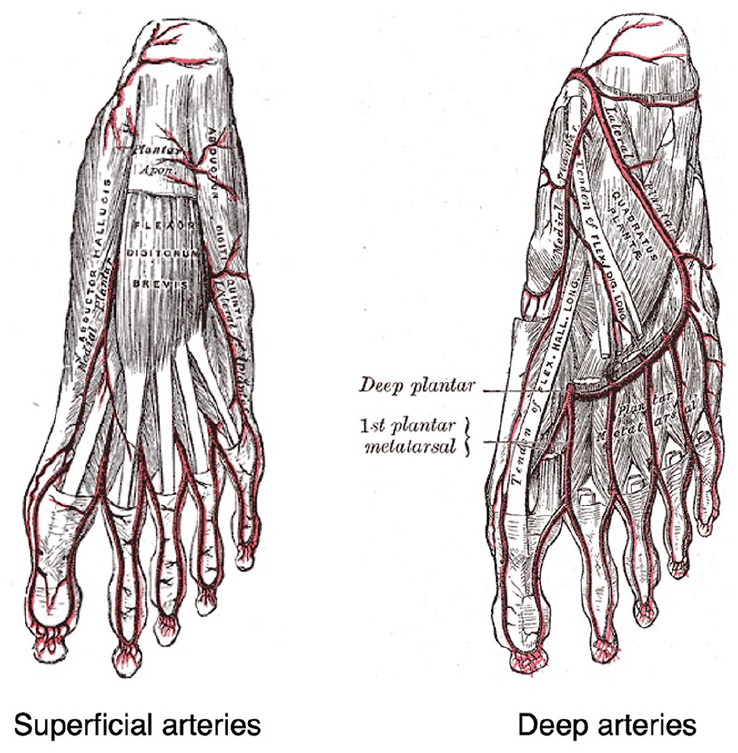
Plantar arteries of the foot including medial plantar artery supplying the abductor hallucis.
Results
Of the 10 abductor hallucis flaps performed, 9 succeeded. Two patients with immersions of their casts in water required skin graft revisions, but the muscle flaps remained viable. There were no postoperative infections, occurrences of hallux valgus, or functional impairments of the great toe. One patient had a nonunion confirmed by CT and was lost to follow-up. Patient characteristics, time to surgery, fracture classification, and outcomes are shown in Table 1.
Patient Characteristics, Fracture Classification, and Outcomes.

The only patient with a flap failure was noted at 21 days postoperatively. He had a Sanders IV depression fracture that was severely displaced and comminuted and necessitated a primary subtalar arthrodesis in addition to ORIF during the index surgery. The patient had a successful revision flap performed by the initial plastic surgeon using a medial plantar fasciocutaneous flap. The fasciocutaneous flap is perfused by cutaneous branches of the medial plantar artery independent of the muscular branches to the abductor hallucis.
Discussion
Soft tissue compromise can be encountered in calcaneal fractures, which may include blistering, present in 15% to 21% of calcaneal fractures,5,6 and subsequent full-thickness skin necrosis. Kwon 2 describes the “almost open” calcaneal fracture in which there is significant medial soft tissue injury due to the spike of the sustentacular fragment which is driven into the soft tissue. This is associated with significant contusion, ecchymosis, or fracture blistering medially, which is indicative of a significant soft tissue injury. Axial heel radiographs and CT scans may show medial bony displacement and impingement over the very thin medial heel soft tissue envelope and may indicate impending soft tissue necrosis. 2
Performing an ORIF and pedicle flap in a single-stage procedure for calcaneal fractures with soft tissue compromise has many benefits. The treatment for full-thickness skin necrosis often involves excision followed by soft tissue reconstruction. If done at the time of ORIF, it can be used as a window of opportunity for improved fracture reduction. The defect left from excising the necrotic tissue provides greater exposure of the fracture site medially, which allows for direct visualization and anatomic reduction of the medial wall and a small incision technique laterally avoiding large lateral skin flaps. The benefits of dual fixation using a combined medial and lateral technique have been described previously.1,4 This technique may be especially applicable in the setting of medial soft tissue defects where the medial wall is directly accessible after debridement.
In addition, using the abductor hallucis flap to fill the medial soft tissue defect may enhance blood flow to the area to better facilitate healing, and it also allows for tension-free closure.
Weaknesses of this study include the retrospective design, small sample size, lack of comparison group, and no functional outcome measures.
Conclusion
Medial full-thickness skin necrosis with an associated calcaneal fracture is a difficult problem to treat. Utilization of an abductor hallucis flap may be a viable option to address the soft tissue defect, and if performed in a single-stage procedure can aid ORIF. This approach can provide an opportunity to expose the medial calcaneus and to directly reduce the medial wall providing stable fixation at the same time as adequate soft tissue coverage.
Footnotes
Ethical Approval
Ethical approval was not sought for the present study as this was a retrospective case series.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.